Double Defibrillation
- Article Author:
- Mark Ramzy
- Article Editor:
- Patrick Hughes
- Updated:
- 7/31/2020 2:30:44 PM
- For CME on this topic:
- Double Defibrillation CME
- PubMed Link:
- Double Defibrillation
Introduction
Double external defibrillation (DED) is the application and administration of transthoracic electrical currents from two defibrillator devices to a single patient experiencing a single type of lethal dysrhythmia during cardiac arrest, known as refractory ventricular fibrillation (RVF).[1][2] This use of DED occurs after standard transthoracic electrical current from a single defibrillator have failed to terminate this lethal rhythm. Refractory ventricular fibrillation is defined as ventricular fibrillation that does not convert with three or more single defibrillation attempts.[2][3] The estimated incidence of RVF is 0.5 to 0.6 per 100000 of the population; some authors report that 10 to 25% of cardiac arrest cases could develop RVF or recurrent VF.[3][4][5] Patients who experience RVF during their cardiac arrest have a mortality of up to 97%.[6][7]
Proposed Theories
1) Power Theory
- Studies have shown that higher energy has improved success on subsequent defibrillation.[8][9][10][11] One of the leading theories behind the success of DED is that the administration of more joules during transthoracic defibrillation allows for the conversion of all the myocytes out of RVF. This approach requires the two electrical currents from both defibrillator devices to be administered at the same time or as close together as possible and is where DED gets one of it’s more common names of “double simultaneous defibrillation” (DSiD).[12][13][14]
2) Setting Up Theory
- Another leading theory behind DED suggests that that the first transthoracic current lowers the defibrillation threshold, which then increases the second transthoracic current’s success at converting any remaining fibrillating myocytes.[1][15] This theory requires a deliberate pause when administering the two electrical currents to ensure they are close together but not delivered at exactly the same time, and is where DED gets its most common name of “double sequential defibrillation” (DSD).
3) Multiple Vector Theory
Indications
Contraindications
Double defibrillation does not have any relative or absolute contraindications. The patient having a pacemaker or implanted automated internal cardiac defibrillator does not change the indication of DED.
Equipment
- Two biphasic defibrillators
- Two sets of defibrillator pads
Personnel
If attempting the power theory; one experienced ACLS qualified healthcare provider is needed to operate both defibrillator devices. If using the setting up theory, then two experienced ACLS qualified healthcare providers are necessary, each operating one of the two defibrillator devices.
Preparation
Begin efforts at obtaining and setting up the second defibrillator if the patient is in ventricular fibrillation and requires a second shock. The placement of this second defibrillator device should be physically close to the first defibrillator, should the two need to be operated by one individual. If the patient was already defibrillated two or more times in the pre-hospital setting, then apply the pads as mentioned below when transferring the patient from the ambulance stretcher to the hospital bed.
- While many defibrillators still have the manual paddles, most manufacturers recommend the use of the adhesive “hands-free” pads. These pads should be the only method of administering DED to ensure adequate delivery of energy and to avoid any operator interference that may occur when using the paddles. Ensure you have the correct size pads on the second defibrillator device before application onto the patient.
Pad Placement
- The first set of defibrillator pads should remain in their original location, one pad along the upper right sternal border and the second at the cardiac apex.
- IMPORTANT: If the pads touch one another, there is a significant risk of damaging one or BOTH defibrillators. Device manufacturers do not cover damage to the defibrillators using DED
There are two location options for placement of the second defibrillator pads:
- The first pad should be immediately medial or lateral to the pad located at the right sternal border without touching that first pad. The second pad should also be placed immediately medial or lateral to the first defibrillator pad located at the cardiac apex and also not touching it
- An anteroposterior placement of the second set of defibrillator pads is also an option. This method is preferred as the pads can easily be applied when transferring patients from pre-hospital stretcher to hospital bed. Furthermore, there is less risk of the pads touching and damaging the defibrillator devices.
Technique
If attempting DED simultaneously using the power theory then it is recommended that a single healthcare provider operate both defibrillator devices to ensure the administration of is as close together as possible
If attempting DED sequentially using the setting up theory, then it is recommended that two healthcare providers each operate a single defibrillator device to ensure an intentional delay exists between the two administered shocks. Alternatively, if only one ACLS qualified healthcare provider is available, then the “shock” button on both defibrillators can be pushed with one hand to ensure the creation of the intentional delay.
As per the current ACLS recommendation with single defibrillation minimize interruptions to chest compressions. CPR should continue while both defibrillators are charging to their initial energy level of 200 Joules. Once both devices become fully charged, and the scene is checked to make sure that no one is touching the patient or in contact with anything touching the patient, administer the shock as described using one of the two methods detailed above. CPR should immediately resume following administration of DED, and the patient’s pulse checked after that 2-minute cycle of compressions.
Complications
Several studies have shown that safety in a patient receiving up to 720 Joules. Furthermore, studies indicate that energy level does not require adjustment for the weight.[1][9][13][14]
As mentioned previously, there is a risk of damaging one or both defibrillator devices if any of the pads are touching one another when delivering the two shocks. To reiterate, damage to a defibrillator from the administration of DED is typically not covered by the manufacturer’s warranty.
Clinical Significance
Several case reports show the effectiveness of a second defibrillator for terminating RVF.[1][8][16][17][18] A large literature review showed DED terminating RVF in 77% of 39 cases with 11 of those patients being discharge with good neurologic outcomes indicated by a Cerebral Performance Category Score of 2 or less.[19] There is currently no evidence suggesting the use of the power theory or the setting up theory is more successful in the administration of DED or the termination of RVF. While more studies are necessary to understand DED better, the use of a second defibrillator may provide benefit and should be a consideration when treating RVF.
Enhancing Healthcare Team Outcomes
There is still much unknown regarding double external defibrillation. Future studies are required to understand better whether DSD or DSiD leads to better outcomes and whether or not increased size of the defibrillator pads, to allow more surface area for the vectors of electricity, leads to more successful defibrillation. Until then, the focus during any cardiac arrest remains early defibrillation and high-quality cardiopulmonary resuscitation. DED serves as another tool in during cardiac arrest and should be an option with other advanced life-saving therapies such as ECMO and cardiac catheterization.
Administration of double defibrillation requires an interprofessional team approach, including physicians, specialists, specialty-trained nurses, and emergency medical personnel, all collaborating across disciplines to achieve optimal patient results. [Level V]
(Click Image to Enlarge)
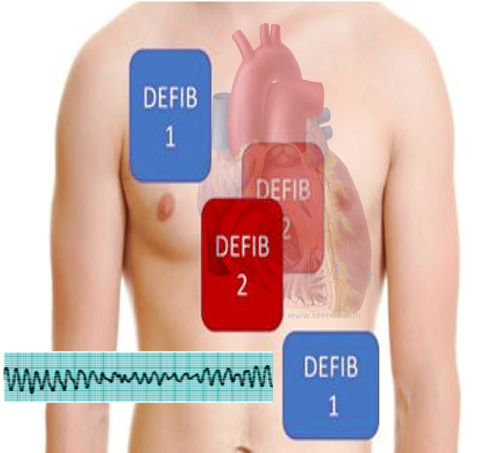
Double defibrillation
Image courtesy Dr Chaigasame