Frostbite
| Frostbite | |
|---|---|
| Other names: Frostnip | |
 | |
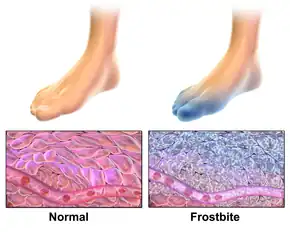
| Frostbitten toes two to three days after mountain climbing | |
| Specialty | Emergency medicine, orthopedics |
| Symptoms | Numbness, feeling cold, clumsy, pale color[1] |
| Complications | Hypothermia, compartment syndrome[2][1] |
| Types | Superficial, deep[2] |
| Causes | Temperatures below freezing[1] |
| Risk factors | Alcohol, smoking, mental health problems, certain medications, prior cold injury[1] |
| Diagnostic method | Based on symptoms[3] |
| Differential diagnosis | Frostnip, pernio, trench foot[4] |
| Prevention | Avoid cold, wear proper clothing, maintain hydration and nutrition, stay active without becoming exhausted[2] |
| Treatment | Rewarming, medication, surgery[2] |
| Medication | Ibuprofen, tetanus vaccine, iloprost, thrombolytics[1][5] |
| Frequency | Unknown[6] |
Frostbite occurs when exposure to low temperatures causes freezing of the skin or other tissues.[1] The initial symptom is typically numbness.[1] This may be followed by clumsiness with a white or bluish color to the skin.[1] Swelling or blistering may occur following treatment.[1] The hands, feet, and face are most commonly affected.[4] Complications may include hypothermia, compartment syndrome, and chronic pain.[2][1][5]
People who are exposed to low temperatures for prolonged periods, such as winter sports enthusiasts, military personnel, and homeless individuals, are at greatest risk.[7][1] Other risk factors include drinking alcohol, smoking, mental health problems, certain medications, and prior injuries due to cold.[1] The underlying mechanism involves injury from ice crystals and blood clots in small blood vessels following thawing.[1] Diagnosis is based on symptoms.[3] Severity may be divided into superficial (1st and 2nd degree) or deep (3rd and 4th degree).[2] A bone scan or MRI may help in determining the extent of injury.[1]
Prevention is through wearing proper clothing, maintaining hydration and nutrition, avoiding low temperatures, and staying active without becoming exhausted.[2] Treatment is by rewarming.[2] This should be done only when refreezing is not a concern.[1] Rubbing or applying snow to the affected part is not recommended.[2] The use of ibuprofen and tetanus toxoid is typically recommended.[1] For severe injuries iloprost or thrombolytics may be used.[1][5] Surgery is sometimes necessary.[1] Amputation, however, should generally be delayed for a few months to allow determination of the extent of injury.[2]
The number of cases of frostbite is unknown.[6] Rates may be as high as 40% a year among those who mountaineer.[1] The most common age group affected is those 30 to 50 years old.[4] Evidence of frostbite occurring in people dates back 5,000 years.[1] Frostbite has also played an important role in a number of military conflicts.[1] The first formal description of the condition was in 1813 by Dominique Jean Larrey, a physician in Napoleon's army, during its invasion of Russia.[1]
Signs and symptoms
Areas that are usually affected include cheeks, ears, nose and fingers and toes. Frostbite is often preceded by frostnip.[2] The symptoms of frostbite progress with prolonged exposure to cold. Historically, frostbite has been classified by degrees according to skin and sensation changes, similar to burn classifications. However, the degrees do not correspond to the amount of long term damage.[8] A simplification of this system of classification is superficial (first or second degree) or deep injury (third or fourth degree).[9]
First degree
- First degree frostbite is superficial, surface skin damage that is usually not permanent.
- Early on, the primary symptom is loss of feeling in the skin. In the affected areas, the skin is numb, and possibly swollen, with a reddened border.
- In the weeks after injury, the skin's surface may slough off.[8]
Second degree
Third degree

- In third degree frostbite, the layers of tissue below the skin freeze.
- Symptoms include blood blisters and "blue-grey discoloration of the skin".
- In the weeks after injury, pain persists and a blackened crust (eschar) develops.
- There can be longterm ulceration and damage to growth plates.[8]
Fourth degree

- In fourth degree frostbite, structures below the skin are involved like muscles, tendon, and bone.
- Early symptoms include a colorless appearance of the skin, a hard texture, and painless rewarming.
- Later, the skin becomes black and mummified. The amount of permanent damage can take one month or more to determine. Autoamputation can occur after two months.[8]
Causes
Risk factors
The major risk factor for frostbite is exposure to cold through geography, occupation and/or recreation. Inadequate clothing and shelter are major risk factors. Frostbite is more likely when the body's ability to produce or retain heat is impaired. Physical, behavioral, and environmental factors can all contribute to the development of frostbite. Immobility and physical stress (such as malnutrition or dehydration) are also risk factors.[7] Disorders and substances that impair circulation contribute, including diabetes, Raynaud's phenomenon, tobacco and alcohol use.[9] Homeless individuals and individuals with some mental illnesses may be at higher risk.[7]
Mechanism
Freezing
In frostbite, cooling of the body causes narrowing of the blood vessels (vasoconstriction). Temperatures below −4 °C (25 °F) are required to form ice crystals in the tissues.[9] The process of freezing causes ice crystals to form in the tissue, which in turn causes damage at the cellular level. Ice crystals can damage cell membranes directly.[10] In addition, ice crystals can damage small blood vessels at the site of injury.[9] Scar tissue forms when fibroblasts replace the dead cells.[10]
Rewarming
Rewarming causes tissue damage through reperfusion injury, which involves vasodilation, swelling (edema), and poor blood flow (stasis). Platelet aggregation is another possible mechanism of injury. Blisters and spasm of blood vessels (vasospasm) can develop after rewarming.[9]
Non-freezing cold injury
The process of frostbite differs from the process of non-freezing cold injury (NFCI). In NFCI, temperature in the tissue decreases gradually. This slower temperature decrease allows the body to try to compensate through alternating cycles of closing and opening blood vessels (vasoconstriction and vasodilation). If this process continues, inflammatory mast cells act in the area. Small clots (microthrombi) form and can cut off blood to the affected area (known as ischemia) and damage nerve fibers. Rewarming causes a series of inflammatory chemicals such as prostaglandins to increase localized clotting.[10]
Pathophysiology
The pathological mechanism by which frostbite causes body tissue injury can be characterized by four stages: Prefreeze, freeze-thaw, vascular stasis, and the late ischemic stage.[11]
- Prefreeze phase: involves the cooling of tissues without ice crystal formation.[11]
- Freeze-thaw phase: ice-crystals form, resulting in cellular damage and death.[11]
- Vascular stasis phase: marked by blood coagulation or the leaking of blood out of the vessels.[11]
- Late ischemic phase: characterized by inflammatory events, ischemia and tissue death.[11]
Diagnosis
Frostbite is diagnosed based on signs and symptoms as described above, and by patient history. Other conditions that can have a similar appearance or occur at the same time include:
- Frostnip is similar to frostbite, but without ice crystal formation in the skin. Whitening of the skin and numbness reverse quickly after rewarming.
- Trench foot is damage to nerves and blood vessels that results exposure to wet, cold (non-freezing) conditions. This is reversible if treated early.
- Pernio or chilblains are inflammation of the skin from exposure to wet, cold (non-freezing) conditions. They can appear as various types of ulcers and blisters.[8]
- Bullous pemphigoid is a condition that causes itchy blisters over the body that can mimic frostbite.[12] It does not require exposure to cold to develop.
- Levamisole toxicity is a vasculitis that can appear similar to frostbite.[12] It is caused by contamination of cocaine by levamisole. Skin lesions can look similar those of frostbite, but do not require cold exposure to occur.
People who have hypothermia often have frostbite as well.[8] Since hypothermia is life-threatening this should be treated first. Technetium-99 or MR scans are not required for diagnosis, but might be useful for prognostic purposes.[13]
Prevention
The Wilderness Medical Society recommends covering the skin and scalp, taking in adequate nutrition, avoiding constrictive footwear and clothing, and remaining active without causing exhaustion. Supplemental oxygen might also be of use at high elevations. Repeated exposure to cold water makes people more susceptible to frostbite.[14] Additional measures to prevent frostbite include:[2]
- Avoiding temperatures below −15 °C (5 °F)
- Avoiding moisture, including in the form of sweat and/or skin emollients
- Avoiding alcohol and drugs that impair circulation or natural protective responses
- Layering clothing
- Using chemical or electric warming devices
- Recognizing early signs of frostnip and frostbite[2]
Treatment
Individuals with frostbite or potential frostbite should go to a protected environment and get warm fluids. If there is no risk of re-freezing, the extremity can be exposed and warmed in the groin or underarm of a companion. If the area is allowed to refreeze, there can be worse tissue damage. If the area cannot be reliably kept warm, the person should be brought to a medical facility without rewarming the area. Rubbing the affected area can also increase tissue damage. Aspirin and ibuprofen can be given in the field[7] to prevent clotting and inflammation. Ibuprofen is often preferred to aspirin because aspirin may block a subset of prostaglandins that are important in injury repair.[15]
The first priority in people with frostbite should be to assess for hypothermia and other life-threatening complications of cold exposure. Before treating frostbite, the core temperature should be raised above 35 °C. Oral or intravenous (IV) fluids should be given.[7]
Other considerations for standard hospital management include:
- wound care: blisters can be drained by needle aspiration, unless they are bloody (hemorrhagic). Aloe vera gel can be applied before breathable, protective dressings or bandages are put on.
- antibiotics: if there is trauma, skin infection (cellulitis) or severe injury
- tetanus toxoid: should be administered according to local guidelines. Uncomplicated frostbite wounds are not known to encourage tetanus.
- pain control: NSAIDs or opioids are recommended during the painful rewarming process.
Rewarming
If the area is still partially or fully frozen, it should be rewarmed in the hospital with a warm bath with povidone iodine or chlorhexidine antiseptic.[7] Active rewarming seeks to warm the injured tissue as quickly as possible without burning. The faster tissue is thawed, the less tissue damage occurs.[16] According to Handford and colleagues, "The Wilderness Medical Society and State of Alaska Cold Injury Guidelines recommend a temperature of 37–39 °C, which decreases the pain experienced by the patient whilst only slightly slowing rewarming time." Warming takes 15 minutes to 1 hour. Rewarming can be very painful, so pain management is important.[7]
Medications

People with potential for large amputations and who present within 24 hours of injury can be given TPA with heparin.[1] These medications should be withheld if there are any contraindications. Bone scans or CT angiography can be done to assess damage.[17]
Blood vessel dilating medications such as iloprost may prevent blood vessel blockage.[7] This treatment might be appropriate in grades 2–4 frostbite, when people get treatment within 48 hours.[17] In addition to vasodilators, sympatholytic drugs can be used to counteract the detrimental peripheral vasoconstriction that occurs during frostbite.[18]
Surgery
Various types of surgery might be indicated in frostbite injury, depending on the type and extent of damage. Debridement or amputation of necrotic tissue is usually delayed unless there is gangrene or systemic infection (sepsis).[7] This has led to the adage "Frozen in January, amputate in July".[19] If symptoms of compartment syndrome develop, fasciotomy can be done to attempt to preserve blood flow.[7]
Prognosis

Tissue loss and autoamputation are potential consequences of frostbite. Permanent nerve damage including loss of feeling can occur. It can take several weeks to know what parts of the tissue will survive.[9] Time of exposure to cold is more predictive of lasting injury than temperature the individual was exposed to. The classification system of grades, based on the tissue response to initial rewarming and other factors is designed to predict degree of longterm recovery.[7]
Grades
Grade 1: if there is no initial lesion on the area, no amputation or lasting effects are expected
Grade 2: if there is a lesion on the distal body part, tissue and fingernails can be destroyed
Grade 3: if there is a lesion on the intermediate or near body part, autoamputation and loss of function can occur
Grade 4: if there is a lesion very near the body (such as the carpals of the hand), the limb can be lost. Sepsis and/or other systemic problems are expected.[7]
A number of long term sequelae can occur after frostbite. These include transient or permanent changes in sensation, paresthesia, increased sweating, cancers, and bone destruction/arthritis in the area affected.[20]
Epidemiology
There is a lack of comprehensive statistics about the epidemiology of frostbite. In the United States, frostbite is more common in northern states. In Finland, annual incidence was 2.5 per 100,000 among civilians, compared with 3.2 per 100,000 in Montreal. Research suggests that men aged 30–49 are at highest risk, possibly due to occupational or recreational exposures to cold.[21]
History
Frostbite has been described in military history for millennia. The Greeks encountered and discussed the problem of frostbite as early as 400 BCE.[9] Researchers have found evidence of frostbite in humans dating back 5,000 years, in an Andean mummy. Napoleon's Army was the first documented instance of mass cold injury in the early 1800s.[7] According to Zafren, nearly 1 million combatants fell victim to frostbite in the First and Second World Wars, and the Korean War.[9]
Society and culture

Several notable cases of frostbite include: Captain Lawrence Oates, an English army captain and Antarctic explorer who in 1912 died of complications of frostbite;[22] noted American rock climber Hugh Herr, who in 1982 lost both legs below the knee to frostbite after being stranded on Mount Washington (New Hampshire) in a blizzard;[23] Beck Weathers, a survivor of the 1996 Mount Everest disaster who lost his nose and hands to frostbite;[24] Scottish mountaineer Jamie Andrew, who in 1999 had all four limbs amputated due to sepsis from frostbite sustained after becoming trapped for four nights whilst climbing Les Droites in the Mont Blanc massif.[25]
Research directions
Evidence is insufficient to determine whether or not hyperbaric oxygen therapy as an adjunctive treatment can assist in tissue salvage.[26] Cases have been reported, but no randomized control trial has been performed on humans.[27][28][29][30][31]
Medical sympathectomy using intravenous reserpine has also been attempted with limited success.[20] Studies have suggested that administration of tissue plasminogen activator (tPa) either intravenously or intra-arterially may decrease the likelihood of eventual need for amputation.[32]
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Handford, C; Thomas, O; Imray, CHE (May 2017). "Frostbite". Emergency Medicine Clinics of North America. 35 (2): 281–299. doi:10.1016/j.emc.2016.12.006. PMID 28411928.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 McIntosh, Scott E.; Opacic, Matthew; Freer, Luanne; Grissom, Colin K.; Auerbach, Paul S.; Rodway, George W.; Cochran, Amalia; Giesbrecht, Gordon G.; McDevitt, Marion (2014-12-01). "Wilderness Medical Society practice guidelines for the prevention and treatment of frostbite: 2014 update". Wilderness & Environmental Medicine. 25 (4 Suppl): S43–54. doi:10.1016/j.wem.2014.09.001. ISSN 1545-1534. PMID 25498262.
- 1 2 Singleton, Joanne K.; DiGregorio, Robert V.; Green-Hernandez, Carol (2014). Primary Care, Second Edition: An Interprofessional Perspective. Springer Publishing Company. p. 172. ISBN 9780826171474. Archived from the original on 2020-08-01. Retrieved 2020-06-07.
- 1 2 3 Ferri, Fred F. (2017). Ferri's Clinical Advisor 2018 E-Book: 5 Books in 1. Elsevier Health Sciences. p. 502. ISBN 9780323529570. Archived from the original on 2020-08-01. Retrieved 2020-06-07.
- 1 2 3 Sheridan, Robert L.; Goverman, Jeremy M.; Walker, T. Gregory (9 June 2022). "Diagnosis and Treatment of Frostbite". New England Journal of Medicine. 386 (23): 2213–2220. doi:10.1056/NEJMra1800868. PMID 35675178.
- 1 2 Auerbach, Paul S. (2011). Wilderness Medicine E-Book: Expert Consult Premium Edition - Enhanced Online Features. Elsevier Health Sciences. p. 181. ISBN 978-1455733569. Archived from the original on 2020-08-01. Retrieved 2020-06-07.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Handford, Charles; Buxton, Pauline; Russell, Katie; Imray, Caitlin EA; McIntosh, Scott E; Freer, Luanne; Cochran, Amalia; Imray, Christopher HE (2014-04-22). "Frostbite: a practical approach to hospital management". Extreme Physiology & Medicine. 3: 7. doi:10.1186/2046-7648-3-7. ISSN 2046-7648. PMC 3994495. PMID 24764516.
- 1 2 3 4 5 6 7 "Frostbite Clinical Presentation". emedicine.medscape.com. Archived from the original on 2017-03-02. Retrieved 2017-03-02.
- 1 2 3 4 5 6 7 8 Zafren, Ken (2013). "Frostbite: Prevention and Initial Management". High Altitude Medicine & Biology. 14 (1): 9–12. doi:10.1089/ham.2012.1114. PMID 23537254. S2CID 3036889.
- 1 2 3 Sachs, Christoph; Lehnhardt, Marcus; Daigeler, Adrien; Goertz, Ole (2017-03-01). "The Triaging and Treatment of Cold-Induced Injuries". Deutsches Ärzteblatt International. 112 (44): 741–747. doi:10.3238/arztebl.2015.0741. ISSN 1866-0452. PMC 4650908. PMID 26575137.
- 1 2 3 4 5 McIntosh, SE; Opacic, M; Freer, L; Grissom, CK; Auerbach, PS; Rodway, GW; Cochran, A; Giesbrecht, GG; McDevitt, M; Imray, CH; Johnson, EL; Dow, J; Hackett, PH; Wilderness Medical, Society. (December 2014). "Wilderness Medical Society practice guidelines for the prevention and treatment of frostbite: 2014 update". Wilderness & Environmental Medicine. 25 (4 Suppl): S43-54. doi:10.1016/j.wem.2014.09.001. PMID 25498262.
- 1 2 "VisualDx - Frostbite". VisualDx. Archived from the original on 2017-03-03. Retrieved 2017-03-03.
- ↑ "Frostbite". us.bestpractice.bmj.com. Archived from the original on 2017-03-04. Retrieved 2017-03-04.
- ↑ Fudge J (2016). "Preventing and Managing Hypothermia and Frostbite Injury". Sports Health. 8 (2): 133–9. doi:10.1177/1941738116630542. PMC 4789935. PMID 26857732.
- ↑ Heil, K; Thomas, R; Robertson, G; Porter, A; Milner, R; Wood, A (March 2016). "Freezing and non-freezing cold weather injuries: a systematic review". British Medical Bulletin. 117 (1): 79–93. doi:10.1093/bmb/ldw001. PMID 26872856.
- ↑ Mistovich, Joseph; Haffen, Brent; Karren, Keith (2004). Prehospital Emergency Care. Upsaddle River, NJ: Pearson Education. p. 506. ISBN 0-13-049288-4.
- 1 2 "Frostbite". www.uptodate.com. Archived from the original on 2017-03-04. Retrieved 2017-03-03.
- ↑ Sachs, C; Lehnhardt, M; Daigeler, A; Goertz, O (30 October 2015). "The Triaging and Treatment of Cold-Induced Injuries". Deutsches Ärzteblatt International. 112 (44): 741–7. doi:10.3238/arztebl.2015.0741. PMC 4650908. PMID 26575137.
- ↑ Golant, A; Nord, RM; Paksima, N; Posner, MA (Dec 2008). "Cold exposure injuries to the extremities". J Am Acad Orthop Surg. 16 (12): 704–15. doi:10.5435/00124635-200812000-00003. PMID 19056919.
- 1 2 Marx 2010, p. 1866
- ↑ "Frostbite: Background, Pathophysiology, Etiology". Medscape. Medscape, LLC. 2017-02-02. Archived from the original on 2017-03-02.
- ↑ "British History in depth: The Race to the South Pole". BBC - History. Archived from the original on 2017-02-13. Retrieved 2017-03-04.
- ↑ "Hugh Herr's Best Foot Forward | Boston Magazine". Boston Magazine. 2009-02-18. Archived from the original on 2017-03-30. Retrieved 2017-03-04.
- ↑ "Beck Weathers Says Fateful Everest Climb Saved His Marriage". PEOPLE. 2015-09-16. Archived from the original on 2017-03-04. Retrieved 2017-03-04.
- ↑ Heawood, Jonathan (2004-03-27). "I'll get there, even if it kills..." The Guardian. ISSN 0261-3077. Archived from the original on 2017-03-04. Retrieved 2017-03-04.
- ↑ Marx 2010
- ↑ Finderle Z, Cankar K (April 2002). "Delayed treatment of frostbite injury with hyperbaric oxygen therapy: a case report". Aviat Space Environ Med. 73 (4): 392–4. PMID 11952063.
- ↑ Folio LR, Arkin K, Butler WP (May 2007). "Frostbite in a mountain climber treated with hyperbaric oxygen: case report". Mil Med. 172 (5): 560–3. doi:10.7205/milmed.172.5.560. PMID 17521112.
- ↑ Gage AA, Ishikawa H, Winter PM (1970). "Experimental frostbite. The effect of hyperbaric oxygenation on tissue survival". Cryobiology. 7 (1): 1–8. doi:10.1016/0011-2240(70)90038-6. PMID 5475096.
- ↑ Weaver LK, Greenway L, Elliot CG (1988). "Controlled Frostbite Injury to Mice: Outcome of Hyperbaric Oxygen Therapy". J. Hyperbaric Med. 3 (1): 35–44. Archived from the original on 10 July 2009. Retrieved 20 June 2008.
- ↑ Ay H, Uzun G, Yildiz S, Solmazgul E, Dundar K, Qyrdedi T, Yildirim I, Gumus T (2005). "The treatment of deep frostbite of both feet in two patients with hyperbaric oxygen". Undersea Hyperb. Med. 32 (1 Suppl). ISSN 1066-2936. OCLC 26915585. Archived from the original on 15 September 2008. Retrieved 30 June 2008.
- ↑ Bruen, KJ; Ballard JR; Morris SE; Cochran A; Edelman LS; Saffle JR (2007). "Reduction of the incidence of amputation in frostbite injury with thrombolytic therapy". Archives of Surgery. 142 (6): 546–51. doi:10.1001/archsurg.142.6.546. PMID 17576891.
External links
| Classification | |
|---|---|
| External resources |
- Yukon frostbite protocol Archived 2021-09-13 at the Wayback Machine