Neuroanatomy, Internal Capsule
- Article Author:
- Marc Christopher Emos
- Article Editor:
- Sanjeev Agarwal
- Updated:
- 8/10/2020 5:17:13 PM
- For CME on this topic:
- Neuroanatomy, Internal Capsule CME
- PubMed Link:
- Neuroanatomy, Internal Capsule
Introduction
The internal capsule (IC) is a white matter structure composed of bundles of myelinated fibers that course past the basal ganglia. It is located in the inferomedial portion of each cerebral hemisphere and separates the caudate nucleus and thalamus from the lentiform nucleus. Ascending and descending fiber tracts course within the internal capsule to connect the cerebral hemispheres with subcortical structures, the brainstem, and the spinal cord. The internal capsule can subdivide into the anterior limb, genu, posterior limb, retrolenticular segment, and sublenticular segment. The various portions of the internal capsule mostly receive their vascular supply from perforating arteries that arise from the anterior cerebral artery, middle cerebral artery, anterior choroidal artery, and the internal carotid artery. These perforating arteries are prone to lipohyalinosis leading to ischemic damage of areas of the internal capsule resulting in clinically significant motor and sensory deficits.[1][2]
Structure and Function
The internal capsule is a two-way tract for transmission of information to and from the cerebral cortex. It is in the inferomedial portion of each cerebral hemisphere. On transverse sections of the brain, the internal capsule is a V-shaped structure with the apex pointing medially. The lentiform nucleus forms the lateral bounds of the internal capsule while the thalamus and caudate form the medial bounds. Above the superior border of the lentiform nucleus, the fibers of the internal capsule arrange in a radiating pattern known as the corona radiata. Fibers of the corona radiata travel caudally and become densely packed to form the internal capsule. The fibers become even more densely packed as they continue past the basal ganglia, forming the basis pedunculi of the midbrain. As the axons from the internal capsule travel down the brain, their numbers decrease since many descending axonal tracts terminate in the thalamus and various nuclei in the brainstem. The internal capsule subdivides into the anterior limb, genu, posterior limb, retrolenticular segment, and sublenticular segment. Each portion of the internal capsule carries distinct ascending and descending axonal tracts that each have critical functions.[1]
The internal capsule's anterior limb is bounded by the head of the caudate nucleus medially and the lentiform nucleus laterally. The anterior limb contains fibers of the anterior thalamic radiation and frontopontine fibers.[1] Anterior thalamic radiation fibers connect the anterior and medial thalamus with the prefrontal cortex and the cingulate gyrus.[3] Frontopontine fibers originate from the frontal lobe and terminate in pontine nuclei.[4] The anterior limb also contains fiber tracts that travel transversely between the caudate nucleus and the putamen. Fiber tracts in the anterior limb are known to be associated with the processing of emotion, cognition, decision making, and motivation.[5] Abnormalities in the white matter of the anterior limb are seen to be abnormal in psychiatric illnesses such as schizophrenia, bipolar disorder, and obsessive-compulsive disorder.[5] In a study utilizing diffusion MRI, researchers segmented the anterior limb into five regions.[5] These regions separate into two mediolateral areas and three dorsoventral areas. The regions were further categorized based on the cortical origins of the fibers tracts which included the ventromedial prefrontal cortex (vmPFC), ventrolateral prefrontal cortex (vlPFC), orbitofrontal cortex (OFC), dorsomedial prefrontal cortex (dmPFC), dorsolateral prefrontal cortex (dlPFC), and the dorsal anterior cingulate cortex (dACC). The ventralmost region of the anterior limb contained fibers from the vmPFC and OFC. Dorsal to this region is the main area of the anterior limb, which contains fibers from vlPFC, dACC, dlPFC, and the dmPFC.[5]
The internal capsule's posterior limb is bounded by the thalamus medially and the lentiform nucleus laterally. The posterior limb contains fibers of the posterior thalamic radiation, corticospinal tract, corticorubral tract, and corticopontine tract.[1] The anterior half of the posterior limb contains the corticospinal tract, corticorubral tract, and corticopontine tract. The corticospinal tract originates from the primary motor cortex and premotor areas. Fibers from the premotor areas are situated rostrally to fibers from the primary motor cortex. Motor fibers within the posterior limb organize somatotopically such that hand fibers are located anteromedially to foot fibers.[6] The corticospinal tract is the primary motor pathway that innervates lower motor neurons. Corticopontine fibers originate from all areas of the cerebral cortex, course to the cerebellum, and terminate in deeper pontine nuclei. These fibers are crucial for the coordination of voluntary motor functions.[7] Corticorubral fibers originate from the primary motor area and sensory areas and terminate in the red nucleus.[8] The posterior third of the posterior limb contains major somatosensory relays from the thalamus to the primary somatosensory cortex. Third order sensory fibers from the posterolateral nucleus of the thalamus tract through this region of the posterior limb and terminate in the postcentral gyrus.[9]
The location of the genu of the internal capsule is at the apex of the pallidal part of the lentiform nucleus. The anterior limb and posterior limb join at a right angle in this region to form the genu.[1]. Tracts that course through the genu include superior thalamic radiation fibers and corticobulbar tract fibers. Corticobulbar tract fibers originate from the primary motor cortex, premotor cortex, and supplementary motor areas. They course through the genu and terminate at the appropriate cranial nerve nuclei within the brainstem. The corticobulbar tract controls the muscles of the face and neck. This tract is necessary for the movement of facial musculature, mastication, and swallowing. The superior thalamic radiation fibers connect ventral nuclear group thalamic nuclei with the postcentral gyrus and appear to carry somaesthetic sensations that pass through the thalamus.[10]
The location of the sublenticular segment of the internal capsule is below the lentiform nucleus. This area contains auditory radiation fibers which course from the medial geniculate body and terminate in the transverse temporal gyri of Heschl. The retrolenticular segment of the internal capsule is around the posterior edge of the lentiform nucleus. It contains fibers of the optic radiation which connect the lateral geniculate nucleus to calcarine fissure. Parts of the optic radiation also course through the sublenticular segment of the internal capsule. The optic radiation transmits visual information from the retina to the visual cortex.[1]
Embryology
The internal capsule is a part of the telencephalon during embryologic development. The telencephalon consists of the two cerebral hemispheres of the brain. Each hemisphere is composed of the cerebral cortex, underlying white matter structures, and basal nuclei. Just like most structures of the brain, the origin of the telencephalon traces to the ectoderm, one of three germinal layers that form in the developing embryo. During embryogenesis, the notochord induces a strip of the ectoderm to form the neural plate. Further signaling from the notochord induces neurulation of the neural plate forming the neural groove and subsequently the neural tube. From the neural tube, the prosencephalon, mesencephalon, and rhombencephalon form which give rise to all regions of the brain. The prosencephalon splits and develops into the telencephalon and diencephalon.[11]
Blood Supply and Lymphatics
Each section of the internal capsule receives vascular supply by perforating branches of the main cerebral arteries. These include the anterior cerebral artery, middle cerebral artery, anterior choroidal artery, and internal carotid artery. The superior levels of the anterior limb, genu, and posterior limb get their supply from perforating arteries of the middle cerebral artery. The inferior levels of the anterior limb obtain their blood supply by the Heubner artery and perforating arteries of the anterior cerebral artery and the inferior levels of the genu get supplied by perforating arteries of the internal carotid artery and proximal perforating arteries of the anterior choroidal artery. Perforating arteries of the anterior choroidal artery supply the inferior levels of the posterior limb. The retrolenticular limb and sublenticular limb of the internal capsule are vascularized primarily by distal perforating arteries of the anterior choroidal artery.[2][12]
Clinical Significance
The internal capsule is prone to cerebrovascular accidents because the perforating arteries that supply the region are predisposed to occlusion or rupture due to their small diameter. Ischemic strokes secondary to blockage of the perforating arteries are known as lacunar strokes. The mechanisms of lacunar strokes include lipohyalinosis of perforating blood vessels, atherosclerosis of the large trunk vessels that supply perforators, and embolic occlusion of the perforating arteries. Lipohyalinosis of perforating arteries is the most common cause of lacunar strokes, and it correlates with states of chronic hypertension. It also has associations with diabetes and hyperlipidemia. The hallmark of lipohyalinosis is vessel wall thickening leading to a reduction of luminal diameter.[13][14]
Lacunar strokes primarily affect the deep structures of the brain, such as the putamen, caudate nucleus, thalamus, and internal capsule. Depending on the location of a lesion, the symptoms of lacunar strokes will require differentiation from cortical strokes. These deep strokes usually have an absence of cortical deficits such as seizures, aphasia, agnosia, and dysgraphia. Other cortical deficits include apraxia, alexia, and amnesia. The progression of symptoms of lacunar strokes are abrupt in onset and evolve within minutes. In some cases, the symptoms may develop over several hours. Many variations on lacunar stroke syndromes exist. Classic lacunar strokes syndrome that arises from lesions of the internal capsule are pure motor strokes, ataxic hemiparesis, and clumsy hand-dysarthria. Pure motor strokes have a characteristic presentation of contralateral hemiparesis that affects the face, arm, and leg in equal parts. Ataxic hemiparesis presents with a combination of ataxia and weakness on the same side of the body. These stroke syndromes can include secondary to lesions of the posterior limb of the internal capsule. Clumsy hand-dysarthria presents with difficulty with the articulation of speech and weakness in the hands and result from damage to the anterior limb of the internal capsule or genu.[15]
Due to the blood supply of the internal capsule, infarctions of different portions of the internal capsule have varied clinical presentations. The deficits secondary to infarctions of the internal capsule correlate with the fiber tracts found in each limb. The anterior limb of the internal capsule contains frontopontine fibers and anterior thalamic radiation fibers. Lesions of the anterior limb can manifest as confusion, impaired attention, agitation, and dysarthria. The genu contains corticobulbar tract fibers. Lesions of the genu can cause face and tongue weakness in addition to dysarthria. The posterior limb contains fibers of the pyramidal and extrapyramidal tracts. It also contains fibers of posterior thalamic radiations. As previously stated, lesions of the anterior half of the posterior limb can cause pure motor hemiparesis contralateral to the location of the lesion. Damage to the posterior third of the posterior limb can lead to contralateral hemisensory deficits. The retrolenticular segment of the internal capsule largely contains fibers of the optic radiations. Infarctions of this portion can lead to homonymous hemianopia, superior quadrantanopia, or inferior quadrantanopia. Finally, the sublenticular segment contains fibers of the auditory radiations. Lesions of the sublenticular limb can create auditory deficits. In general, the internal capsule is an important white matter structure that contains fiber tracts coordinating major cognitive, motor, and sensory pathways. Understanding the diverse blood supply of the internal capsule and the function of each limb are important for characterizing lesions of the internal capsule.[12]
(Click Image to Enlarge)
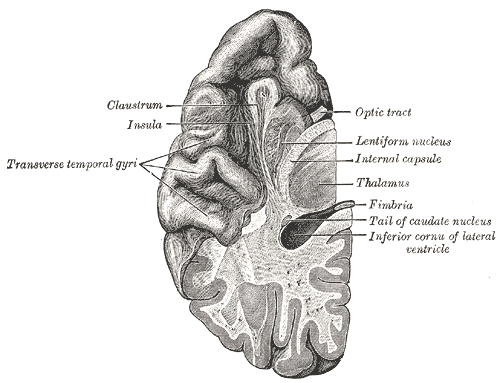
Section of brain showing upper surface of temporal lobe, Claustrum, Insula, Transverse temporal gyri, Optic tract, Lentiform nucleus, Internal capsule, Thalamus, Fimbria, Tail of Caudate Nucleus, Inferior Cornu of lateral ventricle,
Contributed by Gray's Anatomy Plates