Acceleromyograph
An acceleromyograph is a piezoelectric myograph, used to measure the force produced by a muscle after it has undergone nerve stimulation. Acceleromyographs may be used, during anaesthesia when muscle relaxants are administered, to measure the depth of neuromuscular blockade and to assess adequacy of recovery from these agents at the end of surgery. Acceleromyography is classified as quantitative neuromuscular monitoring.
Rationale
Patients who undergo anesthesia may receive a drug that paralyzes muscles, facilitating endotracheal intubation and improving operating conditions for the surgeon. Longer-acting drugs have higher prevalence of residual blockade in the PACU or ICU than shorter acting drugs. Different clinical tests to measure or exclude evidence of residual muscle weakness have been described but cannot exclude postoperative residual curarization.[1] Small degrees of muscle blockade can only accurately be measured by the use of quantitative neuromuscular monitoring. Specifically, the observer cannot reliably measure muscular fade when train-of-four ratios are between 0.4 and 0.9.[2]
Acceleromyograph design
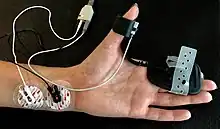
Acceleromyographs measure muscle activity using a miniature piezoelectric transducer that is attached to the stimulated muscle. A voltage is created when the muscle accelerates and that acceleration is proportion to force of contraction. The mass of the piezoelectric transducer is known and the acceleration is measured therefore the force can be calculated, (Force = mass × acceleration). Acceleromyographs are more costly than the more common twitch monitors, but have been shown to better alleviate residual blockade and associated symptoms of muscle weakness, and to improve overall quality of recovery.
See also
References
- ↑ Brull SJ, Murphy GS (July 2010). "Residual neuromuscular block: lessons unlearned. Part II: methods to reduce the risk of residual weakness". Anesth. Analg. 111 (1): 129–40. doi:10.1213/ANE.0b013e3181da8312. PMID 20442261.
- ↑ Capron F, Fortier LP, Racine S, Donati F (May 2006). "Tactile fade detection with hand or wrist stimulation using train-of-four, double-burst stimulation, 50-hertz tetanus, 100-hertz tetanus, and acceleromyography". Anesth. Analg. 102 (5): 1578–84. doi:10.1213/01.ane.0000204288.24395.38. PMID 16632846.
External links
- Comparison of mechanomyography and acceleromyography at Respond2Articles.com