Emergency Department Triage
- Article Author:
- Charles Yancey
- Article Editor:
- Maria O'Rourke
- Updated:
- 6/5/2020 8:53:00 PM
- For CME on this topic:
- Emergency Department Triage CME
- PubMed Link:
- Emergency Department Triage
Definition/Introduction
Triage originates from the French word "trier," which is used to describe the processes of sorting and organization. Triage is utilized in the healthcare community to categorize patients based on the severity of their injuries and, by extension, the order in which multiple patients require care and monitoring. The history of the emergency triage originated in the military for field doctors. As early as the 18th century, documentation shows how field surgeons would quickly look over soldiers and determine if there was anything they could do for the wounded soldier. French military surgeon Baron Dominique Jean Larrey, the chief surgeon in Napoleon Bonaparte's imperial guard, developed a system based on the need to evaluate and categorize wounded soldiers quickly during battle. The triage system was first implemented in hospitals in 1964 when Weinerman et al. published a systematic interpretation of civilian emergency departments using triage. Today, triage is still deeply integrated into healthcare. Triage can be broken down into three phases: prehospital triage, triage at the scene of the event, and triage upon arrival to the emergency department. There are various triage systems implemented around the world, but the universal goal of triage is to supply effective and prioritized care to patients while optimizing resource usage and timing.[1][2][3]
Emergency Department Triage in the United States (U.S.)
The most common triage system in the United States is the START (simple triage and rapid treatment) triage system. This algorithm is utilized for patients above the age of 8 years. Using this algorithm, triage status is intended to be calculated in less than 60 seconds. Various criteria are taken into consideration, including the patient's pulse, respiratory rate, capillary refill time, presence of bleeding, and the patient's ability to follow commands.[4] For children, a commonly used triage algorithm is the Jump-START (simple triage and rapid treatment) triage system. This algorithm is based on the START triage algorithm discussed earlier. However, it takes into consideration the increased likelihood for children to experience respiratory failure and their inability to follow verbal commands.[5] It is important to understand that triage is a dynamic process, meaning a patient can change triage statuses with time.[6] This will be discussed further in the field and disaster triage section of this article.
Overview of the Emergency Severity Index (ESI) Triage Algorithm
The first question in the ESI triage algorithm for triage nurses asks whether "the patient requires immediate life-saving interventions" or simply "is the patient dying?" The nurse determines this by looking to see if the patient has a patent airway, is the patient breathing, and does the patient have a pulse. The nurse evaluates the patient, checking pulse, rhythm, rate, and airway patency. Is there concern for inadequate oxygenation? Is this person hemodynamically stable? Does the patient need any immediate medication or interventions to replace volume or blood loss? Does this patient have pulselessness, apnea, severe respiratory distress, oxygen saturation below 90, acute mental status changes, or unresponsiveness? If the nurse can accurately diagnose the patient with these criteria and mark as a Level 1 trauma patient, the patient will need immediate life-saving therapy. Immediate physician involvement in the care of the patient is critical and is one of the differences between level 1 and level 2 patient designations. Another scale used by nurses in the assessment is if the patient is meeting criteria for a true level 1 trauma is the AVPU (alert, verbal, pain, unresponsive) scale. The scale is used to evaluate if the patient had a recent or sudden change in the level of consciousness and needs immediate intervention. Patients who are only responsive to painful stimuli (P) or unresponsive (U) are categorized as level 1.
If the patient is not categorized as a level 1, the nurse then decides if the patients should wait or not. This is determined by three questions; is the patient in a high-risk situation, confused, lethargic, or disoriented? Or is the patient in severe pain or distress? The high-risk patient is one who could easily deteriorate, one who could have a threat to life, limb, or organ. This is where the experience of the nurse comes into play. The clinical experience of the nurse allows for pinpointing the unusual presentations of diseases that may progress with rapid deterioration.
Once the level 1 and level 2 questions are ruled as negative, the nurse needs to ask how many different resources are needed for the physician to provide adequate care and allow the physician to reach a disposition decision. That decision meaning discharge, admit to the observation unit, or the hospital floor. The experience of the triage nurse is again referenced to make a clinical judgment on what is done for patients who typically present with these symptoms. The nurse uses experience and the routine practice of the emergency department to make this decision.
Before moving on, if the nurse has concluded that the patient will need many hospital resources during the visit, the nurse will again evaluate the patient's vital signs and look for unstable vital signs. If the patient is outside the normal or acceptable limits and approaching dangerous vitals, the patient would then be triaged as a Level 2. The dangerous vital signs are adjusted according to age. For example, if the patient was a 58-year-old man who would need multiple resources as decided by the triage nurse, and the vitals showed a heart rate of 114, oxygen saturation lower than 90%, and a respiratory rate of 26/min, that patient would be triaged as a Level 2. These findings, along with the patient's history and physical, are taken into consideration whether the triage nurse is concerned for the patient and decides on a Level 2 or 3/4/5 level triage.
Differentiating between levels 3,4, and 5 are determined by how many hospital resources the patient will most likely need. If the patient requires two or more hospital resources, the patient is triaged as a level 3. If the patient needs one hospital resource, the patient would be labeled a 4. If the patient does not need any hospital resources, the patient would be labeled a 5. One aspect of ESI that may differ at various institutions is what they consider an ESI resource. ESI triage resource examples are laboratory tests, electrocardiograms, radiographic imaging, parenteral or nebulizer medications, consultations, simple procedures such as a laceration repair, or a complex procedure. Resources qualified as "not resources" by ESI is history and physical examination (including pelvic exams), peripheral intravenous access placement, oral medications, immunizations, prescription refills, phone calls to outside physicians, simple wound care, crutches, splints, or slings. Whether or not some emergency departments (EDs) send certain tests such as a urinalysis or pregnancy test to the laboratory would change the ESI level between a 4 and a 5. Regardless, ESI is a simple and effective way for nurses to assess patient needs.
Field and Disaster Triage
Emergency medicine services (EMS) are the front-line personnel that are the first eyes and ears on patients. Their clinical decision making is just as important as physicians when it comes to the outcome of a patient. In mass casualty events or disasters, the emergency providers must be able to quickly size up the scene, develop an action plan, and do the most good for the most amount of people. These can include difficult decisions being made by physicians, EMS, and nurses regarding who to provide care for immediately, who can wait, and who cannot be saved. There have been many different algorithms in how to properly triage patients in the field to help responders develop a system on care. One of these algorithms is called START triage, which stands for "simple triage and rapid transport." As emergency responders arrive at the scene, victims are asked to walk to a designated area marked off for care. Anyone who can follow these commands and walk to this area is designated as "minor" and given a green tag to signify minor injury status. Once the "minor" injuries are out of the area, responders should begin to move and triage patients with the RPM acronym; respirations, perfusion, and mental status. This includes making sure the individual has a manual respiration rate that is roughly greater than 30 breaths a minute, peripheral pulses are present with a capillary refill of fewer than 2 seconds and can follow commands. If a patient has none of these, the patient is declared deceased, given a black tag, and moved to the black coded area. If individuals can breathe spontaneously, follow simple commands, and have distal pulses with a normal capillary refill, they are tagged delayed and given the code yellow. The rest of the individuals who have poor respirations or cannot protect their airway, have absent or decreased peripheral pulses, and unable to follow simple commands are tagged immediately and given the color red. With this method, providers can quickly rule in and rule out individuals who require immediate medical attention, who can wait, and who nothing can be done for. However, the assignment of individuals in this algorithm is purely based on vital signs that can change rapidly in the field.
Another algorithm of triage is called the SALT triage or sort, assess, life-saving interventions, and treatment/transport. This is similar to the START triage system as it asks individuals who can walk to a specific area of treatment marked off for minor injuries. After, individuals not able to ambulate are asked to wave their hands to identify themselves. This allows providers to assess who can follow commands and walk, who can follow commands but cannot ambulate, and who is not able to follow commands and wave their hands. The individuals who are not waving their hands are taken care of first as they most likely need immediate medical attention, then the individuals waving their hands, then those who were able to ambulate over to the designated treatment area. Affected individuals can be divided into one of five categories based on this initial assessment; immediate, expectant, delayed, minimal, or deceased. Categorization is based similarly to the START triage system of mental status, presence or absence of peripheral pulses, and the presence or absence of respiratory distress. One difference between the SALT and START triage is that Salt asks an internal question to differentiate between immediate or expectant. The question is, "Is the patient likely to survive the current circumstance given the resources available?" If the answer is no, then the patient is deemed expectant. The benefit of the SALT method vs. the START method is that there is a grey area that is provided for the population affected and allows providers to be more flexible with their decision making. However, this could be hard on the mental health of providers who are making decisions on whether someone receives treatment or not.
The Australasian Triage Scale
Originally named the international triage scale (ITS), the Australasian triage scale or ATS is based on a 5-level categorical scale. Originally used in The Box Hill Hospital in Victoria, after successful trials in several Australian Hospitals, the ITS was adopted as the national triage scale (NTS) in 1993 by the Australasian College of Emergency Medicine. The NTS would then become the ATS in 2000. ATS is now the basis of performance reporting in EDs across Australia. Several international scales have been based on the ATS, such as the Canadian scale (CTAS) in 1999, further upgraded in 2004 and 2008. Other countries and institutions have adopted models like the ATS and CTAS, such as Sweden, Andorra, Netherlands, and while ESI is used in Greece.[7]
ATS incorporates looking at presenting patients' problems, appearance, and overview of pertinent physiological findings. These pertinent physiological findings are based on 79 clinical descriptors. The nurse is then able to determine how urgent the patient needs to be seen and categorizes them based on how much time the patient can wait to see a physician. Figure 1.1 will show a categorization of the different levels of urgency and the corresponding response time, patient description of what goes into that category, and clinical indicators that justify the patient being triaged into that category.[8]
In specific populations or presentations, special considerations are taken. In pediatric cases, generally, the same standard triage categorization is applied. However, individual department policies may differ, due to some departments offering fast track options for certain populations such as pediatrics or trauma patients. Both of these populations are triaged mostly due to objective clinical urgency. In the case of behavioral patients, both physical and behavioral assessments are used to determine severity. When both physical and behavioral problems are present, the patient is placed in the highest appropriate category.
The Canadian Triage System
Also known as the Canadian triage and acuity scale or CTAS, is based on the NTS of Australia. CTAS is a 5-level triage system based on the severity of the illness or time needed before medical intervention combined with a standardized presenting patient complaint list. Similar to other 5 level triage systems, starting with level one as the most severe patients needing immediate medical attention, and descending in severity to level five (non-urgent). Each level of acuity in CTAS has a certain set of symptoms, including cardiovascular, mental health, environmental, neurological, respiratory, obstetrics/gynecology, gastrointestinal, and trauma. Under each category, are a list of symptoms specific to that organ system that, if present, the patient is classified under that level.[8]
Unique to CTAS is the first and second-order modifiers that are used after an initial acuity level is given to a patient that changes that patient's acuity level. These were first implemented in 2004 when the system underwent a revision. The revision allowed triage nurses to use these modifiers to change the acuity level of the patient. First-order modifiers include vital signs, pain scales, mechanism of injury, level of consciousness, each looking for worsening of a certain pathology, such as hemodynamic instability, sepsis, and cognitive impairment.[8] Second-order modifiers are complaint specific and are applied after a general complaint, and first-order modifiers have been determined. The second-order modifiers include blood glucose level, dehydration, hypertension, pregnancy longer than 20 weeks, and mental health complaints. If patients meet criteria to be categorized with one of the following second-order modifiers, their CTAS level is changed based on patient presentation.[9]
Chinese Four-level and Three District Triage Standard
The Chinese four-level and three district triage standard or CHT was drafted in 2011 by the Chinese Ministry of Health. However, only 43% of the hospitals use the formal 4 tier scale, while 34% of the hospitals adopted the ATS. In the CHT system, each patient is categorized into one of four categories based on the level of acuity. Similar to ATS, the categories are based on the level of acuity. Category one is a critically ill patient who needs life-saving intervention. Category two is reserved for patients whose current condition is likely to destabilize to a category one if treatment is not administered in a short amount of time. Category three is considered emergent, where there are no life-threatening disabilities, and treatment can be given within a certain set time. Category four is considered non-emergent. Based on the level of acuity, the triage nurses sort the patients into three distinct treatment areas. These areas are the red zone, which is considered a resuscitation zone for category one patients, and a rescue room for category two patients. The next two areas are the yellow and green zone, which treat category three and four patients.
Manchester Triage System
The Manchester triage system (MTS) is one of the most common triage systems used in Europe. What is unique about this particular system is that it utilizes 52 flowcharts based on patients presenting complaints. Each flowchart has additional signs and symptoms named "discriminators," which would be categorized as worsening symptoms or signs of a particular disease, such as airway compromise or persistent vomiting. These discriminators are then ranked by priority from most severe to least severe. Each group of discriminators tells the nurse how urgent the patient's visit is. If the patient meets a certain group of discriminators, he or she is categorized into an urgency category that ranges from immediate to non-urgent. The urgency categorization is tied to a maximum waiting time, with immediate maximum waiting time being 0 minutes, very urgent is 10 minutes max. Urgent waiting time is maxed at 60 minutes, standard 120 minutes, and non-urgent waiting time is maxed at 240 minutes. Each triage nurse who performs these examinations receives training on how to navigate the charts and accurately triage the patient into the most accurate category.[10][11]
Issues of Concern
When triaged accurately, patients receive care in an appropriate and timely manner by emergency care providers. This limits their injuries and their complications. However, incorrectly triaged patients could sustain further injury and complications.[12][13] Additionally, the main limitations of today's triage systems lie in their lack of sensitivity and specificity. Given the multitude of variables present during prehospital triage, it is difficult to establish a triage system that applies to all situations appropriately.[1]
The effectiveness and validity of the MTS have shown mixed results when being reviewed in journals. A study by Zachariasses et al. in 2017 examined the validity of the MTS by performing a prospective observational study in three European emergency departments during a one-year period. They examined the validity by looking at the proportion of correctly triaged patients to over and under triaged patients. Their results showed that in more vulnerable populations, the pediatric and the elderly population, these groups showed poorer performance. This conclusion is further supported in a 2019 cohort study by Brouns et al. that showed that the MTS has worse performance in patients over the age of 65 as compared to patients between 18-64 years. This was accurate also for predicting the in-hospital mortality of patients over 65 years as compared to 18 to 64-year-old patients. However, when predicting hospitalization and in-hospital mortality for surgical patients over 65 years, it showed better predictive ability compared to medical patients over 65 years of age. This study also showed accuracy in the prediction of in-hospital mortality with increasing MTS urgency between the age groups of 18 to 64 years. The inconsistencies between the age groups are possibly due to the increasing complexity of medical issues in patients over 65 years.[10][11]
Modern emergency departments are crowded places with many different people with different complaints, all with different levels of severity. Nurses must be able to scan crowded emergency departments for critically ill patients and move them to the front. If this occurs, nurses must be able to anticipate the prioritization and status of available treatment areas. An optimal arrival to proper triage of the patient should occur in 10-15 minutes. As patients wait in busy emergency rooms, they should advise the nursing staff if there have been any changes in their condition. To facilitate this, a major international study would be useful to compare the expression of the CTAS, MTS, and ATS in terms of the patterns of population descriptions, the outcomes, and the consistency of the results of different triage systems.
Clinical Significance
In the U.S., the primary system in use is ESI. The ESI, similar to the Canadian, Australian, and United Kingdom systems, is a five-level triage system focusing on the prioritization of patients who need help immediately and the urgency of the treatment of the patient’s conditions. The ESI system went through several revisions based on studies done at university-based emergency departments. These revisions were based on limitations shown in the study done by Tanabe et al., showing that many patients classified as level 2 patients would have benefited from being classified as level 1 to receive lifesaving interventions.[14]
Unlike the Australian, Canadian, and U.K. systems, the ESI focuses more on the urgency and how severe the patient’s symptoms are, rather than evaluating how long the patient can wait before being seen. Another difference in the ESI system, is the requirement of nurses to also anticipate the needs of subacute patients, those who are deemed stable. This is so stable patients who are finally seen by physicians can properly and efficiently be placed in the appropriate care for their condition. Nurses and administrators also have seen benefits in the ESI system. A study by Wuerz et al. in 2001 showed improved communication of inpatient acuity compared to the three-tiered system. Communications between charge nurses and triage nurses were simplified for patient needs. Hospital administrators are also able to simply look at available resources in the hospital that would be needed for different levels of acuity based on ESI, and then make decisions on needing additional resources or needing to divert incoming patients to other hospitals. Overall, the ESI systems have improved quality in the assessment of patient care and improved the quality of communication and hospital resource applications by providers and hospital administrators.[14]
In a 2019 study by Zhu et al., the validity was compared between the ATS and the CHT. The study found that both the ATS and CHT had similar validity in the categorization of higher acuity patients. Also, the ATS and CHT both had good reliability based on the Fleiss grade. The study concluded that both systems were adequate in identifying critically ill patients in the emergency department.[15]
Nursing, Allied Health, and Interprofessional Team Interventions
It has been shown that triage refresher training programs in emergency departments do not yield an increase in triage accuracy.[16][Level 1] However, when given a single presentation explaining the logic and characteristics of triage systems, healthcare workers were significantly more likely to triage patients correctly.[17][18] [Level 1] Of note, the transition between EMS care and hand-off to the emergency department is crucial whether the transfer involves different healthcare providers, such as technicians, nurses, and physicians. Studies have shown that it is best to train using the same common triage criteria.[19]
Nursing, Allied Health, and Interprofessional Team Monitoring
As in training and practice, monitoring performance measures across interprofessional teams help identify collaborative care outcomes.[20]
(Click Image to Enlarge)
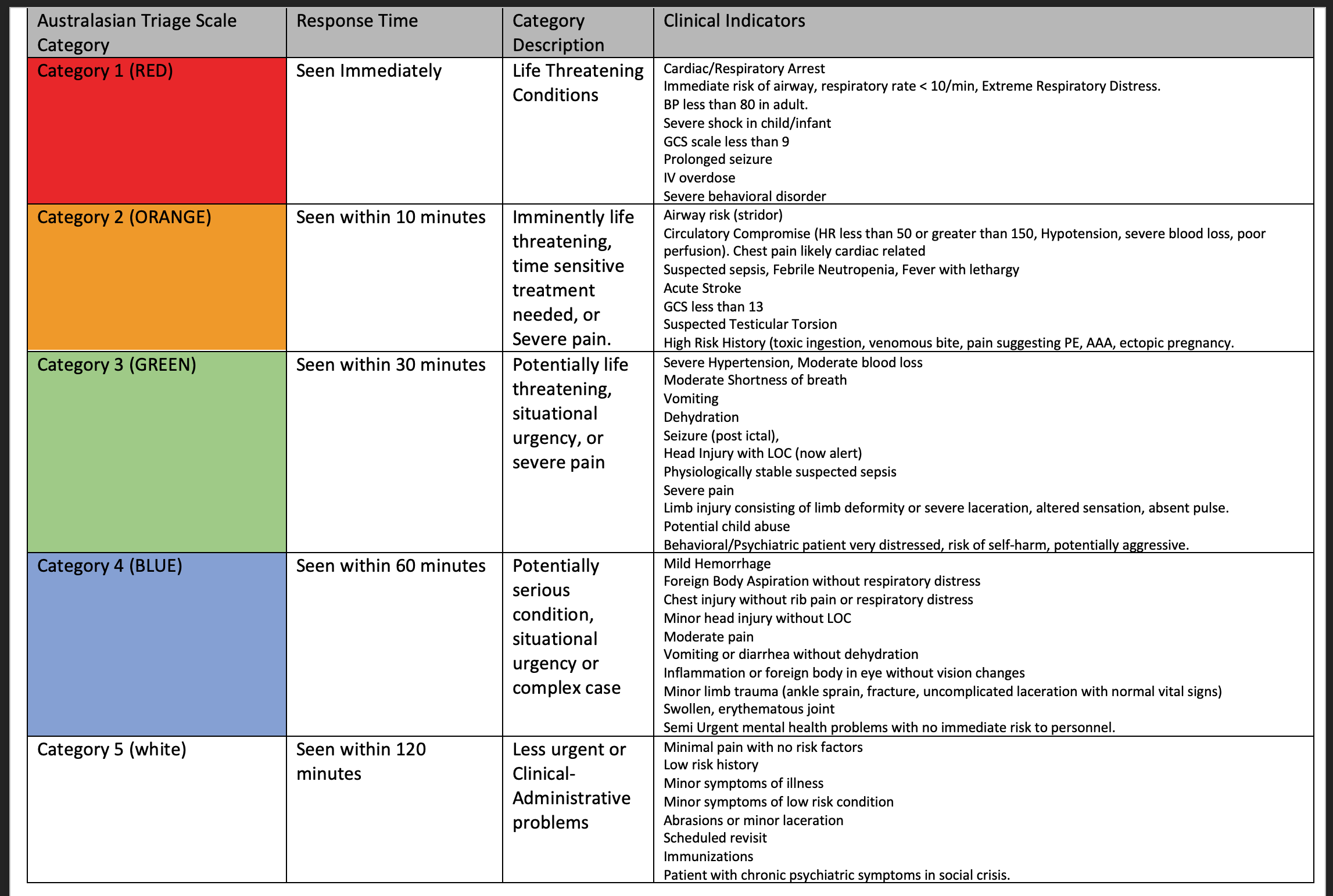
Australasian Triage Scale Figure.
Contributed by Charles Yancey