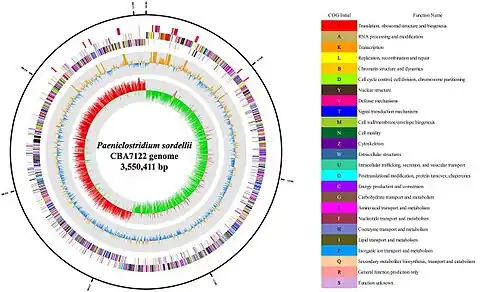
Paeniclostridium sordellii
| Paeniclostridium sordellii | |
|---|---|
| Scientific classification | |
| Domain: | Bacteria |
| Phylum: | Bacillota |
| Class: | Clostridia |
| Order: | Eubacteriales |
| Family: | Clostridiaceae |
| Genus: | Paeniclostridium |
| Species: | P. sordellii |
| Binomial name | |
| Paeniclostridium sordellii (Hall and Scott, 1927) Sasi Jyothsna et al. 2016 | |
| Synonyms | |
| |
Paeniclostridium sordellii is a rare anaerobic, gram-positive, spore-forming rod with peritrichous flagella that is capable of causing pneumonia, endocarditis, arthritis, peritonitis, and myonecrosis. C. sordellii bacteremia and sepsis occur rarely. Most cases of sepsis from C. sordellii occur in patients with underlying conditions. Severe toxic shock syndrome among previously healthy persons has been described in a small number of C. sordellii cases, most often associated with gynecologic infections in women and infection of the umbilical stump in newborns. It has also been described in post-partum females, medically induced abortions, injection drug users and trauma cases.[1] So far, all documented post-partum females who contracted C. sordellii septicaemia have died, and all but one woman who contracted the bacterium post-abortion have died .
Infection
The source of the bacteria has not been determined but it has been documented that about 0.5% to 10% of healthy women are lengthened vaginal carriage of C. sordellii.[2] There are several clinical features which are unique to C. sordellii: marked leukocytosis (leukaemoid reaction), refractory hypotension, severe tachycardia, haemoconcentration, persistent apyrexia and profound capillary leak syndrome (see entry for Clostridium novyi alpha-toxin for details of mechanism). In terms of management, there is no hard and fast rule, as with most bacterial pathogens, but past data reveals C. sordellii susceptibility to beta-lactams, clindamycin, tetracycline and chloramphenicol but resistant to aminoglycosides and sulphonamides.[3]
References
- ↑ M. J. Aldape, A. E. Bryant, D. L. Stevens; Clostridium sordellii Infection: Epidemiology, Clinical Findings, and Current Perspectives on Diagnosis and Treatment; Clinical Infectious Diseases 2006; 43:1436-46
- ↑ Miech RP. Pathophysiology of mifepristone-induced septic shock due to Clostridium sordellii. Ann Pharmacother 2005; 39:1483-8
- ↑ Nakamura S, Yamakawa K, Nishida S. Antibacterial susceptibility of Clostridium sordellii strains. Zentralbl Bakteriol Mikrobiol Hyg [A] 1986; 261:345-9.
External links
- McGregor.pdf Archived 2017-05-31 at the Wayback Machine
- Pathema-Clostridium Resource
- Type strain of Clostridium sordellii at BacDive - the Bacterial Diversity Metadatabase Archived 2017-01-11 at the Wayback Machine