Castleman disease
| Castleman diseases | |
|---|---|
| Other names | Giant lymph node hyperplasia, lymphoid hamartoma, angiofollicular lymph node hyperplasia |
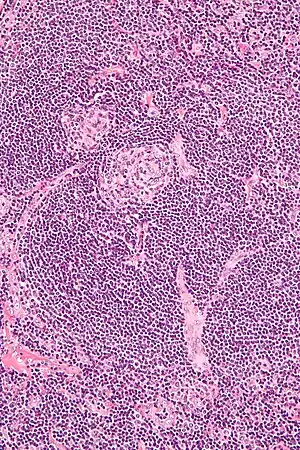 | |
| Micrograph of Castleman disease showing hyaline vascular features including atrophic germinal center, expanded mantle zone, and a radially penetrating sclerotic blood vessel ("lollipop" sign). H&E stain. | |
| Specialty | Immunology, angiology |
Castleman disease is a group of uncommon lymphoproliferative disorders characterized by lymph node enlargement, which often manifests without any other obivous symptoms.
Castleman disease includes at least three distinct subtypes: unicentric Castleman disease (UCD), human herpesvirus 8 associated multicentric Castleman disease (HHV-8-associated MCD), and idiopathic multicentric Castleman disease (iMCD). These are differentiated by the number and location of affected lymph nodes and the presence of human herpesvirus 8, a known causative agent. Correctly classifying the Castleman disease subtype is important, as the three subtypes vary significantly in symptoms, clinical findings, disease mechanism, treatment approach, and prognosis. In the United States, approximately 6,500 to 7,700 new cases are diagnosed each year.[1]
Castleman disease is named after Benjamin Castleman, who first described the disease in 1956. The Castleman Disease Collaborative Network is the largest organization focused on the disease and is involved in research, awareness, and patient support.[2]
Classification
The subtypes of Castleman disease reflect the number of lymph node regions with enlarged lymph nodes and known causes of the disease.[3] In unicentric disease, one or more enlarged lymph nodes are present in a single region of lymph nodes. In multicentric disease, enlarged lymph nodes are present in multiple regions of lymph nodes. The only known cause of Castleman disease is uncontrolled infection with human herpesvirus 8, which has only been reported in cases of multicentric disease.[3] There are three established subtypes of Castleman disease.[4]
Unicentric Castleman disease
In unicentric Castleman disease (UCD) one or more enlarged lymph nodes are present in a single region of lymph nodes. The cause of UCD is unknown.[5] It is the most common subtype of Castleman disease and compared to HHV-8-associated MCD and iMCD, symptoms are typically milder and relate to the lymph node affected, and organ dysfunction is uncommon. Surgical removal of enlarged lymph nodes is the treatment of choice, but in cases that resection is not an option, treatment is similar to iMCD cases.[6][7]
Idiopathic multicentric Castleman disease
In idiopathic multicentric Castleman disease (iMCD), enlarged lymph nodes are present in multiple lymph node regions and no known cause for the disease is identified. It is less common than unicentric Castleman disease (UCD) and compared to UCD, symptoms are typically more severe, laboratory abnormalities must be present for diagnosis, and medications are used for treatment as surgery is ineffective.[6] Symptoms include systemic inflammatory and organ dysfunction. Medications used for treatment include antivirals, cytotoxic chemotherapy and rituximab.[1] Two great challenges in the diagnosis and treatment of iMCD are the spectrum of nonspecific symptoms and the unclear etiology of the disease.[8]
Human herpesvirus 8 associated multicentric Castleman disease
In human herpesvirus 8 associated multicentric Castelman disease (HHV-8-associated MCD), enlarged lymph nodes are present in multiple lymph node regions and infection with human herpesvirus 8 is present. It is less common than unicentric Castleman disease and diagnosed most frequently in patients infected with human immunodeficiency virus (HIV). Compared to UCD and iMCD, HHV-8-associated MCD presents with similar symptoms and clinical findings to iMCD. While UCD is readily treatable with surgery, HHV-8-associated MCD, like iMCD, is treated with medications as surgery is ineffective.[6]
TAFRO Syndrome: a constellation of clinical symptoms reported in some iMCD and HHV-8 associated MCD patients. The clinical symptoms are Thrombocytopenia, Anasarca, Fever, Reticulin fibrosis, and Organomegaly. These patients respond well to immunosuppressive therapy and steroids.[9]
Pathology
Castleman disease is defined by a range of characteristic features seen on microscopic analysis (histology) of tissue from enlarged lymph nodes.[10] Histologic features consistent with Castleman disease are categorized into common patterns:
- Hyaline vascular: regressed germinal centers, follicular dendritic cell prominence or dysplasia, hypervascularity in interfollicular regions, sclerotic vessels, prominent mantle zones with an “onion-skin” appearance.[11]
- Plasmacytic: increased number of follicles with large hyperplastic germinal centers and sheetlike plasmacytosis (increased number plasma cells).[10][11]
- Hypervascular: similar to hyaline vascular features, but seen in iMCD rather than UCD. Includes regressed germinal centers, follicular dendritic cell prominence, hypervascularity in interfollicular regions, and prominent mantle zones with an “onion-skin” appearance.[11]
- Mixed: presence of a combination of hyaline vascular, plasmacytic, and/or hypervascular features
UCD most commonly demonstrates hyaline vascular features, but plasmacytic features or a mix of features may also be seen.[7] iMCD more commonly demonstrates plasmacytic features, but hypervascular features or a mix of features are also seen. All cases of HHV-8-associated MCD are thought to demonstrate plasmablastic features—similar to plasmacytic features, but with plasmablasts present.[10] The clinical utility of subtyping Castleman disease by histologic features is uncertain, as histologic subtypes do not consistently predict disease severity or treatment response.[10]
Staining with latency-associated nuclear antigen (LANA-1), a marker for HHV-8 infection, is positive only in HHV-8-associated MCD.[12]
Diseases other than Castleman disease can present with similar histologic findings in lymph node tissue, including:[10]
History
Unicentric Castleman disease was first described in a case series by Benjamin Castleman in 1956.[13] By 1984, a number of case reports had been published describing a multicentric variant of the disease and with some reports describing an association with Kaposi's sarcoma.[14] In 1995, the association between HHV-8 and Castleman disease was described in patients with HIV.[15] Formal diagnostic criteria and definition of the disease was established in 2016, which will allow for better understanding and the ability to appropriately track and research CD. In 2017, international consensus diagnostic criteria for idiopathic multicentric Castleman disease (iMCD) were established for the first time.[10] In 2018, the first treatment guidelines for iMCD were established.[16]
World Castleman Disease Day was established in 2018 and is held every year on July 23. This date was chosen for Benjamin Castleman's initial case series describing Castleman disease, which was published in July 1956,[13] and the diagnostic criteria for idiopathic multicentric Castleman disease, which were published in the journal Blood on March 23, 2017.[10]
Culture
The Castleman Disease Collaborative Network was founded in 2012 and is the largest organization to be focused on Castleman disease.[17] It is a global collaborative network involved in research, awareness, and patient support.[18]
References
- 1 2 Yu, Li; Tu, Meifeng; Cortes, Jorge; Xu-Monette, Zijun Y.; Miranda, Roberto N.; Zhang, Jun; Orlowski, Robert Z.; Neelapu, Sattva; Boddu, Prajwal C.; Akosile, Mary A.; Uldrick, Thomas S. (2017-03-23). "Clinical and pathological characteristics of HIV- and HHV-8–negative Castleman disease". Blood. 129 (12): 1658–1668. doi:10.1182/blood-2016-11-748855. ISSN 0006-4971. PMC 5364343. PMID 28100459.
- ↑ "Castleman Disease Collaborative Network". CDCN. Retrieved 2019-12-30.
- 1 2 Fajgenbaum DC, Shilling D (February 2018). "Castleman Disease Pathogenesis". Hematology/Oncology Clinics of North America. 32 (1): 11–21. doi:10.1016/j.hoc.2017.09.002. PMID 29157613.
- ↑ "What Is Castleman Disease?". www.cancer.org. Retrieved 2020-10-25.
- ↑ Yu, Li; Tu, Meifeng; Cortes, Jorge; Xu-Monette, Zijun Y.; Miranda, Roberto N.; Zhang, Jun; Orlowski, Robert Z.; Neelapu, Sattva; Boddu, Prajwal C.; Akosile, Mary A.; Uldrick, Thomas S. (2017-03-23). "Clinical and pathological characteristics of HIV- and HHV-8–negative Castleman disease". Blood. 129 (12): 1658–1668. doi:10.1182/blood-2016-11-748855. ISSN 0006-4971. PMC 5364343. PMID 28100459.
- 1 2 3 Oksenhendler E, Boutboul D, Fajgenbaum D, Mirouse A, Fieschi C, Malphettes M, Vercellino L, Meignin V, Gérard L, Galicier L (January 2018). "The full spectrum of Castleman disease: 273 patients studied over 20 years". British Journal of Haematology. 180 (2): 206–216. doi:10.1111/bjh.15019. PMID 29143319.
- 1 2 Talat N, Belgaumkar AP, Schulte KM (April 2012). "Surgery in Castleman's disease: a systematic review of 404 published cases". Annals of Surgery. 255 (4): 677–84. doi:10.1097/SLA.0b013e318249dcdc. PMID 22367441. S2CID 7553851.
- ↑ Iwaki, Noriko; Fajgenbaum, David C.; Nabel, Christopher S.; Gion, Yuka; Kondo, Eisei; Kawano, Mitsuhiro; Masunari, Taro; Yoshida, Isao; Moro, Hiroshi; Nikkuni, Koji; Takai, Kazue (2016). "Clinicopathologic analysis of TAFRO syndrome demonstrates a distinct subtype of HHV-8-negative multicentric Castleman disease". American Journal of Hematology. 91 (2): 220–226. doi:10.1002/ajh.24242. ISSN 1096-8652. PMID 26805758. S2CID 521845.
- ↑ Iwaki, Noriko; Fajgenbaum, David C.; Nabel, Christopher S.; Gion, Yuka; Kondo, Eisei; Kawano, Mitsuhiro; Masunari, Taro; Yoshida, Isao; Moro, Hiroshi; Nikkuni, Koji; Takai, Kazue (2016). "Clinicopathologic analysis of TAFRO syndrome demonstrates a distinct subtype of HHV-8-negative multicentric Castleman disease". American Journal of Hematology. 91 (2): 220–226. doi:10.1002/ajh.24242. ISSN 1096-8652. PMID 26805758. S2CID 521845.
- 1 2 3 4 5 6 7 Fajgenbaum DC, Uldrick TS, Bagg A, Frank D, Wu D, Srkalovic G, et al. (March 2017). "International, evidence-based consensus diagnostic criteria for HHV-8-negative/idiopathic multicentric Castleman disease". Blood. 129 (12): 1646–1657. doi:10.1182/blood-2016-10-746933. PMC 5364342. PMID 28087540.
- 1 2 3 Keller AR, Hochholzer L, Castleman B (March 1972). "Hyaline-vascular and plasma-cell types of giant lymph node hyperplasia of the mediastinum and other locations". Cancer. 29 (3): 670–83. doi:10.1002/1097-0142(197203)29:3<670::aid-cncr2820290321>3.0.co;2-#. PMID 4551306.
- ↑ Liu AY, Nabel CS, Finkelman BS, Ruth JR, Kurzrock R, van Rhee F, Krymskaya VP, Kelleher D, Rubenstein AH, Fajgenbaum DC (April 2016). "Idiopathic multicentric Castleman's disease: a systematic literature review". The Lancet. Haematology. 3 (4): e163–75. doi:10.1016/S2352-3026(16)00006-5. PMID 27063975.
- 1 2 Castleman, B.; Iverson, L.; Menendez, V. P. (July 1956). "Localized mediastinal lymphnode hyperplasia resembling thymoma". Cancer. 9 (4): 822–830. doi:10.1002/1097-0142(195607/08)9:4<822::aid-cncr2820090430>3.0.co;2-4. ISSN 0008-543X. PMID 13356266.
- ↑ Chen KT (April 1984). "Multicentric Castleman's disease and Kaposi's sarcoma". The American Journal of Surgical Pathology. 8 (4): 287–93. doi:10.1097/00000478-198404000-00006. PMID 6711739. S2CID 38948699.
- ↑ Soulier J, Grollet L, Oksenhendler E, Cacoub P, Cazals-Hatem D, Babinet P, et al. (August 1995). "Kaposi's sarcoma-associated herpesvirus-like DNA sequences in multicentric Castleman's disease". Blood. 86 (4): 1276–80. doi:10.1182/blood.V86.4.1276.bloodjournal8641276. PMID 7632932.
- ↑ van Rhee, Frits; Voorhees, Peter; Dispenzieri, Angela; Fosså, Alexander; Srkalovic, Gordan; Ide, Makoto; Munshi, Nikhil; Schey, Stephen; Streetly, Matthew (2018-09-04). "International, evidence-based consensus treatment guidelines for idiopathic multicentric Castleman disease". Blood. 132 (20): blood-2018-07-862334. doi:10.1182/blood-2018-07-862334. ISSN 1528-0020. PMC 6238190. PMID 30181172.
- ↑ "Castleman Disease Collaborative Network". CDCN. Retrieved 2019-12-30.
- ↑ Fajgenbaum, David C.; Ruth, Jason R.; Kelleher, Dermot; Rubenstein, Arthur H. (April 2016). "The collaborative network approach: a new framework to accelerate Castleman's disease and other rare disease research". The Lancet Haematology. 3 (4): e150–152. doi:10.1016/S2352-3026(16)00007-7. ISSN 2352-3026. PMID 27063967.
Further reading
- Fajgenbaum, David (2019). Chasing My Cure: A Doctor's Race to Turn Hope into Action; a Memoir. New York: Ballantine Books. ISBN 9781524799618. OCLC 1144129598. Book by the founder of the Castleman Disease Collaborative Network.