Management of Antithrombotics Around Gastrointestinal Procedures
- Article Author:
- Karthik Gnanapandithan
- Article Editor:
- Thiruvengadam Muniraj
- Updated:
- 4/17/2020 4:09:06 PM
- For CME on this topic:
- Management of Antithrombotics Around Gastrointestinal Procedures CME
- PubMed Link:
- Management of Antithrombotics Around Gastrointestinal Procedures
Introduction
Antithrombotic therapy, including antiplatelet and anticoagulants, is used to reduce the risk of thromboembolic episodes in patients with medical conditions like coronary artery disease (CAD), cerebrovascular accidents (CVA), peripheral arterial disease (PAD), atrial fibrillation (AF), venous thromboembolism (VTE), hypercoagulable states, and mechanical heart valves among others. These agents increase the bleeding risk when undertaking endoscopic procedures, but there is also a risk of thromboembolic sequelae if they are withheld. The strategy for managing this therapy when these patients need gastrointestinal (GI) endoscopic procedures has been a subject of controversy. In this chapter, we discuss this based on the available evidence and the current guidelines.[1][2][3] The two vital factors to be considered while performing an endoscopic procedure in a patient on these agents is the risk of bleeding associated with the procedure and the risk of thromboembolism associated with the underlying medical condition for which the agents are being used.
Function
Bleeding risk associated with the procedure
Various endoscopic procedures have different risks of associated bleeding. Table 1 lists the general risks of bleeding among the commonly employed endoscopic procedures.[1] Most of the data is from studies conducted in patients who are not on multiple antithrombotic agents, and hence this needs to be interpreted with caution in an individual patient. Traditionally, endoscopic procedures associated with intervention have a higher bleeding risk than those without interventions. Other factors influence this risk, as well. For example, polypectomy, one of the most common interventions during endoscopy, has a bleeding risk ranging from 0.3% to 10%, depending on poly size, location, type of polyp, and the technique for resection or cautery used. Percutaneous endoscopic gastrostomy (PEG) in patients on a single antiplatelet therapy is considered low risk, whereas a percutaneous endoscopic jejunostomy (PEJ) in general has a higher risk of bleeding. Endoscopic submucosal dissection and endoscopic resection of large (greater than 2 cm) polyps are considered ultra-high risk procedures.[3]
Thrombosis risk associated with the condition
The underlying condition dictates the risk of thromboembolic episodes in these patients, especially when withholding the antithrombotic agent. Stroke prevention in non-valvular AF is a very common indication for antiplatelet or anticoagulant therapy, and the risk of cerebral thromboembolism in these patients is predictable using the CHA(2)DS(2)Vasc index.[4] This measure includes congestive heart failure, hypertension, age greater than or equal to 75 years, diabetes mellitus, stroke or transient ischemic attack, vascular disease, age 65 to 74 years, sex category; age greater than or equal to 75 years and previous stroke carry doubled risk weight. In patients with CAD on antiplatelet therapy, a few important factors determine the risk of major adverse cardiac events. Placement of a drug-eluting coronary stent (DES) in the last 12 months or a bare-metal stent (BMS) within one month or an acute coronary syndrome (ACS) within six months are considered high-risk conditions requiring dual antiplatelet therapy (DAPT).[5] Patients on anticoagulation for venous thromboembolism (VTE) or mechanical heart valves have different risk factors for thromboembolic episodes. As shown in table 2, the patients categorize as low, medium, and high-risk groups.[5] Bioprosthetic valves are considered low risk.
Clinical Significance
INTERRUPTION OF ANTITHROMBOTIC THERAPY PRIOR TO ENDOSCOPY
ELECTIVE ENDOSCOPY
In patients who need elective endoscopic procedures, if the indication for anti-thrombotic therapy is short-term, the procedure is best delayed until after that period. For patients on long-term or life-long antithrombotic treatment, the decision on temporarily holding the treatment for endoscopy should take place after a discussion with the patient and the concerned providers (primary medical provider, cardiologist, neurologist or hematologist). In some high-risk patients, these agents cannot be interrupted, in which case the surgeon and patient must consider the risks and benefits of the procedure. A simplified summary[2] of the recommendations appears in figure 1 (anticoagulant therapy) and figure 2 (antiplatelet therapy).
Parenteral anticoagulants
Unfractionated heparin (UHF) administered as a continuous intravenous infusion can be stopped 3 to 4 hours before the procedure, given the short half-life. Low molecular weight heparin (LMWH), including enoxaparin and dalteparin, should be stopped 24 hours prior to the procedure.[2][6] Fondaparinux is a synthetic X-a inhibitor that requires discontinuation at least 36 hours preceding a high-risk procedure.
Warfarin
The therapeutic effect of warfarin is measured in terms of the International Normalized Ratio (INR). The INR decreases to less than 1.5 in over 90% of patients when holding treatment is held for five days.[7] The overall risk of a thromboembolic event when warfarin for 4 to 7 days is around 1%.[8] Hence it is recommended that it should be restarted within 4 to 7 days of initial discontinuation to keep the risk of these events to a minimum.[1] The role of bridge therapy with unfractionated heparin (UFH) or low molecular weight heparin (LMWH) has been studied for patients on warfarin for various indications. Based on the current guidelines for patients with valvular AF on warfarin, bridging is recommended for a CHA(2)DS(2)Vasc score of 2 or more. LMWH should be started two days after discontinuation of warfarin therapy, and the last dose should be administered at least 24 hours before the procedure.[2] Those with a CHA(2)DS(2)Vasc score of 0 or 1 do not require bridge therapy while withholding warfarin. Another study showed that bridge therapy for nonvalvular AF in the periprocedural period was associated with higher bleeding risk and no benefit in reducing thromboembolic episodes. However, these studies should require cautious interpretation with caution in patients with a higher risk of thrombosis.[9] In these patients, bridge therapy is always a recommendation using an interprofessional approach with the other providers managing anticoagulation therapy.
Direct Oral Anticoagulants
The use of direct oral anticoagulants (DOACs) has been on the rise over the last decade. This trend includes anti-Xa agents, rivaroxaban and apixaban, and the direct thrombin inhibitor dabigatran. There are no reliable laboratory assays to assess the anticoagulant effect of these agents at this time. The duration before high-risk endoscopic procedures that the DOACs have to be held depends on the renal function of the patient. The anti-Xa drugs should be held for 1 to 2 days if the creatinine clearance (CrCl)is 60 mL/min or more, for three days if the CrCl is between 30 mL/min and 59 mL/min and for four days if the CrCl is less than 30 mL/min.[10] The recommendation for stopping dabigatran is 2 to 3 days before a high-risk procedure in patients with CrCl more than 80 mL/min, 3 to 4 days prior if between 30 to 49 mL/min and 4 to 6 days prior if less than 30 mL/min.[11]
Antiplatelets
Aspirin and thienopyridines (clopidogrel, prasugrel, and ticagrelor) are the most commonly used antiplatelet agents. Aspirin irreversibly inhibits cyclooxygenase systems. It takes 7 to 9 days to regain platelet function following the discontinuation of aspirin.[12] Thienopyridines inhibit platelet aggregation by binding to the P2Y12 component of the platelet ADP receptors. Clopidogrel and prasugrel have to be stopped 5 to 7 days prior, to allow normal platelet aggregation to resume as opposed to ticagrelor, a reversible P2Y12 inhibitor that can be stopped 3 to 5 days prior.[13] In patients on dual antiplatelet therapy with aspirin and a thienopyridine, research has shown that those who discontinued both had a much higher incidence of stent thrombosis than those who remained on aspirin alone.[14] The recommendation for patients on antiplatelet therapy undergoing high-risk endoscopic procedures is the continue the aspirin and stop the thienopyridine agent 5 to 7 days before the procedure.[1]
EMERGENT ENDOSCOPY
The most common indication for emergent endoscopic procedures is GI bleeding. The common etiologies for acute upper GI bleeding are peptic ulcer disease, variceal bleeding and gastritis or esophagitis, while lower GI bleeding is most commonly diverticular in origin. The decision to discontinue antithrombotic therapy and reversal of anticoagulation must be weighed against the risk of incurring a thromboembolic event. For patients on warfarin, correction of INR to between 1.5 and 2.5 has demonstrated to be adequate for diagnostic purposes and to allow intervention, is comparable to patients not on any form of anticoagulation. Therapeutic measures to achieve hemostasis in patients with GI bleeding are effective even with a moderately elevated INR.[15][16] Hence it is not advisable to delay the procedure until normalization of INR. In patients with acute bleeding, warfarin can be held, and the reversal of anticoagulation is most rapidly achieved with 4-factor prothrombin complex concentrate (PCC) when compared to fresh frozen plasma (FFP).[17] Vitamin K at a dose of 5 mg or 10 mg can be given intravenously as an additional therapy. In patients with mechanical heart valves requiring reversal of anticoagulation, either FFP or PCC are options.[18] High dose vitamin K therapy is generally not preferred in these patients as it can increase the coagulability for a longer period.
If an urgent reversal of anticoagulation is necessary for patients on UFH therapy, the patient can receive a slow infusion of protamine sulfate. The dose is calculated based on the dose of heparin administered and the duration of therapy. The anticoagulant effect of dabigatran is reversible with idarucizumab, which was approved for life-threatening bleeding or before emergent surgery.[19] Since the kidneys primarily excrete it, hemodialysis is also a viable option in these patients. Andexanet alfa is a recombinant modified factor X-a protein that acts as a specific antidote for direct thrombin inhibitors, low molecular weight heparin, and fondaparinux.[20] For patients on antiplatelet therapy with acute major bleeding, the options include stopping the agent and/or reversal by platelet administration, which merits consideration with the thrombotic risk in an individual patient.
RESUMPTION OF ANTITHROMBOTIC THERAPY AFTER ENDOSCOPY
Anticoagulation should generally be resumed upon completion of the procedure unless there remains a continued risk of major bleeding.[1][6] This concept has its basis in studies available on warfarin and heparin products, with very limited literature available regarding the resumption of DOACs. For patients on warfarin with a high risk of thromboembolism, the recommendation is for UFH or LMWH to be started at the earliest possible when there is no risk of major bleeding and continued until INR reaches a therapeutic level with warfarin. For patients at a lower risk of thromboembolism, warfarin should be restarted within 24 hours of the procedure. Because of the shorter duration of DOACs, if treatment with these agents cannot resume within 24 hours of a high-risk procedure, bridge therapy should be considered with UFH or LMWH in patients with a high risk of thrombosis.[21] In patients receiving DOACs for stroke prophylaxis in AF, the use of these agents can safely resume one day after low-risk procedures and 2 to 3 days after high-risk procedures without the need for bridging.[22] All antiplatelet agents should resume soon after hemostasis.
Enhancing Healthcare Team Outcomes
It is essential for health care providers to educate patients on the importance of holding these medications for the specific duration before the procedure and on their prompt resumption. This counsel is possible through both direct counseling, educational materials, and the use of technology to send reminders. The potential risks and benefits of this strategy have to be discussed with patients by the interprofessional team. This interprofessional approach is vital in ensuring an appropriate treatment plan. In addition to the specialists, surgeons, and other clinicians, nursing will monitor the patient following the procedure. A board-certified pharmacotherapy pharmacist can consult with the clinicians in both stopping and resuming anticoagulation therapy surrounding the procedure.
A patient-centered interprofessional team consisting of the primary care provider, gastroenterologist, cardiologist, or hematologist, pharmacists, and nurses have to be involved in guiding patients on handling the change in their medication regimen, monitoring for bleeding, titration of therapy, and early recognition of any complications should they occur. This team paradigm will positively drive patient outcomes. [Level 5]
(Click Image to Enlarge)
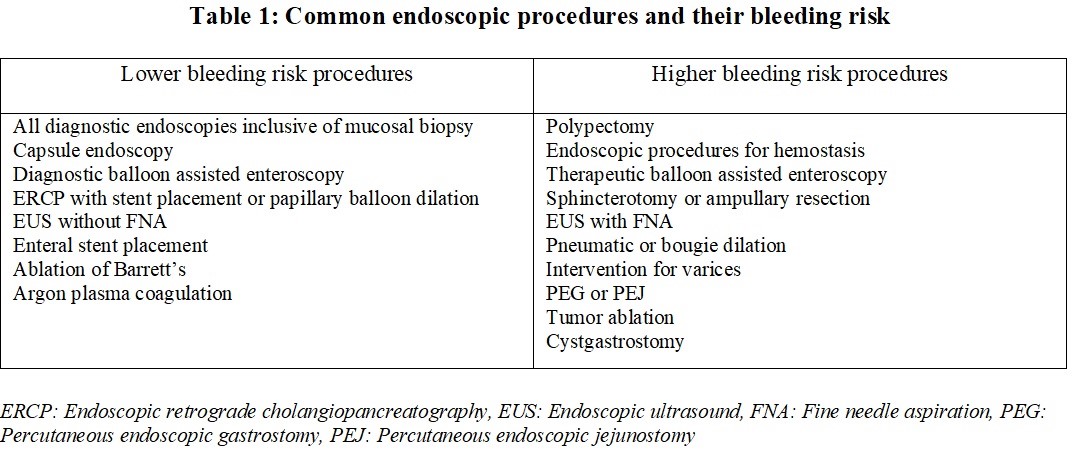
Bleeding risk associated with the various common endoscopic procedures.
Modified table from Acosta RD et al. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest Endosc 2016. CITED for the table, and also elsewhere in the text.
(Click Image to Enlarge)
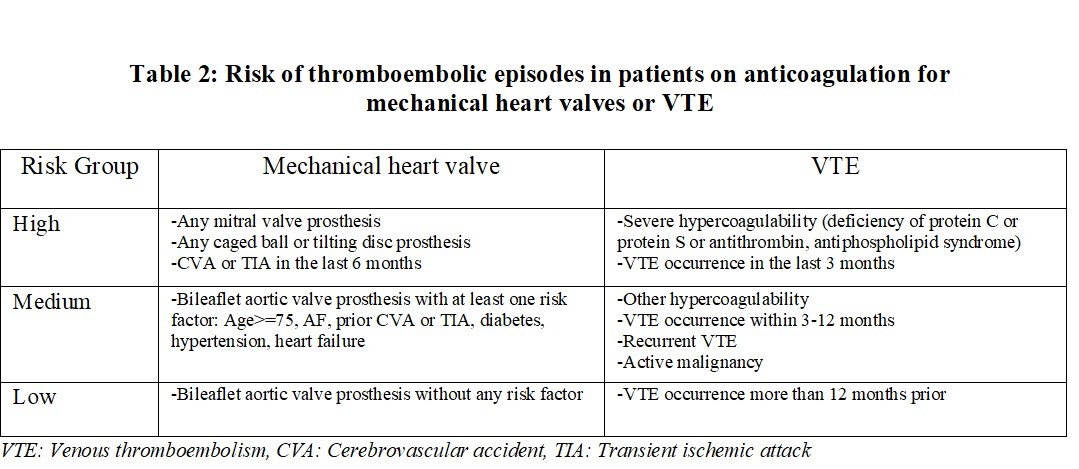
Risk of thromboembolism in patients on anticoagulation for mechanical heart valves or venous thromboembolism.
Modified table from Douketis JD. Perioperative management of antithrombotic therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; CITED and acknowledged.
(Click Image to Enlarge)
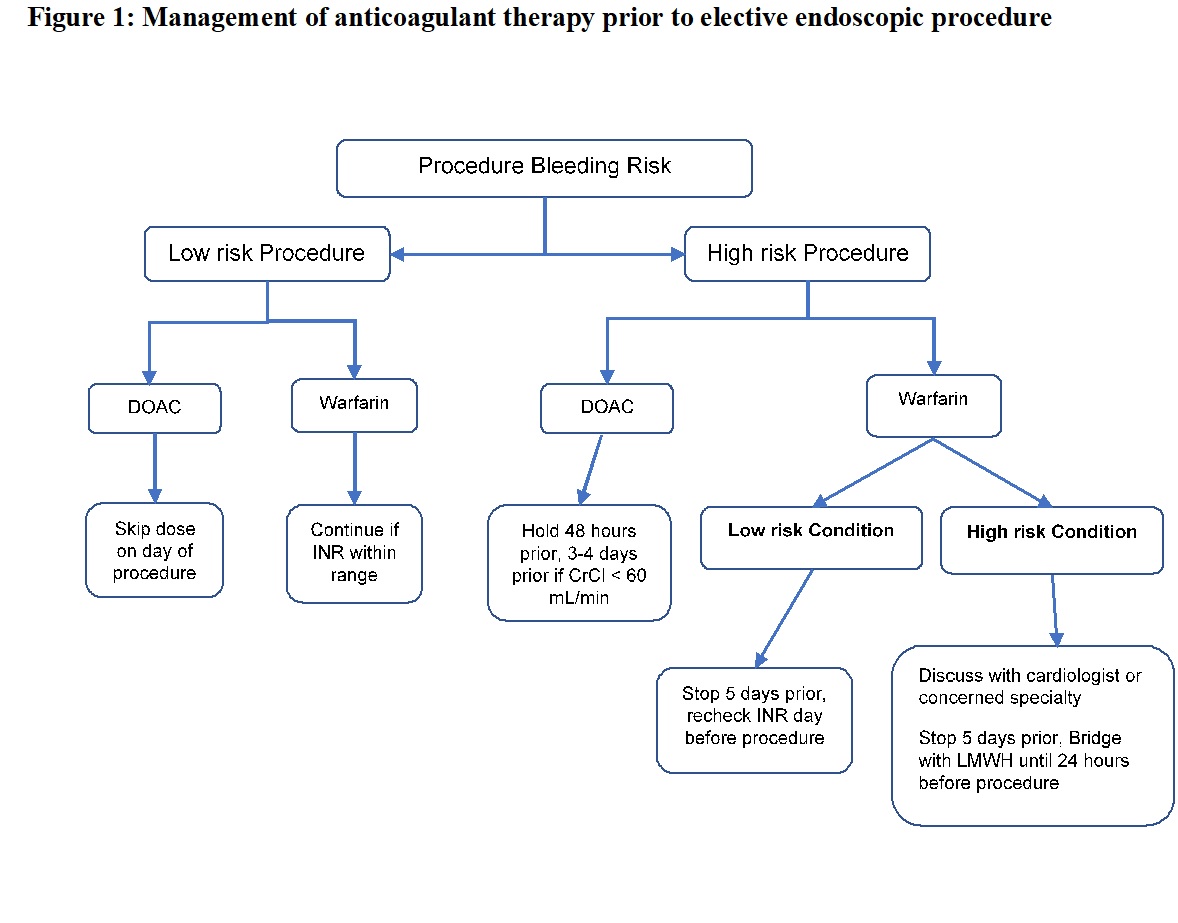
Management of anticoagulant therapy prior to elective endoscopic procedures
Modified flow chart (not copied as such). CITED and acknowledged. From: Veitch AM et al. Endoscopy in patients on antiplatelet or anticoagulant therapy , including direct oral anticoagulants : British Society of Gastroenterology ( BSG ) and European Society of Gastrointestinal Endoscopy ( ESGE ) guidelines. 2016
(Click Image to Enlarge)

Management of antiplatelet therapy prior to elective endoscopic procedures.
Modified flow chart (not copied). CITED for the figure and throughout the paper. Veitch AM et al. Endoscopy in patients on antiplatelet or anticoagulant therapy , including direct oral anticoagulants : British Society of Gastroenterology ( BSG ) and European Society of Gastrointestinal Endoscopy ( ESGE ) guidelines. 2016