Vasculitis
| Vasculitis | |
|---|---|
| Other names: Vasculitides,[1] angiitis[2] | |
 | |
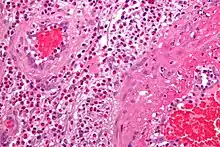
| Smaller and larger areas of bleeding into the skin on the lower limb due to medication-induced vasculitis. | |
| Pronunciation |
|
| Specialty | Rheumatology |
| Symptoms | Fever, weight loss, tiredness, bleeding, tender blood vessels[3][4] |
| Complications | Stroke, heart attacks, aortic dissection, kidney failure, coughing up blood[3] |
| Usual onset | Variable[4] |
| Types | Large: Giant cell arteritis, Takayasu disease, Behcet disease[3][5] Medium: Kawasaki disease, polyarteritis nodosa[3][5] Small: Microscopic polyangiitis, granulomatosis with polyangiitis[3][5] |
| Causes | Often unknown[3] |
| Diagnostic method | Blood tests, medical imaging, biopsy[5] |
| Differential diagnosis | Infective endocarditis, histoplasmosis, gonorrhea, thrombotic thrombocytopenic purpura |
| Treatment | Depends on the type, often initially with steroids[3] |
Vasculitis is a group of disorders that involves inflammation of blood vessels.[3][6] Symptoms may include fever, weight loss, tiredness, bleeding, and tender blood vessels.[3][4] Further symptoms may vary depending on the location and type of vessel affected.[3] Complications may include stroke, heart attacks, aortic dissection, kidney failure, and coughing up blood.[3]
There are more than 30 types of vasculitis, which may involve arteries, veins, or capillaries.[3][5] Types that involve large vessels include giant cell arteritis (GCA), Takayasu disease, and Behcet disease; types that involve medium vessels include Kawasaki disease and polyarteritis nodosa (PAN); and types that involve small vessels include microscopic polyangiitis and granulomatosis with polyangiitis (GPA).[3][5] There; however, may be overlap between these groups.[5]
The cause is often unknown, though certain cases may be triggered by an infection, medication, or other disorder.[3][5] Risk factors depend on the condition in question.[3] The underlying mechanism is often that of an autoimmune disease with neutrophils entering the inner lining of the vessel.[6][4] The diagnosis may be suspected based on blood tests, such as ESR or CRP, medical imaging, and biopsy.[3][5]
Treatment depends on the type, though steroids are often used initially.[3] About 3 per 100,000 people are newly affected by a systemic vasculitis per year in Europe and the United States.[3] In those over the age of 50 GCA newly affects about 24 per 100,000 per year.[3] Different types of disease are more common within certain age groups.[4] Overall males and females are affected with similar frequency.[2] While the condition has been described since at least the 11th century the first detailed description is attributed to Kussmaul and Maier in 1866.[7]
Signs and symptoms
Possible symptoms include:[8]
- General symptoms: Fever, unintentional weight loss
- Skin: Palpable purpura, livedo reticularis
- Muscles and joints: Muscle pain or inflammation, joint pain or joint swelling
- Nervous system: Mononeuritis multiplex, headache, stroke, tinnitus, reduced visual acuity, acute visual loss
- Heart and arteries: Heart attack, high blood pressure, gangrene
- Respiratory tract: Nose bleeds, bloody cough, lung infiltrates
- GI tract: Abdominal pain, bloody stool, perforations (hole in the GI tract)
- Kidneys: Inflammation of the kidney's filtration units (glomeruli)
Cause
Classification
Vasculitis can be classified by the cause, the location, the type of vessel or the size of vessel.
- Underlying cause. For example, the cause of syphilitic aortitis is infectious (aortitis simply refers to inflammation of the aorta, which is an artery.) However, the causes of many forms of vasculitis are poorly understood. There is usually an immune component, but the trigger is often not identified. In these cases, the antibody found is sometimes used in classification, as in ANCA-associated vasculitides.
- Location of the affected vessels. For example, ICD-10 classifies "vasculitis limited to skin" with skin conditions (under "L"), and "necrotizing vasculopathies" (corresponding to systemic vasculitis) with musculoskeletal system and connective tissue conditions (under "M"). Arteritis/phlebitis on their own are classified with circulatory conditions (under "I").
- Type or size of the blood vessels that they predominantly affect.[9] Apart from the arteritis/phlebitis distinction mentioned above, vasculitis is often classified by the caliber of the vessel affected. However, there can be some variation in the size of the vessels affected.
A small number have been shown to have a genetic basis. These include adenosine deaminase 2 deficiency and haploinsufficiency of A20.
According to the size of the vessel affected, vasculitis can be classified into:[10][11]
- Large vessel: Takayasu's arteritis, Temporal arteritis
- Medium vessel: Buerger's disease, Kawasaki disease, Polyarteritis nodosa
- Small vessel: Behçet's syndrome, Eosinophilic granulomatosis with polyangiitis, Cutaneous vasculitis, granulomatosis with polyangiitis, Henoch–Schönlein purpura, and microscopic polyangiitis. Condition of some disorders have vasculitis as their main feature. The major types are given in the table below:
| Major types | ||
|---|---|---|
| Vasculitis | Affected organs | Histopathology |
| Cutaneous small-vessel vasculitis | Skin, kidneys | Neutrophils, fibrinoid necrosis |
| Granulomatosis with polyangiitis | Nose, lungs, kidneys | Neutrophils, giant cells |
| Eosinophilic granulomatosis with polyangiitis | Lungs, kidneys, heart, skin | Histiocytes, eosinophils |
| Behçet's disease | Commonly sinuses, brain, eyes and skin; can affect other organs such as lungs, kidneys, joints | Lymphocytes, macrophages, neutrophils |
| Kawasaki disease | Skin, heart, mouth, eyes | Lymphocytes, endothelial necrosis |
| Buerger's disease | Leg arteries and veins (gangrene) | Neutrophils, granulomas |
| "Limited" granulomatosis with polyangiitis vasculitis | Commonly sinuses, brain, and skin; can affect other organs such as lungs, kidneys, joints; | |
Takayasu's arteritis, polyarteritis nodosa and giant cell arteritis mainly involve arteries and are thus sometimes classed specifically under arteritis.
Furthermore, there are many conditions that have vasculitis as an accompanying or atypical feature, including:
- Rheumatic diseases, such as rheumatoid arthritis, systemic lupus erythematosus, and dermatomyositis
- Cancer, such as lymphomas
- Infections, such as hepatitis C
- Exposure to chemicals and drugs, such as amphetamines, cocaine, and anthrax vaccines which contain the Anthrax Protective Antigen as the primary ingredient.
In pediatric patients varicella inflammation may be followed by vasculitis of intracranial vessels. This condition is called post varicella angiopathy and this may be responsible for arterial ischaemic strokes in children.[12]
Several of these vasculitides are associated with antineutrophil cytoplasmic antibodies.[13] These are:
- Granulomatosis with polyangiitis
- Eosinophilic granulomatosis with polyangiitis
- Microscopic polyangiitis
Diagnosis

- Laboratory tests of blood or body fluids are performed for patients with active vasculitis. Their results will generally show signs of inflammation in the body, such as increased erythrocyte sedimentation rate (ESR), elevated C-reactive protein (CRP), anemia, increased white blood cell count and eosinophilia. Other possible findings are elevated antineutrophil cytoplasmic antibody (ANCA) levels and hematuria.
- Other organ functional tests may be abnormal. Specific abnormalities depend on the degree of various organs involvement. A Brain SPECT can show decreased blood flow to the brain and brain damage.
- The definite diagnosis of vasculitis is established after a biopsy of involved organ or tissue, such as skin, sinuses, lung, nerve, brain, and kidney. The biopsy elucidates the pattern of blood vessel inflammation.
- Some types of vasculitis display leukocytoclasis, which is vascular damage caused by nuclear debris from infiltrating neutrophils.[14] It typically presents as palpable purpura.[14] Conditions with leucocytoclasis mainly include hypersensitivity vasculitis (also called leukocytoclastic vasculitis) and cutaneous small-vessel vasculitis (also called cutaneous leukocytoclastic angiitis).
- An alternative to biopsy can be an angiogram (x-ray test of the blood vessels). It can demonstrate characteristic patterns of inflammation in affected blood vessels.
- 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT)has become a widely used imaging tool in patients with suspected Large Vessel Vasculitis, due to the enhanced glucose metabolism of inflamed vessel walls.[15] The combined evaluation of the intensity and the extension of FDG vessel uptake at diagnosis can predict the clinical course of the disease, separating patients with favourable or complicated progress.[16]
- Acute onset of vasculitis-like symptoms in small children or babies may instead be the life-threatening purpura fulminans, usually associated with severe infection.
| Disease | Serologic test | Antigen | Associated laboratory features |
|---|---|---|---|
| Systemic lupus erythematosus | ANA including antibodies to dsDNA and ENA [including SM, Ro (SSA), La (SSB), and RNP] | Nuclear antigens | Leukopenia, thrombocytopenia, Coombs' test, complement activation: low serum concentrations of C3 and C4, positive immunofluorescence using Crithidia luciliae as substrate, antiphospholipid antibodies (i.e. anticardiolipin, lupus anticoagulant, false-positive VDRL) |
| Goodpasture's disease | Anti-glomerular basement membrane antibody | Epitope on noncollagen domain of type IV collagen | |
| Small vessel vasculitis | |||
| Microscopic polyangiitis | Perinuclear antineutrophil cytoplasmic antibody | Myeloperoxidase | Elevated CRP |
| Granulomatosis with polyangiiitis | Cytoplasmic antineutrophil cytoplasmic antibody | Proteinase 3 (PR3) | Elevated CRP |
| Eosinophilic granulomatosis with polyangiitis | perinuclear antineutrophil cytoplasmic antibody in some cases | Myeloperoxidase | Elevated CRP and eosinophilia |
| IgA vasculitis (Henoch-Schönlein purpura) | None | ||
| Cryoglobulinemia | Cryoglobulins, rheumatoid factor, complement components, hepatitis C | ||
| Medium vessel vasculitis | |||
| Classical polyarteritis nodosa | None | Elevated CRP and eosinophilia | |
| Kawasaki's Disease | None | Elevated CRP and ESR |
In this table: ANA = Antinuclear antibodies, CRP = C-reactive protein, ESR = Erythrocyte Sedimentation Rate, dsDNA = double-stranded DNA, ENA = extractable nuclear antigens, RNP = ribonucleoproteins; VDRL = Venereal Disease Research Laboratory
Treatment
Treatments are generally directed toward stopping the inflammation and suppressing the immune system. Typically, corticosteroids such as prednisone are used. Additionally, other immune suppression medications, such as cyclophosphamide and others, are considered. In case of an infection, antimicrobial agents including cephalexin may be prescribed. Affected organs (such as the heart or lungs) may require specific medical treatment intended to improve their function during the active phase of the disease.
References
- ↑ "Vasculitis - Definition from the Merriam-Webster Online Dictionary". Archived from the original on 1 July 2016. Retrieved 8 January 2009.
- 1 2 "Vasculitis". NORD (National Organization for Rare Disorders). Archived from the original on 6 February 2021. Retrieved 18 February 2021.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Jatwani, S; Goyal, A (January 2020). "Vasculitis". PMID 31424770.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 3 4 5 "Vasculitis". www.nhlbi.nih.gov. NHLBI, NIH. Archived from the original on 11 February 2021. Retrieved 18 February 2021.
- 1 2 3 4 5 6 7 8 9 "Overview of Vasculitis - Musculoskeletal and Connective Tissue Disorders". Merck Manuals Professional Edition. Archived from the original on 3 April 2015. Retrieved 18 February 2021.
- 1 2 "Glossary of dermatopathological terms. DermNet NZ". Archived from the original on 20 December 2008. Retrieved 8 January 2009.
- ↑ Hendaoui, Lotfi; Stanson, Anthony W.; Bouhaouala, M. Habib; Joffre, Francis (2011). Systemic Vasculitis: Imaging Features. Springer Science & Business Media. p. 8. ISBN 978-3-642-02484-9. Archived from the original on 10 July 2021. Retrieved 18 February 2021.
- ↑ "The Johns Hopkins Vasculitis Center - Symptoms of Vasculitis". Archived from the original on 27 February 2009. Retrieved 7 May 2009.
- ↑ Jennette JC, Falk RJ, Andrassy K, et al. (1994). "Nomenclature of systemic vasculitides. Proposal of an international consensus conference". Arthritis Rheum. 37 (2): 187–92. doi:10.1002/art.1780370206. PMID 8129773.
- ↑ "Overview of Vasculitis". Archived from the original on 3 April 2015. Retrieved 5 October 2016.
- ↑ Gündüz, Özgür (18 October 2011). "Histopathological Evaluation of Behçet's Disease and Identification of New Skin Lesions". Pathology Research International. 2012: 1–7. doi:10.1155/2012/209316. ISSN 2090-8091. PMC 3199096. PMID 22028988.
- ↑ Nita R Sutay, Md Ashfaque Tinmaswala, Shilpa Hegde . "International Journal of Medical Research and Health Sciences | 404 Page". Archived from the original on 17 November 2015. Retrieved 19 August 2015.
- ↑ Millet A, Pederzoli-Ribeil M, Guillevin L, Witko-Sarsat V, Mouthon L (2013) Antineutrophil cytoplasmic antibody-associated vasculitides: is it time to split up the group? Ann Rheum Dis
- 1 2 A Brooke W Eastham, Ruth Ann Vleugels and Jeffrey P Callen. "Leukocytoclastic Vasculitis". Medscape. Archived from the original on 19 October 2019. Retrieved 8 November 2019. Updated: Oct 25, 2018
- ↑ Maffioli L, Mazzone A (2014). "Giant-Cell Arteritis and Polymyalgia Rheumatica". NEJM. 371 (17): 1652–1653. doi:10.1056/NEJMc1409206. PMC 4277693. PMID 25337761.
- ↑ Dellavedova L, Carletto M, Faggioli P, Sciascera A, Del Sole A, Mazzone A, Maffioli LS (2015). "The prognostic value of baseline 18F-FDG PET/CT in steroid-naïve large-vessel vasculitis: introduction of volume-based parameters". European Journal of Nuclear Medicine and Molecular Imaging. 55 (2): 340–8. doi:10.1007/s00259-015-3148-9. PMID 26250689.
- ↑ Burtis CA, Ashwood ER, Bruns DE (2012). Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 5th edition. Elsevier Saunders. p. 1568. ISBN 978-1-4160-6164-9.
External links
| Classification |
|---|