Cancer survivor
A cancer survivor is a person with cancer of any type who is still living. Whether a person becomes a survivor at the time of diagnosis or after completing treatment, whether people who are actively dying are considered survivors, and whether healthy friends and family members of the cancer patient are also considered survivors, varies from group to group. Some people who have been diagnosed with cancer reject the term survivor or disagree with some definitions of it.
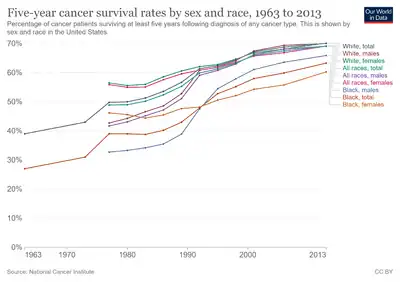
How many people are cancer survivors depends on the definition used. Currently nearly 65% of adults diagnosed with cancer in the developed world are expected to live at least five years after the cancer is discovered.[1] In the U.S. for example, about 11 million Americans alive today—one in 30 people–are either currently undergoing treatment for cancer or have done so in the past.[2]
Many cancer survivors describe the process of living with and beating cancer as a life-changing experience.[3] It is not uncommon for survivors to use the experience as opportunities for creative self-transformation into a "better person" or as motivation to meet goals of great personal importance, such as climbing a mountain or reconciling with an estranged family member. This process of posttraumatic growth is called benefit finding.[4] Cancer survivors often have specific medical and non-medical needs related to their cancer experience.
Definitions and alternatives
Macmillan Cancer Support in the UK defines a cancer survivor as someone who is "living with or beyond cancer", namely someone who:
- has completed initial cancer management and has no apparent evidence of active disease;
- is living with progressive disease and may be receiving cancer treatment, but is not in the terminal phases of illness; or
- has had cancer in the past.[5]
The National Coalition for Cancer Survivorship (NCCS) pioneered the definition of survivor as being any person diagnosed with cancer, from the time of initial diagnosis until his or her death. This expansive definition of "survivor" includes people who are dying from untreatable cancer. NCCS later expanded the definition of survivor even further to include family, friends and voluntary caregivers who are affected by the diagnosis in any way.[6] The US National Cancer Institute's Office of Cancer Survivorship uses a variant of this expanded definition.[6]
The word survivor is a loaded term.[3] Within the breast cancer culture, survivorship is conferred upon women and men who are perceived as having suffered emotional or physical trauma, even if their breast cancer was a non-life-threatening pre-cancerous condition like LCIS or DCIS. The term tends to erase and degrade people who are dying of incurable cancer. This idea of survivorship emphasizes and values longevity of life after diagnosis, while overlooking issues of quality of life.[3]
Some people reject the term survivor as being a narrow conceptualization of highly variable human experiences. Alternatives include alivers and thrivers, which put emphasis on living as well as possible, despite limitations and disability.[3] A third term, the diers, is used by some terminally ill patients who reject the claim that dying is part of survivorship or should be covered up with inappropriately optimistic language.[3]
The term previvor has been used to describe unaffected carriers. Unaffected carriers, or previvors, are those who have not been diagnosed with cancer, but who know that they are likely to develop cancer due to certain genetic mutations that form a known cancer syndrome. They have survived the predisposition, or higher risk, of cancer.[7][8] As such, this is the first generation in human history who, armed with information about a predisposition to a cancer after opting into DNA testing, can make informed choices prior to cancer diagnosis. The typical previvor has tested positive for a BRCA mutation and learned that she is at high risk for developing breast cancer and ovarian cancer, and is attempting to manage that risk through a combination of increased surveillance through mammograms, breast MRIs, pelvic ultrasounds, oophorectomy, bilateral mastectomy, and other medical procedures. There has been much controversy over the term previvor, due to the fact that the name compares these healthy women to people who have actually been diagnosed with invasive cancer.
Needs of cancer survivors
People who have finished cancer treatment often have psychological and physical medical challenges.[9] These effects can vary from person to person, change over time, and range in intensity from mild and intermittent to fully disabling. They commonly include fatigue,[10] pain,[10] sleep problems,[11] physical side effects like lymphoedema,[12] weight gain,[13] anxiety and depression,[14] fear of cancer recurrence,[15] and impaired quality of life.[16]
Psychosocial
Returning to life
If the treatment is lengthy and disruptive, many patients experience some difficulty in returning to normal daily life.[17] The energy needed to cope with a rigorous treatment program may have caused them to disconnect from previous daily patterns, such as working, normal self-care, and housekeeping. A small number of patients become dependent on the attention and sympathy that they received during their treatment and feel neglected when life returns to normal. There are tremendous implications that cancer has on the relationships that survivors have with their loved ones (particularly their partners) once their cancer has been treated,[18] and social support plays a critical role in their long-term emotional adjustment.[19]
Ongoing effects
Some survivors have to adjust to the idea that they will never be cured.
Some survivors, even if the cancer has been permanently cured, struggle emotionally from the trauma of having experienced a life-threatening disease.[20] Cancer survivors suffer from more psychological distress than those who have never experienced cancer (5.6% compared to 3.0%)[21] Serious psychosocial distress was seen 40% more among cancer survivors of five years or more than in those who have never had cancer.[21] About 10% develop major depressive disorder; others experience an adjustment disorder.[20] In young adult cancer survivors, one small study found that 20% of participants met the full clinical diagnosis of post-traumatic stress disorder (PTSD), and 45% to 95% displayed at least one symptom of PTSD.[22] Survivors of adult cancer are at an increased risk of suicidal ideology (having thoughts about suicide),[23] while as many as 13% of childhood cancer survivors experience suicidal ideology.[24] Issues of pain and physical ailments have been hypothesized as major contributing factors in cancer survivors experiencing this suicidal ideology.
Fear of cancer recurrence
Patients whose cancer is in remission may still have to cope with the uncertainty that at any time their cancer could return without warning. After the initial treatment has ended, anxiety is more common among cancer survivors than among other people.[25] This anxiety regarding the cancer's return is referred to as fear of cancer recurrence.[26] Many patients are anxious that any minor symptom indicates that the cancer has returned, with as many as 9 in 10 patients fearful that their cancer will recur or spread.[2] In addition to the appearance of any new aches and pains, common triggers for a fear that the cancer may return include hearing that someone else has been diagnosed with cancer, annual medical exams to determine whether the cancer recurred and news stories about cancer.[27] This anxiety leads to more medical check ups, which can be measured even after a period of up to ten years.[28] This fear can have a significant impact on individual's lives, resulting in difficulties in their daily life such as work and socialising, and difficulties planning for the future.[29] Overall, fear of cancer recurrence is related to a reduced quality of life in cancer survivors[29]
While Fear of Cancer Recurrence (FCR) can be adaptive at low levels, high levels of FCR require psychological treatment. At present, there are no psychometrically sound measures of FCR, which makes research into the effectiveness of treatment protocols difficult to interpret.[30] Treatments that are being investigated include: cognitive-behavioural therapy,[31] Meta-cognitive therapy[32] and Cognitive-existential group therapy[33] mindfulness-based interventions,[34] and exercise.[35]
Survivorship
The cultural ideal of a survivor may add to individual patients' distress if the patient is unable or unwilling to live up to the ideal.[3] As described by Gayle Sulik in her book Pink Ribbon Blues: How Breast Cancer Culture Undermines Women's Health, the ideal survivor is bravely committed to mainstream medicine and optimistic or even certain of a physical cure. She[Notes 1] is open about diagnosis and treatment and become an educated, empowered medical consumer. The ideal survivor, like a superwoman who simultaneously manages her home, family, and career, struggles valiantly to prevent cancer from affecting loved ones by appearing, behaving, and working as much as possible. Once the immediate crisis is past, the person may feel strongly pressured to donate time, money, and energy to cancer-related organizations. Above all, the ideal survivor does not die of cancer. People who publicly conform to this ideal are given social status and respect.[3]
Physical
In terms of medical challenges, some survivors experience cancer-related fatigue, may have long-term side effects from cancer and its treatment, and may need extensive rehabilitation for mobility and function if aggressive surgery was required to remove the cancer. They may experience temporary or persistent post-chemotherapy cognitive impairment. Some young survivors lose their ability to have children.
Cancer survivors frequently need medical monitoring, and some treatments for unrelated diseases in the future may be contraindicated. For example, a patient who has had a significant amount of radiation therapy may not be a good candidate for more radiation treatments in the future. To assist with these needs, "survivor care plans" have been promoted. These are personalized documents that describe the person's diagnosis and treatment in detail, list common known side effects, and specifically outline the steps that the survivor should take in the future, ranging from maintaining a healthy weight to receiving specific medical tests on a stated schedule.[36]
Medical tests to determine whether the cancer has returned commonly provoke fears. Informally, this is called scanxiety, a portmanteau of scan and anxiety. A desire to avoid feeling this fear can prompt survivors to postpone or refuse tests.[37][38] This may be able to be helped by the follow up of people who have had cancer post-treatment being undertaken via self-reported patient-related outcome measures rather than follow up visits but there is not enough controlled research looking into this.[39]
Survivors of childhood cancer have a life expectancy up to 28% shorter than people in the general population.[40] Therefore, there is a need to closely monitor these patients for much longer than usual. The Children's Oncology Group recommends that monitoring should include periodic follow up and screening by a clinician familiar with these patients' risks. Improving these patients' longevity requires recognition and treatment of illnesses associated with late effects in the decades after therapy for childhood cancer. For example, survivors of childhood cancer may have more difficulty than typical with breastfeeding and require more support to undertake this health-promoting activity.[41] Childhood cancer survivors are also at risk for developing adverse renal effects.[42] Others experience various forms of heart disease. One challenge to achieving this goal is that childhood cancer survivors are both very adaptable and accustomed to denying difficulties; as a result, they tend to minimize their symptoms. Therefore, internists may not give them all the attention they need and thus the actual help they may need. Symptom management, health promotion, specific attention to psychosocial needs, and surveillance for recurrence and specific late effects of treatment are helpful.[40] Health behaviour interventions may be able to reduce the impact of some of the chronic issues cancer survivors face by improving their dietary intake.[43] Likewise, physical exercise training interventions may have positive effects on physical fitness, including cardio-respiratory fitness, muscle strength and health-related quality of life.[44]
Adolescent and young adult survivors
Adolescent and young adult (AYA) survivors, often defined as being between the ages of 15 and 39, have seen advancements in technology and modern medicine causing a dramatic increase in the number of AYA survivors. Prior to 1970, being diagnosed with cancer during childhood was considered a universally fatal disease. From 1995 to 2000, however, the 5-year survival rate for children diagnosed with cancer was 80%.[45] Significant progress has been built in the last 25 years as there are now approximately 270,000 survivors of pediatric cancer in the U.S., which translates to approximately 1 in every 640 young adults being a survivor of childhood cancer.[46][47] However, as studies have shown, as patient needs increase, the likelihood of having an unmet need also increases.[48] For the AYA population, 2 out of 3 childhood cancer survivors will develop 1 complication due to the therapy they received and 1 out of 3 will develop serious or life-threatening complications, meaning they will most likely need treatment and follow-up care.[49] In addition, AYAs may experience greater difficulties adhering to treatment, which may negatively impact future outcomes.[50]
An AYA survivor faces a variety of issues as a result of their cancer diagnosis and treatment that are unique to their particular age group which differentiate their survivor population from the adult survivor population. For example, AYA survivors report that their education, employment, sexual functioning,[51] marriage, fertility, and other life values are impacted by their cancer.[52][53] Data show that AYA survivors have a much greater risk of getting a second primary malignancy as a side effect of the treatment for their original diagnosis. It is believed that AYAs have a much higher relative risk of developing a second primary cancer because the intensity of the treatment for their original diagnosis, typically including any combination of chemotherapy, surgery, and radiation, is much higher than the level of intensity given to patients over 40.[54] Furthermore, since AYA survivors are diagnosed and treated at such a young age, their length of time as a survivor is much longer than their adult counterparts, making it more likely they will face a second primary cancer in their lifetime.[54]
Barriers to quality long-term follow-up care
Childhood cancer survivors, in particular, need comprehensive long-term follow-up care to thrive. One way this can be accomplished is through continuous follow-up care with a primary care physician who is trained to identify possible late effects from previous treatments and therapies.[55]
The Children's Oncology Group (COG) has designed a set of survivorship guidelines that hope to aid both health care professionals and survivors themselves, in both the intricacies and basics of long-term follow-up care. The COG has guidelines for how a patient should put together their own "treatment summary", so they can have their treatment history with them when they visit any health care provider. The COG suggests that a survivor include the following in his/her treatment summary:
- Name of disease, date of diagnosis, stage of disease, contact information of the clinics/hospitals where you received your care
- Names and doses of the chemotherapy and radiation you have received and the area of the body that was radiated
- Names and dates of any surgeries you have had
- If you have received a transplant, the type of transplant and where it was received and whether you developed any chronic Graft-versus-Host Disease
- Names and dates of any significant complications and treatment received for those complications[56]
With the treatment summary, experts hope that survivors will be better equipped to face the significant burden of maintaining quality follow-up care long after their original treatment. This is especially important for the AYA population, in particular, because they are typically facing major social changes regarding their relationship status, employment or education status, their insurance coverage, and even their place of residence, etc. Typically, most of these factors are pretty constant for the adult population and if they experience any changes, it would occur in one or two aspects of their life. However, with the AYA population, the period of time until they are 40 is when they are going to, for the majority of the population, undergo the most change. This reality underscores the importance of a smooth transition from child-centered to adult-focused health care services through which they are consistently managed.[57]
Impact of Affordable Care Act on the AYA survivor population
The US Affordable Care Act (ACA) in 2010 makes it illegal for health insurance providers to deny coverage for a pre-existing condition, such as previously having survived cancer.[58] Young adults will now be required to have insurance coverage and, with a few exceptions, will be able to be covered under their parent's coverage until the age of 26 as a dependent in their parent's plan.[58]
Care
Studies among endometrial cancer survivors show that satisfaction with information provided about the disease and treatment increases the quality of life, lowers depression and results in less anxiety.[59] People who receive information on paper, compared to oral, indicate that they receive more information and are more satisfied about the information provided.[60] The American Institute of Medicine and the Dutch Health Council recommend the use of a Survivorship Care Plan; which is a summary of a patient's course of treatment, with recommendations for subsequent surveillance, management of late effects, and strategies for health promotion.[61]
Cancer survivors are encouraged to meet the same guidelines for physical activity as the rest of the population.[62][63] However, less than 1/3 of US cancer survivors met Physical Activity Guideline for Americans.[64] Increased physical activity reduces both all-cause and cancer-specific mortality in breast[65] and colo-rectal cancer survivors[66] as well as all cancer survivors.[64] In addition, sedentary behaviors, particularly prolonged sitting, were associated with worse survival outcomes.[64] Physical activity improves quality of life among a range of cancer survivors[67] and may also assist with cancer-related fatigue and common co-morbidities.[68][69]
Diet can also impact long-term mortality, with evidence across various cancer types.[70][71][72][73]
However, adherence to diet and exercise recommendations among cancer survivors is often poor.[74][75][76]
Digital behaviour change interventions can be successful at increasing physical activity and may also help with diet in cancer survivors.[77]
In breast cancer survivors, home-based multidimensional survivorship programmes have short term beneficial impacts on quality of life and can reduce anxiety, fatigue and insomnia.[78] Meta-analyses examining the effectiveness of mindfulness-based survivorship programs suggest it is an effective way to improve the mental health of cancer survivors.[79][80]
Family members
Family members can be significantly affected by the cancer experience of their loved ones.[81][82] For parents of children with cancer, finishing treatment can be a particularly vulnerable time. In the post-treatment period, some parents may experience increases in anxiety, depression and feelings of helplessness.[83] A sub-group of parents report post-traumatic stress symptoms up to years after treatment completion.[84] Evidence-based psychological interventions tailored to the needs of parents of childhood cancer survivors may assist parents in resuming their normal lives after their child has finished treatment.[85]
Spouses of cancer survivors are more likely than other people to experience anxiety in the years after their partner's successful treatment.[25]
See also
Notes
- ↑ Sulik was writing specifically about women survivors of breast cancer.
References
- ↑ Zwickey H, Schiffke HC (March 2007). "Genetic correlates of Chinese medicine: in search of a common language". Journal of Alternative and Complementary Medicine. 13 (2): 183–4. doi:10.1089/act.2007.13406. PMID 17388756.
- 1 2 "Cancer survivors face psychological challenges". Sun-Sentinel. Fort Lauderdale, Florida. 22 January 2009. Archived from the original on 23 April 2022. Retrieved 11 April 2022.
- 1 2 3 4 5 6 7 Sulik GA (2010). Pink Ribbon Blues: How Breast Cancer Culture Undermines Women's Health. USA: Oxford University Press. ISBN 978-0-19-974045-1. OCLC 535493589.
- ↑ Carr BI, Steel J, eds. (2013). Psychological aspects of cancer a guide to emotion and psychological consequences of cancer, their causes and their management. New York: Springer. p. 167. ISBN 9781461448662.
- ↑ "Living with or beyond cancer". Macmillan Cancer Support. Archived from the original on 16 July 2011. Retrieved 30 November 2010.
- 1 2 "DCCPS: OCS: About Cancer Survivorship Research: Survivorship Definitions". Office of Cancer Survivorship of the US National Cancer Institute. 6 November 2006. Archived from the original on 2 January 2011. Retrieved 30 November 2010.
- ↑ Harmon A (16 September 2007). "The DNA Age, Cancer Free at Age 33, but Weighing a Mastectomy". The New York Times. Archived from the original on 18 August 2021. Retrieved 16 September 2007.
- ↑ "FORCE | Special Populations : Cancer Previvors". Archived from the original on 25 July 2008. Retrieved 11 April 2022.
- ↑ "Living with cancer". Macmillan Cancer Support. Archived from the original on 19 April 2010. Retrieved 30 November 2010.
- 1 2 Weis J (August 2011). "Cancer-related fatigue: prevalence, assessment and treatment strategies". Expert Review of Pharmacoeconomics & Outcomes Research. 11 (4): 441–6. doi:10.1586/erp.11.44. PMID 21831025. S2CID 25361592.
- ↑ Sharma N, Hansen CH, O'Connor M, Thekkumpurath P, Walker J, Kleiboer A, et al. (September 2012). "Sleep problems in cancer patients: prevalence and association with distress and pain". Psycho-Oncology. 21 (9): 1003–9. doi:10.1002/pon.2004. PMID 21726015. S2CID 31925897.
- ↑ Hayes SC, Janda M, Cornish B, Battistutta D, Newman B (July 2008). "Lymphedema after breast cancer: incidence, risk factors, and effect on upper body function". Journal of Clinical Oncology. 26 (21): 3536–42. doi:10.1200/JCO.2007.14.4899. PMID 18640935.
- ↑ Koo HY, Seo YG, Cho MH, Kim MJ, Choi HC (2016). "Weight Change and Associated Factors in Long-Term Breast Cancer Survivors". PLOS ONE. 11 (7): e0159098. Bibcode:2016PLoSO..1159098K. doi:10.1371/journal.pone.0159098. PMC 4938573. PMID 27391162.
- ↑ Krebber AM, Buffart LM, Kleijn G, Riepma IC, de Bree R, Leemans CR, et al. (February 2014). "Prevalence of depression in cancer patients: a meta-analysis of diagnostic interviews and self-report instruments". Psycho-Oncology. 23 (2): 121–30. doi:10.1002/pon.3409. PMC 4282549. PMID 24105788.
- ↑ Simard S, Thewes B, Humphris G, Dixon M, Hayden C, Mireskandari S, Ozakinci G (September 2013). "Fear of cancer recurrence in adult cancer survivors: a systematic review of quantitative studies". Journal of Cancer Survivorship. 7 (3): 300–22. doi:10.1007/s11764-013-0272-z. PMID 23475398. S2CID 26655474.
- ↑ Quinten C, Coens C, Ghislain I, Zikos E, Sprangers MA, Ringash J, et al. (December 2015). "The effects of age on health-related quality of life in cancer populations: A pooled analysis of randomized controlled trials using the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 involving 6024 cancer patients" (PDF). European Journal of Cancer. 51 (18): 2808–19. doi:10.1016/j.ejca.2015.08.027. PMID 26602015. Archived (PDF) from the original on 4 March 2022. Retrieved 11 April 2022.
- ↑ Jennings D (29 June 2009). "Losing a Comforting Ritual: Treatment". The New York Times. Archived from the original on 6 May 2021. Retrieved 11 April 2022.
- ↑ Zhou ES, Kim Y, Rasheed M, Benedict C, Bustillo NE, Soloway M, et al. (December 2011). "Marital satisfaction of advanced prostate cancer survivors and their spousal caregivers: the dyadic effects of physical and mental health". Psycho-Oncology. 20 (12): 1353–7. doi:10.1002/pon.1855. PMC 3020233. PMID 20925137.
- ↑ Zhou ES, Penedo FJ, Bustillo NE, Benedict C, Rasheed M, Lechner S, et al. (2010). "Longitudinal effects of social support and adaptive coping on the emotional well-being of survivors of localized prostate cancer". The Journal of Supportive Oncology. 8 (5): 196–201. doi:10.1016/j.suponc.2010.09.004. PMC 3066633. PMID 21086876.
- 1 2 Smith S (14 August 2009). "Remy's woes befall many after cancer: Depression can hit as survivors adjust". Boston Globe. Archived from the original on 3 March 2016. Retrieved 11 April 2022.
- 1 2 Hoffman KE, McCarthy EP, Recklitis CJ, Ng AK (July 2009). "Psychological distress in long-term survivors of adult-onset cancer: results from a national survey". Archives of Internal Medicine. 169 (14): 1274–81. doi:10.1001/archinternmed.2009.179. PMID 19636028.
- Lay summary in: http://www.nhs.uk/Conditions/Eating-disorders/Pages/News.aspx?ListID=2&CurrentPage=4&NewsId={C162253C-016F-448B-8F80-CE88E5450022}.
{{cite journal}}: Cite journal requires|journal=(help); Missing or empty|title=(help)
- Lay summary in: http://www.nhs.uk/Conditions/Eating-disorders/Pages/News.aspx?ListID=2&CurrentPage=4&NewsId={C162253C-016F-448B-8F80-CE88E5450022}.
- ↑ Twombly R (February 2001). "Post-traumatic stress disorder in childhood cancer survivors: how common is it?". Journal of the National Cancer Institute. 93 (4): 262–3. doi:10.1093/jnci/93.4.262. PMID 11181770.
- ↑ Recklitis CJ, Diller LR, Li X, Najita J, Robison LL, Zeltzer L (February 2010). "Suicide ideation in adult survivors of childhood cancer: a report from the Childhood Cancer Survivor Study". Journal of Clinical Oncology. 28 (4): 655–61. doi:10.1200/JCO.2009.22.8635. PMC 2816000. PMID 19841325.
- ↑ Recklitis CJ, Lockwood RA, Rothwell MA, Diller LR (August 2006). "Suicidal ideation and attempts in adult survivors of childhood cancer". Journal of Clinical Oncology. 24 (24): 3852–7. doi:10.1200/JCO.2006.06.5409. PMID 16921037.
- Lay summary in: http://www.news.harvard.edu/gazette/2006/09.28/09-suicide.html.
{{cite journal}}: Cite journal requires|journal=(help); Missing or empty|title=(help)
- Lay summary in: http://www.news.harvard.edu/gazette/2006/09.28/09-suicide.html.
- 1 2 Mitchell AJ, Ferguson DW, Gill J, Paul J, Symonds P (July 2013). "Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: a systematic review and meta-analysis". The Lancet. Oncology. 14 (8): 721–32. doi:10.1016/S1470-2045(13)70244-4. PMID 23759376.
- Lay summary in: "Anxiety Lingers Long After Cancer". Anxiety Lingers Long After Cancer. 12 July 2013.
- ↑ Thewes B, Lebel S, Seguin Leclair C, Butow P (May 2016). "A qualitative exploration of fear of cancer recurrence (FCR) amongst Australian and Canadian breast cancer survivors". Supportive Care in Cancer. 24 (5): 2269–2276. doi:10.1007/s00520-015-3025-x. PMC 4805701. PMID 26581900.
- ↑ Gill KM, Mishel M, Belyea M, Germino B, Germino LS, Porter L, et al. (May 2004). "Triggers of uncertainty about recurrence and long-term treatment side effects in older African American and Caucasian breast cancer survivors". Oncology Nursing Forum. 31 (3): 633–9. doi:10.1188/04.ONF.633-639. PMID 15146229.
- ↑ Nicolaije KA, Ezendam NP, Vos MC, Boll D, Pijnenborg JM, Kruitwagen RF, et al. (May 2013). "Follow-up practice in endometrial cancer and the association with patient and hospital characteristics: a study from the population-based PROFILES registry". Gynecologic Oncology. 129 (2): 324–31. doi:10.1016/j.ygyno.2013.02.018. PMID 23435365.
- 1 2 Custers JA, Tielen R, Prins JB, de Wilt JH, Gielissen MF, van der Graaf WT (14 September 2015). "Fear of progression in patients with gastrointestinal stromal tumors (GIST): Is extended lifetime related to the Sword of Damocles?". Acta Oncologica. 54 (8): 1202–8. doi:10.3109/0284186X.2014.1003960. PMID 25734906. S2CID 6438769.
- ↑ Thewes B, Butow P, Zachariae R, Christensen S, Simard S, Gotay C (June 2012). "Fear of cancer recurrence: a systematic literature review of self-report measures". Psycho-Oncology. 21 (6): 571–87. doi:10.1002/pon.2070. PMID 22021099. S2CID 23735336.
- ↑ van de Wal MA, Gielissen MF, Servaes P, Knoop H, Speckens AE, Prins JB (2015). "Study protocol of the SWORD-study: a randomised controlled trial comparing combined online and face-to-face cognitive behaviour therapy versus treatment as usual in managing fear of cancer recurrence". BMC Psychology. 3 (1): 12. doi:10.1186/s40359-015-0068-1. PMC 4431367. PMID 25977758.
- ↑ Butow PN, Bell ML, Smith AB, Fardell JE, Thewes B, Turner J, et al. (April 2013). "Conquer fear: protocol of a randomised controlled trial of a psychological intervention to reduce fear of cancer recurrence". BMC Cancer. 13 (1): 201. doi:10.1186/1471-2407-13-201. PMC 3652728. PMID 23617696.
- ↑ Maheu C, Lebel S, Courbasson C, Lefebvre M, Singh M, Bernstein LJ, et al. (April 2016). "Protocol of a randomized controlled trial of the fear of recurrence therapy (FORT) intervention for women with breast or gynecological cancer". BMC Cancer. 16 (1): 291. doi:10.1186/s12885-016-2326-x. PMC 4845394. PMID 27112319.
- ↑ Subnis UB, Farb NA, Piedalue KL, Speca M, Lupichuk S, Tang PA, et al. (May 2020). "A Smartphone App-Based Mindfulness Intervention for Cancer Survivors: Protocol for a Randomized Controlled Trial". JMIR Research Protocols. 9 (5): e15178. doi:10.2196/15178. PMC 7248798. PMID 32390591.
- ↑ Brown JC, Damjanov N, Courneya KS, Troxel AB, Zemel BS, Rickels MR, et al. (April 2018). "A randomized dose-response trial of aerobic exercise and health-related quality of life in colon cancer survivors". Psycho-Oncology. 27 (4): 1221–1228. doi:10.1002/pon.4655. PMC 5895514. PMID 29388275.
- ↑ Neergaard L (23 October 2007). "'Survivor plans' a long-term cancer-treatment strategy". Associated Press. Archived from the original on 21 September 2010. Retrieved 11 April 2022.
- ↑ McCoyd JL, Kerson TS (2 March 2016). "Chapter 9". Social Work in Health Settings: Practice in Context. Routledge. ISBN 9781317409113. Archived from the original on 7 April 2022. Retrieved 11 April 2022.
- ↑ Feiler B (June 2011). "Scanxiety. Fear of a postcancer ritual". Time. 177 (24): 56. PMID 21682131. Archived from the original on 1 March 2022. Retrieved 11 April 2022.
- ↑ Nama V, Nordin A, Bryant A (November 2013). "Patient-reported outcome measures for follow-up after gynaecological cancer treatment". The Cochrane Database of Systematic Reviews. 2022 (11): CD010299. doi:10.1002/14651858.cd010299.pub2. PMC 6457831. PMID 24249483.
- 1 2 Yeh JM, Nekhlyudov L, Goldie SJ, Mertens AC, Diller L (April 2010). "A model-based estimate of cumulative excess mortality in survivors of childhood cancer". Annals of Internal Medicine. 152 (7): 409–17, W131-8. doi:10.7326/0003-4819-152-7-201004060-00005. PMC 3086591. PMID 20368646.
- Lay summary in: "Childhood Cancer Survivors Need Closer Monitoring in Adulthood". Childhood Cancer Survivors Need Closer Monitoring in Adulthood. 7 April 2010.
- ↑ Ogg SW, Hudson MM, Randolph ME, Klosky JL (June 2011). "Protective effects of breastfeeding for mothers surviving childhood cancer". Journal of Cancer Survivorship. 5 (2): 175–81. doi:10.1007/s11764-010-0169-z. PMID 21253880. S2CID 26613314.
- ↑ Kooijmans EC, Bökenkamp A, Tjahjadi NS, Tettero JM, van Dulmen-den Broeder E, van der Pal HJ, Veening MA (March 2019). "Early and late adverse renal effects after potentially nephrotoxic treatment for childhood cancer". The Cochrane Database of Systematic Reviews. 3: CD008944. doi:10.1002/14651858.cd008944.pub3. PMC 6410614. PMID 30855726.
- ↑ Cohen JE, Wakefield CE, Cohn RJ (August 2016). "Nutritional interventions for survivors of childhood cancer". The Cochrane Database of Systematic Reviews. 2016 (8): CD009678. doi:10.1002/14651858.cd009678.pub2. PMC 6486279. PMID 27545902.
- ↑ Braam KI, van der Torre P, Takken T, Veening MA, van Dulmen-den Broeder E, Kaspers GJ (March 2016). "Physical exercise training interventions for children and young adults during and after treatment for childhood cancer". The Cochrane Database of Systematic Reviews. 3: CD008796. doi:10.1002/14651858.cd008796.pub3. PMC 6464400. PMID 27030386.
- ↑ Ries LA, Eisener MP, Kosary CL (2004). "SEER cancer statistics review, 1975-2001". National Cancer Institute.
- ↑ Aziz NM, Oeffinger KC, Brooks S, Turoff AJ (August 2006). "Comprehensive long-term follow-up programs for pediatric cancer survivors". Cancer. 107 (4): 841–8. doi:10.1002/cncr.22096. PMID 16886175.
- ↑ Hewitt M, Weisner SL, Simone JV (2003). Childhood cancer survivorship: Improving care and quality of life. Washington, D.C.: National Academies Press.
- ↑ Heinrich RL, Schag CC, Ganz PA (July 1984). "Living with cancer: the Cancer Inventory of Problem Situations". Journal of Clinical Psychology. 40 (4): 972–80. doi:10.1002/1097-4679(198407)40:4<972::aid-jclp2270400417>3.0.co;2-w. PMID 6480863.
- ↑ Oeffinger KC, Hudson MM (2004). "Long-term complications following childhood and adolescent cancer: foundations for providing risk-based health care for survivors". CA: A Cancer Journal for Clinicians. 54 (4): 208–36. doi:10.3322/canjclin.54.4.208. PMID 15253918.
- ↑ Butow P, Palmer S, Pai A, Goodenough B, Luckett T, King M (November 2010). "Review of adherence-related issues in adolescents and young adults with cancer". Journal of Clinical Oncology. 28 (32): 4800–4809. doi:10.2147/coaya.s85988. PMID 20212260.
- ↑ Bober SL, Zhou ES, Chen B, Manley PE, Kenney LB, Recklitis CJ (August 2013). "Sexual function in childhood cancer survivors: a report from Project REACH". The Journal of Sexual Medicine. 10 (8): 2084–93. doi:10.1111/jsm.12193. PMID 23679087.
- ↑ Zebrack BJ, Zeltzer LK (2003). "Quality of life issues and cancer survivorship". Current Problems in Cancer. 27 (4): 198–211. CiteSeerX 10.1.1.170.8566. doi:10.1016/s0147-0272(03)00027-8. PMID 12855951.
- ↑ Robertson EG, Sansom-Daly UM, Wakefield CE, Ellis SJ, McGill BC, Doolan EL, Cohn RJ (September 2016). "Sexual and Romantic Relationships: Experiences of Adolescent and Young Adult Cancer Survivors". Journal of Adolescent and Young Adult Oncology. 5 (3): 286–91. doi:10.1089/jayao.2015.0061. PMID 26885746.
- 1 2 Soliman H, Agresta SV (January 2008). "Current issues in adolescent and young adult cancer survivorship". Cancer Control. 15 (1): 55–62. doi:10.1177/107327480801500107. PMID 18094661.
- ↑ American Academy of Pediatrics Section on Hematology/Oncology Children's Oncology Group (March 2009). "Long-term follow-up care for pediatric cancer survivors". Pediatrics. 123 (3): 906–15. doi:10.1542/peds.2008-3688. PMC 2696806. PMID 19255020.
- ↑ "Introduction to Long-term Follow-Up after Treatment for Childhood, Adolescent, or Young Adult Cancer" (PDF). Children's Oncology Group. 2008. Archived (PDF) from the original on 21 January 2012. Retrieved 1 February 2012.
- ↑ Freyer DR (November 2010). "Transition of care for young adult survivors of childhood and adolescent cancer: rationale and approaches". Journal of Clinical Oncology. 28 (32): 4810–8. doi:10.1200/jco.2009.23.4278. PMC 3018346. PMID 20351333.
- 1 2 "Summary of New Health Reform Law" (PDF). Kaiser Family Foundation. Archived (PDF) from the original on 17 January 2013. Retrieved 2 February 2012.
- ↑ Husson O, Mols F, van de Poll-Franse LV (April 2011). "The relation between information provision and health-related quality of life, anxiety and depression among cancer survivors: a systematic review". Annals of Oncology. 22 (4): 761–72. doi:10.1093/annonc/mdq413. PMC 3065875. PMID 20870912.
- ↑ Nicolaije KA, Husson O, Ezendam NP, Vos MC, Kruitwagen RF, Lybeert ML, van de Poll-Franse LV (September 2012). "Endometrial cancer survivors are unsatisfied with received information about diagnosis, treatment and follow-up: a study from the population-based PROFILES registry" (PDF). Patient Education and Counseling. 88 (3): 427–35. doi:10.1016/j.pec.2012.05.002. PMID 22658248. Archived (PDF) from the original on 19 July 2018. Retrieved 11 April 2022.
- ↑ van de Poll-Franse LV, Nicolaije KA, Vos MC, Pijnenborg JM, Boll D, Husson O, et al. (December 2011). "The impact of a cancer Survivorship Care Plan on gynecological cancer patient and health care provider reported outcomes (ROGY Care): study protocol for a pragmatic cluster randomized controlled trial". Trials. 12: 256. doi:10.1186/1745-6215-12-256. PMC 3286432. PMID 22141750.
- ↑ "Physical activity guidelines for Americans" (PDF). U.S. Department of Health and Human Services. 2008. Archived (PDF) from the original on 18 October 2018. Retrieved 11 April 2022.
- ↑ Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, Galvão DA, Pinto BM, et al. (July 2010). "American College of Sports Medicine roundtable on exercise guidelines for cancer survivors". Medicine and Science in Sports and Exercise. 42 (7): 1409–26. doi:10.1249/MSS.0b013e3181e0c112. PMID 20559064.
- 1 2 3 Cao C, Friedenreich CM, Yang L (March 2022). "Association of Daily Sitting Time and Leisure-Time Physical Activity With Survival Among US Cancer Survivors". JAMA Oncology. 8 (3): 395–403. doi:10.1001/jamaoncol.2021.6590. PMC 8739832. PMID 34989765.
{{cite journal}}: CS1 maint: PMC embargo expired (link) - ↑ Lahart IM, Metsios GS, Nevill AM, Carmichael AR (May 2015). "Physical activity, risk of death and recurrence in breast cancer survivors: A systematic review and meta-analysis of epidemiological studies". Acta Oncologica. 54 (5): 635–54. doi:10.3109/0284186X.2014.998275. hdl:2436/346757. PMID 25752971. S2CID 7965866.
- ↑ Schmid D, Leitzmann MF. Association between physical activity and mortality among breast cancer and colorectal cancer survivors: a systematic review and meta-analysis. Ann Oncol. 2014;25(7):1293–311.
- ↑ Mishra SI, Scherer RW, Geigle PM, et al. Exercise interventions on health-related quality of life for cancer survivors. Cochrane Database Syst Rev. 2012;8:CD007566.
- ↑ van Roekel EH, Winkler EA, Bours MJ, Lynch BM, Willems PJ, Meijer K, et al. (December 2016). "Associations of sedentary time and patterns of sedentary time accumulation with health-related quality of life in colorectal cancer survivors". Preventive Medicine Reports. 4: 262–9. doi:10.1016/j.pmedr.2016.06.022. PMC 4941044. PMID 27419042.
- ↑ Phillips SM, Lloyd GR, Awick EA, McAuley E (June 2016). "Correlates of objectively measured sedentary behavior in breast cancer survivors". Cancer Causes & Control. 27 (6): 787–95. doi:10.1007/s10552-016-0756-z. PMC 5507361. PMID 27146839.
- ↑ Xing MY, Xu SZ, Shen P (2014). "Effect of low-fat diet on breast cancer survival: a meta-analysis". Asian Pacific Journal of Cancer Prevention. 15 (3): 1141–4. doi:10.7314/apjcp.2014.15.3.1141. PMID 24606431.
- ↑ Brennan SF, Woodside JV, Lunny PM, Cardwell CR, Cantwell MM (July 2017). "Dietary fat and breast cancer mortality: A systematic review and meta-analysis" (PDF). Critical Reviews in Food Science and Nutrition. 57 (10): 1999–2008. doi:10.1080/10408398.2012.724481. PMID 25692500. S2CID 34098509. Archived (PDF) from the original on 4 September 2021. Retrieved 11 April 2022.
- ↑ Meyerhardt JA, Niedzwiecki D, Hollis D, Saltz LB, Hu FB, Mayer RJ, et al. (August 2007). "Association of dietary patterns with cancer recurrence and survival in patients with stage III colon cancer". JAMA. 298 (7): 754–64. doi:10.1001/jama.298.7.754. PMID 17699009.
- ↑ Schwingshackl L, Hoffmann G (December 2015). "Adherence to Mediterranean diet and risk of cancer: an updated systematic review and meta-analysis of observational studies". Cancer Medicine. 4 (12): 1933–47. doi:10.1002/cam4.539. PMC 5123783. PMID 26471010.
- ↑ Winkels RM, van Lee L, Beijer S, Bours MJ, van Duijnhoven FJ, Geelen A, et al. (September 2016). "Adherence to the World Cancer Research Fund/American Institute for Cancer Research lifestyle recommendations in colorectal cancer survivors: results of the PROFILES registry". Cancer Medicine. 5 (9): 2587–95. doi:10.1002/cam4.791. PMC 5055169. PMID 27418442.
- ↑ Blanchard CM, Courneya KS, Stein K (May 2008). "Cancer survivors' adherence to lifestyle behavior recommendations and associations with health-related quality of life: results from the American Cancer Society's SCS-II". Journal of Clinical Oncology. 26 (13): 2198–204. doi:10.1200/JCO.2007.14.6217. PMID 18445845.
- ↑ Williams K, Steptoe A, Wardle J (June 2013). "Is a cancer diagnosis a trigger for health behaviour change? Findings from a prospective, population-based study". British Journal of Cancer. 108 (11): 2407–12. doi:10.1038/bjc.2013.254. PMC 3681023. PMID 23695026.
- ↑ Roberts AL, Fisher A, Smith L, Heinrich M, Potts HW (December 2017). "Digital health behaviour change interventions targeting physical activity and diet in cancer survivors: a systematic review and meta-analysis". Journal of Cancer Survivorship. 11 (6): 704–719. doi:10.1007/s11764-017-0632-1. PMC 5671545. PMID 28779220.
- ↑ Cheng KK, Lim YT, Koh ZM, Tam WW (August 2017). "Home-based multidimensional survivorship programmes for breast cancer survivors". The Cochrane Database of Systematic Reviews. 2017 (8): CD011152. doi:10.1002/14651858.cd011152.pub2. PMC 6483678. PMID 28836379.
- ↑ Cramer H, Lauche R, Paul A, Dobos G (October 2012). "Mindfulness-based stress reduction for breast cancer-a systematic review and meta-analysis". Current Oncology. 19 (5): e343-52. doi:10.3747/co.19.1016. PMC 3457885. PMID 23144582. Archived from the original on 27 September 2020. Retrieved 11 April 2022.
- ↑ Zainal NZ, Booth S, Huppert FA (July 2013). "The efficacy of mindfulness-based stress reduction on mental health of breast cancer patients: a meta-analysis". Psycho-Oncology. 22 (7): 1457–65. doi:10.1002/pon.3171. PMID 22961994.
- ↑ Girgis A, Lambert S, Johnson C, Waller A, Currow D (July 2013). "Physical, psychosocial, relationship, and economic burden of caring for people with cancer: a review". Journal of Oncology Practice. 9 (4): 197–202. doi:10.1200/JOP.2012.000690. PMC 3710169. PMID 23942921.
- ↑ Wakefield CE, Drew D, Ellis SJ, Doolan EL, McLoone JK, Cohn RJ (March 2014). "'What they're not telling you': a new scale to measure grandparents' information needs when their grandchild has cancer". Patient Education and Counseling. 94 (3): 351–5. doi:10.1016/j.pec.2013.10.030. PMID 24315159.
- ↑ Wijnberg-Williams BJ, Kamps WA, Klip EC, Hoekstra-Weebers JE (January 2006). "Psychological adjustment of parents of pediatric cancer patients revisited: five years later". Psycho-Oncology (Submitted manuscript). 15 (1): 1–8. doi:10.1002/pon.927. hdl:11370/e9249a8a-c4e9-478d-92e5-909bc886356e. PMID 15880477. S2CID 31950002. Archived from the original on 5 August 2020. Retrieved 11 April 2022.
- ↑ Ljungman L, Cernvall M, Grönqvist H, Ljótsson B, Ljungman G, von Essen L (24 July 2014). Stemmer SM (ed.). "Long-term positive and negative psychological late effects for parents of childhood cancer survivors: a systematic review". PLOS ONE. 9 (7): e103340. Bibcode:2014PLoSO...9j3340L. doi:10.1371/journal.pone.0103340. PMC 4110004. PMID 25058607.
- ↑ Wakefield CE, Sansom-Daly UM, McGill BC, McCarthy M, Girgis A, Grootenhuis M, et al. (April 2015). "Online parent-targeted cognitive-behavioural therapy intervention to improve quality of life in families of young cancer survivors: study protocol for a randomised controlled trial". Trials. 16 (1): 153. doi:10.1186/s13063-015-0681-6. PMC 4395969. PMID 25872773.
External links
- Information about survivorship Archived 6 August 2012 at the Wayback Machine at Cancer.Net by the American Society of Clinical Oncology
- National Coalition for Cancer Survivorship Archived 9 April 2022 at the Wayback Machine