Pattern hair loss
| Pattern hair loss | |
|---|---|
| Other names: Androgenic alopecia, androgenetic alopecia, male pattern baldness, female androgenic alopecia, female pattern baldness[1] | |
 | |
| Male-pattern hair loss shown on the vertex of the scalp | |
| Specialty | Dermatology, plastic surgery |
| Usual onset | After puberty[2] |
| Risk factors | Family history[2] |
| Diagnostic method | Based on symptoms and examination[2] |
| Differential diagnosis | Alopecia areata, anagen effluvium, telogen effluvium, syphilis[2] |
| Treatment | Acceptance, medications, hair transplant surgery[3] |
| Medication | Minoxidil, finasteride, dutasteride, spironolactone[3][2] |
| Prognosis | Not serious[2] |
| Frequency | By age 50: half (males), 25% (females)[3] |
Pattern hair loss, also known as androgenetic alopecia, is a type of hair loss that is gradual in onset and occurs in a characteristic pattern.[2] Onset is after puberty.[2] In males the top and front of the scalp is initially involved.[2] In females it typically presents as thinning of the hair.[3] While it is associated with heart disease and prostate cancer, the condition itself is not serious.[2]
Male pattern hair loss is believed to be due to a combination of genetics and the male hormone dihydrotestosterone.[3] The cause in female pattern hair loss remains unclear.[3] A son, of an affected father, has a five fold increased risk of the condition.[2] Multiple genes are involved.[2] In women the condition is often first noticed one to six months after a significant stressor.[2]
Management may include simply accepting the condition.[3] Otherwise, treatments may include minoxidil, finasteride, dutasteride, or hair transplant surgery.[3] These medications can take six months for an effect.[2] In women spironolactone may also be used.[2] Use of finasteride and dutasteride in women is not well-studied, and it may result in birth defects if taken during pregnancy.[3]
Pattern hair loss by the age of 50 affects about half of males and a quarter of females.[3] Up to 80% of males over the age of 70 may be affected.[2] The condition becomes more common after menopause.[2] White people are more commonly affected than people of color.[2]
Signs and symptoms
Classic male-pattern hair loss begins above the temples and vertex (calvaria) of the scalp. As it progresses, a rim of hair at the sides and rear of the head remains. This has been referred to as a 'Hippocratic wreath', and rarely progresses to complete baldness.[4] Pattern hair loss is classified as a form of non-scarring hair loss.
Female-pattern hair loss more often causes diffuse thinning without hairline recession; similar to its male counterpart, female androgenic alopecia rarely leads to total hair loss.[5] The Ludwig scale grades severity of female-pattern hair loss. These include Grades 1, 2, 3 of balding in women based on their scalp showing in the front due to thinning of hair.
.jpg.webp) Grade 2 hair loss
Grade 2 hair loss.jpg.webp) Grade 3 hair loss
Grade 3 hair loss.jpg.webp) Grade 4 hair loss
Grade 4 hair loss
Psychological
Androgenic alopecia is typically experienced as a "moderately stressful condition that diminishes body image satisfaction".[6] However, although most men regard baldness as an unwanted and distressing experience, they usually are able to cope and retain integrity of personality.[7]
Although baldness is not as common in women as in men, the psychological effects of hair loss tend to be much greater. Typically, the frontal hairline is preserved, but the density of hair is decreased on all areas of the scalp. Previously, it was believed to be caused by testosterone just as in male baldness, but most women who lose hair have normal testosterone levels.[8]
Causes
KRT37 is the only keratin that is regulated by androgens.[9] This sensitivity to androgens was acquired by Homo sapiens and is not shared with their great ape cousins. Although Winter et al. found that KRT37 is expressed in all the hair follices of chimpanzees, it was not detected in the head hair of modern humans. As androgens are known to grow hair on the body but decrease it on the scalp, this lack of scalp KRT37 may help explain the paradoxical nature of Androgenic alopecia as well as the fact that head hair anagen cycles are extremely long.
Research indicates that the initial programming of pilosebaceous units of hair follicles begins in utero.[10] The physiology is primarily androgenic, with dihydrotestosterone (DHT) being the major contributor at the dermal papillae. Men with premature androgenic alopecia tend to have lower than normal values of sex hormone-binding globulin (SHBG), follicle stimulating hormone (FSH), testosterone, and epitestosterone when compared to men without pattern hair loss.[11] Although hair follicles were previously thought to be permanently gone in areas of complete hair loss, they are more likely dormant, as recent studies have shown the scalp contains the stem cell progenitor cells from which the follicles arose.[12]
Transgenic studies have shown that growth and dormancy of hair follicles are related to the activity of insulin-like growth factor (IGF) at the dermal papillae, which is affected by DHT. Androgens are important in male sexual development around birth and at puberty. They regulate sebaceous glands, apocrine hair growth, and libido. With increasing age, androgens stimulate hair growth on the face, but can suppress it at the temples and scalp vertex, a condition that has been referred to as the 'androgen paradox'.[13]
Men with androgenic alopecia typically have higher 5α-reductase, higher total testosterone, higher unbound/free testosterone, and higher free androgens, including DHT.[14] 5-alpha-reductase converts free testosterone into DHT, and is highest in the scalp and prostate gland. DHT is most commonly formed at the tissue level by 5α-reduction of testosterone.[15] The genetic corollary that codes for this enzyme has been discovered.[16] Prolactin has also been suggested to have different effects on the hair follicle across gender.[17]
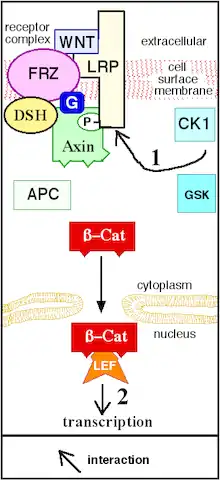
Also, crosstalk occurs between androgens and the Wnt-beta-catenin signaling pathway that leads to hair loss. At the level of the somatic stem cell, androgens promote differentiation of facial hair dermal papillae, but inhibit it at the scalp.[13] Other research suggests the enzyme prostaglandin D2 synthase and its product prostaglandin D2 (PGD2) in hair follicles as contributive.[18]
These observations have led to study at the level of the mesenchymal dermal papillae.[19] Types 1 and 2 5α reductase enzymes are present at pilosebaceous units in papillae of individual hair follicles.[20] They catalyze formation of the androgens testosterone and DHT, which in turn regulate hair growth.[13] Androgens have different effects at different follicles: they stimulate IGF-1 at facial hair, leading to growth, but can also stimulate TGF β1, TGF β2, dickkopf1, and IL-6 at the scalp, leading to catagenic miniaturization.[13] Hair follicles in anaphase express four different caspases. Significant levels of inflammatory infiltrate have been found in transitional hair follicles.[21] Interleukin 1 is suspected to be a cytokine mediator that promotes hair loss.[22]
The fact that hair loss is cumulative with age while androgen levels fall as well as the fact that finasteride does not reverse advanced stages of androgenetic alopecia remains a mystery but some possible explanations have been put forward: Higher conversion of testosterone to DHT locally with age as higher levels of 5-alpha reductase are noted in balding scalp, and higher levels of DNA damage in the dermal papilla as well as senescence of the dermal papilla due to androgen receptor activation and environmental stress.[23] The mechanism by which the androgen receptor triggers dermal papilla permanent senescence is not known but may involve IL6, TGFB-1 and oxidative stress. Senescence of the dermal papilla is measured by lack of mobility, different size and shape, lower replication and altered output of molecules and different expression of markers. The dermal papilla is the primary location of androgen action and its migration towards the hair bulge and subsequent signaling and size increase are required to maintain the hair follicle so senescence via the androgen receptor explains much of the physiology.
Diagnosis
The diagnosis of androgenic alopecia can be usually established based on clinical presentation in men. In women, the diagnosis usually requires more complex diagnostic evaluation. Further evaluation of the differential requires exclusion of other causes of hair loss, and assessing for the typical progressive hair loss pattern of androgenic alopecia.[24] Trichoscopy can be used for further evaluation.[25] Biopsy may be needed to exclude other causes of hair loss,[26] and histology would demonstrate perifollicular fibrosis.[27][28] The Hamilton–Norwood scale has been developed to grade androgenic alopecia in males by severity.
Treatment
Medications
Androgen-dependent
Finasteride is a medication of the 5α-reductase inhibitors (5-ARIs) class.[29] By inhibiting type II 5-AR, finasteride prevents the conversion of testosterone to dihydrotestosterone in various tissues including the scalp.[29][30] Increased hair on the scalp can be seen within three months of starting finasteride treatment and longer-term studies have demonstrated increased hair on the scalp at 24 and 48 months with continued use.[30] Treatment with finasteride more effectively treats male-pattern hair loss at the vertex than male-pattern hair loss at the front of the head and temples.[30]
Dutasteride is a medication in the same class as finasteride but inhibits both type I and type II 5-alpha reductase.[30] Dutasteride is approved for the treatment of male-pattern hair loss in Korea and Japan, but not in the United States.[30] However, it is commonly used off-label to treat male-pattern hair loss.[30]
Androgen-independent
Minoxidil dilates small blood vessels; it is not clear how this causes hair to grow.[31] Other treatments include tretinoin combined with minoxidil, ketoconazole shampoo, dermarolling (Collagen induction therapy) spironolactone,[32] alfatradiol, and topilutamide (fluridil).[33]
There is evidence supporting the use of minoxidil as a safe and effective treatment for female pattern hair loss, and there is no significant difference in efficacy between 2% and 5% formulations.[34] Finasteride was shown to be no more effective than placebo based on low-quality studies.[34] The effectiveness of laser-based therapies is unclear.[34]
Procedures
More advanced cases may be resistant or unresponsive to medical therapy and require hair transplantation. Naturally occurring units of one to four hairs, called follicular units, are excised and moved to areas of hair restoration.[32] These follicular units are surgically implanted in the scalp in close proximity and in large numbers. The grafts are obtained from either follicular unit transplantation (FUT) or follicular unit extraction (FUE). In the former, a strip of skin with follicular units is extracted and dissected into individual follicular unit grafts, and in the latter individual hairs are extracted manually or robotically. The surgeon then implants the grafts into small incisions, called recipient sites.[35][36] Cosmetic scalp tattoos can also mimic the appearance of a short, buzzed haircut.
Alternative therapies
Many people use unproven treatments.[37] Regarding female pattern alopecia, there is no evidence for vitamins, minerals, or other dietary supplements.[38] As of 2008, there is little evidence to support the use of lasers to treat male-pattern hair loss.[39] The same applies to special lights.[38] Dietary supplements are not typically recommended.[39] A 2015 review found a growing number of papers in which plant extracts were studied but only one randomized controlled clinical trial, namely a study in 10 people of saw palmetto extract.[40][41]
Epidemiology
Female androgenic alopecia has become a growing problem that, according to the American Academy of Dermatology, affects around 30 million women in the United States. Although hair loss in females normally occurs after the age of 50 or even later when it does not follow events like pregnancy, chronic illness, crash diets, and stress among others, it is now occurring at earlier ages with reported cases in women as young as 15 or 16.[42]
Society and culture
Studies have been inconsistent across cultures regarding how balding men rate on the attraction scale. While a 2001 South Korean study showed that most people rated balding men as less attractive,[43] a 2002 survey of Welsh women found that they rated bald and gray-haired men quite desirable.[44] One of the proposed social theories for male pattern hair loss is that men who embraced complete baldness by shaving their heads subsequently signaled dominance, high social status, and/or longevity.[45]
Myths

Greek philosophers with and without much hair (from left to right: Socrates, Antisthenes, Chrysippus, and Epicurus, fifth to third centuries BC)
Many myths exist regarding the possible causes of baldness and its relationship with one's virility, intelligence, ethnicity, job, social class, wealth, and many other characteristics.
Physical activity
Because it increases testosterone levels, many Internet forums have put forward the idea that weight training and other forms of exercise increase hair loss in predisposed individuals. Although scientific studies do support a correlation between exercise and testosterone, no direct study has found a link between exercise and baldness. However, a few have found a relationship between a sedentary life and baldness, suggesting some exercise is beneficial. The type or quantity of exercise may influence hair loss.[46][47] Testosterone levels are not a good marker of baldness, and many studies actually show paradoxical low testosterone in balding persons, although research on the implications is limited.
Emotional stress
Emotional stress has been shown to accelerate baldness in genetically susceptible individuals.[48] Stress due to sleep deprivation in military recruits lowered testosterone levels, but is not noted to have affected SHBG.[49] Thus, stress due to sleep deprivation in fit males is unlikely to elevate DHT, which is one cause of male pattern baldness. Whether sleep deprivation can cause hair loss by some other mechanism is not clear.
Sexually activity
Levels of free testosterone are strongly linked to libido and DHT levels, but unless free testosterone is virtually nonexistent, levels have not been shown to affect virility. Men with androgenic alopecia are more likely to have a higher baseline of free androgens. However, sexual activity is multifactoral, and androgenic profile is not the only determining factor in baldness. Additionally, because hair loss is progressive and free testosterone declines with age, a male's hairline may be more indicative of his past than his present disposition.[50][51]
Many misconceptions exist about what can help prevent hair loss, one of these being that lack of sex will prevent hair loss. While a correlation exists between increased frequency of ejaculation and increased levels of DHT, the study suggests that ejaculation frequency may be a sign, rather than a cause, of higher DHT levels.[52] Another study shows that although sexual arousal and masturbation-induced orgasm increase testosterone concentration around orgasm, they reduce testosterone concentration on average, and because about 5% of testosterone is converted to DHT, ejaculation does not elevate DHT levels.[53]
The only published study to test correlation between ejaculation frequency and baldness was probably large enough to detect an association (1390 subjects) and found no correlation, although persons with only vertex androgenetic alopecia had fewer female sexual partners than those of other androgenetic alopecia categories (such as frontal or both frontal and vertex). One study may not be enough, especially in baldness, where there is a complex with age.[54]
Names
Male pattern hair loss is also known as androgenic alopecia, androgenetic alopecia (AGA), alopecia androgenetica, and male pattern baldness (MPB).
Other animals
Animal models of androgenic alopecia occur naturally and have been developed in transgenic mice;[55] chimpanzees (Pan troglodytes); bald uakaris (Cacajao rubicundus); and stump-tailed macaques (Macaca speciosa and M. arctoides). Of these, macaques have demonstrated the greatest incidence and most prominent degrees of hair loss.[56][57]
Baldness is not a trait unique to human beings. One possible case study is about a maneless male lion in the Tsavo area. The Tsavo lion prides are unique in that they frequently have only a single male lion with usually seven or eight adult females, as opposed to four females in other lion prides. Male lions may have heightened levels of testosterone, which could explain their reputation for aggression and dominance, indicating that lack of mane may at one time have had an alpha correlation.[58]
Although primates do not go bald, their hairlines do undergo recession. In infancy the hairline starts at the top of the supraorbital ridge, but slowly recedes after puberty to create the appearance of a small forehead.
References
- ↑ "Androgenetic alopecia: MedlinePlus Genetics". medlineplus.gov. Archived from the original on 9 November 2020. Retrieved 6 November 2020.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Ho, Chin H.; Sood, Tanuj; Zito, Patrick M. (2020). "Androgenetic Alopecia". StatPearls. StatPearls Publishing. PMID 28613674. Archived from the original on 2021-08-28. Retrieved 2020-11-06.
- 1 2 3 4 5 6 7 8 9 10 Vary JC, Jr (November 2015). "Selected Disorders of Skin Appendages--Acne, Alopecia, Hyperhidrosis". The Medical Clinics of North America (Review). 99 (6): 1195–1211. doi:10.1016/j.mcna.2015.07.003. PMID 26476248.
- ↑ "Hippocratic wreath (Baldness)". Britannica Online. Dec 15, 2012. Archived from the original on June 19, 2013. Retrieved Dec 15, 2012.
- ↑ "Female pattern baldness". MedlinePlus. Dec 15, 2012. Archived from the original on December 1, 2012. Retrieved Dec 15, 2012.
- ↑ Cash, T. F. (1999). "The psychosocial consequences of androgenetic alopecia: A review of the research literature". The British Journal of Dermatology. 141 (3): 398–405. doi:10.1046/j.1365-2133.1999.03030.x. PMID 10583042.
- ↑ Cash, T. F. (1992). "The psychological effects of androgenetic alopecia in men". Journal of the American Academy of Dermatology. 26 (6): 926–931. doi:10.1016/0190-9622(92)70134-2. PMID 1607410.
- ↑ Birch, M. P.; Lalla, S. C.; Messenger, A. G. (2002). "Female pattern hair loss". Clinical and Experimental Dermatology. 27 (5): 383–388. doi:10.1046/j.1365-2230.2002.01085.x. PMID 12190638.
- ↑ Jave-Suarez LF, Langbein L, Winter H, Praetzel S, Rogers MA, Schweizer J (March 2004). "Androgen regulation of the human hair follicle: the type I hair keratin hHa7 is a direct target gene in trichocytes". The Journal of Investigative Dermatology. 122 (3): 555–564. doi:10.1111/j.0022-202X.2004.22336.x. PMID 15086535.
- ↑ Alonso, L. C.; Rosenfield, R. L. (2003). "Molecular genetic and endocrine mechanisms of hair growth". Hormone Research. 60 (1): 1–13. doi:10.1159/000070821. PMID 12792148. Archived from the original on 2021-08-28. Retrieved 2020-01-31.
- ↑ Starka, L.; Duskova, I.; Cermakova, I.; Vrbiková, J. & Hill, M. (April 6, 2006). "Premature androgenic alopecia and insulin resistance. Male equivalent of polycystic ovary syndrome?" (pdf). Endocrine Regulations. Slovak Academic Press. 39 (4): 127–131. PMID 16552990. Archived from the original on March 7, 2019. Retrieved Mar 7, 2019.
- ↑ Garza, LA; Yang, CC; Zhao, T; Blatt, HB; Lee, M; He, H; Stanton, DC; Carrasco, L; Spiegel, JH; Tobias, JW; Cotsarelis, G (February 2011). "Bald scalp in men with androgenetic alopecia retains hair follicle stem cells but lacks CD200-rich and CD34-positive hair follicle progenitor cells". The Journal of Clinical Investigation. 121 (2): 613–622. doi:10.1172/JCI44478. PMC 3026732. PMID 21206086.
- 1 2 3 4 Inui, S.; Itami, S. (2012). "Androgen actions on the human hair follicle: Perspectives". Experimental Dermatology. 22 (3): 168–171. doi:10.1111/exd.12024. PMID 23016593.
- ↑ Y., Zhang; J., Xu (2018). "Serum Levels of Androgen-Associated Hormones Are Correlated with Curative Effect in Androgenic Alopecia in Young Men". Medical Science Monitor. 24: 7770–7777. doi:10.12659/MSM.913116. PMC 6223099. PMID 30376555.
- ↑ Kaufman, J. M.; Vermeulen, A. (2005). "The Decline of Androgen Levels in Elderly Men and Its Clinical and Therapeutic Implications". Endocrine Reviews. 26 (6): 833–876. doi:10.1210/er.2004-0013. PMID 15901667.
- ↑ Ellis, J. A.; Panagiotopoulos, S.; Akdeniz, A.; Jerums, G.; Harrap, S. B. (2005). "Androgenic correlates of genetic variation in the gene encoding 5α-reductase type 1". Journal of Human Genetics. 50 (10): 534–537. doi:10.1007/s10038-005-0289-x. PMID 16155734.
- ↑ Langan, E. A.; Ramot, Y.; Goffin, V.; Griffiths, C. E. M.; Foitzik, K.; Paus, R. (2009). "Mind the (Gender) Gap: Does Prolactin Exert Gender and/or Site-Specific Effects on the Human Hair Follicle?". Journal of Investigative Dermatology. 130 (3): 886–891. doi:10.1038/jid.2009.340. PMID 19890346.
- ↑ Garza, L. A.; Liu, Y.; Yang, Z.; Alagesan, B.; Lawson, J. A.; Norberg, S. M.; Loy, D. E.; Zhao, T.; Blatt, H. B.; Stanton, D. C.; Carrasco, L.; Ahluwalia, G.; Fischer, S. M.; Fitzgerald, G. A.; Cotsarelis, G. (2012). "Prostaglandin D2 Inhibits Hair Growth and is Elevated in Bald Scalp of Men with Androgenetic Alopecia". Science Translational Medicine. 4 (126): 126ra34. doi:10.1126/scitranslmed.3003122. PMC 3319975. PMID 22440736.
- ↑ Randall, V. A.; Hibberts, N. A.; Thornton, M. J.; Merrick, A. E.; Hamada, K.; Kato, S.; Jenner, T. J.; De Oliveira, I.; Messenger, A. G. (2001). "Do androgens influence hair growth by altering the paracrine factors secreted by dermal papilla cells?". European Journal of Dermatology. 11 (4): 315–320. PMID 11399537.
- ↑ Bernard, B. A. (1994). "Molecular approach of hair biology". Comptes Rendus des Séances de la Société de Biologie et de Ses Filiales. 188 (3): 223–233. PMID 7834505.
- ↑ Jaworsky, C.; Kligman, AM.; Murphy, GF. (1992). "Characterization of inflammatory infiltrates in male pattern alopecia: Implications for pathogenesis". Br J Dermatol. 127 (3): 239–246. doi:10.1111/j.1365-2133.1992.tb00121.x. PMID 1390168.
- ↑ Hoffmann, R.; Happle, R. (1995). "Does interleukin-1 induce hair loss?". Dermatology. 191 (4): 273–275. doi:10.1159/000246567. PMID 8573920.
- ↑ Kang, Hong- Yo (March 15, 2013). "Androgen Receptor Accelerates Premature Senescence of Human Dermal Papilla Cells in Association with DNA Damage". PLOS ONE. 8 (11): e79434. Bibcode:2013PLoSO...879434Y. doi:10.1371/journal.pone.0079434. PMC 3828374. PMID 24244503.
- ↑ Diagnosing Men's Hair Loss: Norwood Scale Chart Archived 2009-04-09 at the Wayback Machine. Webmd.com (2010-03-01). Retrieved on 2010-11-28.
- ↑ Rudnicka, L.; Olszewska, M.; Rakowska, A.; Kowalska-Oledzka, E.; Slowinska, M. (2008). "Trichoscopy: A new method for diagnosing hair loss". Journal of Drugs in Dermatology. 7 (7): 651–654. PMID 18664157.
- ↑ Mounsey, A. L.; Reed, S. W. (2009). "Diagnosing and treating hair loss". American Family Physician. 80 (4): 356–362. PMID 19678603.
- ↑ Yoo, H. G.; Kim, J. S.; Lee, S. R.; Pyo, H. K.; Moon, H. I.; Lee, J. H.; Kwon, O. S.; Chung, J. H.; Kim, K. H.; Eun, H. C.; Cho, K. H. (2006). "Perifollicular fibrosis: Pathogenetic role in androgenetic alopecia". Biological & Pharmaceutical Bulletin. 29 (6): 1246–1250. doi:10.1248/bpb.29.1246. PMID 16755026.
- ↑ Rashid, R. M.; Thomas, V. (2010). "Androgenic pattern presentation of scarring and inflammatory alopecia". Journal of the European Academy of Dermatology and Venereology. 24 (8): 979–980. doi:10.1111/j.1468-3083.2009.03557.x. PMID 20059630.
- 1 2 Supenya, Varothai (2014). "Bergfeld". Wilma F. 15 (3): 217–230. doi:10.1007/s40257-014-0077-5. PMID 24848508. Archived from the original on 2021-08-28. Retrieved 2020-01-31.
- 1 2 3 4 5 6 Yim, Elizabeth; Nole, Katherine L. Baquerizo; Tosti, Antonella (December 2014). "5α-Reductase inhibitors in androgenetic alopecia". Current Opinion in Endocrinology, Diabetes and Obesity (Review). 21 (6): 493–498. doi:10.1097/MED.0000000000000112. PMID 25268732.
- ↑ "Minoxidil solution". DermNet NZ. Dec 29, 2013. Archived from the original on February 2, 2014. Retrieved Jan 29, 2014.
- 1 2 Rogers, N. E.; Avram, M. R. (2008). "Medical treatments for male and female pattern hair loss". Journal of the American Academy of Dermatology. 59 (4): 547–566, quiz 566–8. doi:10.1016/j.jaad.2008.07.001. PMID 18793935.
- ↑ Varothai, Supenya; Bergfeld, Wilma F. (2014). "Androgenetic Alopecia: An Evidence-Based Treatment Update". American Journal of Clinical Dermatology. 15 (3): 217–230. doi:10.1007/s40257-014-0077-5. ISSN 1175-0561. PMID 24848508. Archived from the original on 2021-08-28. Retrieved 2020-01-31.
- 1 2 3 van Zuuren, Esther J; Fedorowicz, Zbys; Schoones, Jan (2016-05-26). "Interventions for female pattern hair loss". Cochrane Database of Systematic Reviews (5): CD007628. doi:10.1002/14651858.CD007628.pub4. ISSN 1465-1858. PMC 6457957. PMID 27225981. Archived from the original on 2018-06-14. Retrieved 2018-06-12.
- ↑ Caroli, S.; Pathomvanich, D.; Amonpattana, K.; Kumar, A. (2011). "Current status of hair restoration surgery". International Surgery. 96 (4): 345–351. doi:10.9738/cc31.1. PMID 22808618.
- ↑ Rose, P. (2011). "The Latest Innovations in Hair Transplantation". Facial Plastic Surgery. 27 (4): 366–377. doi:10.1055/s-0031-1283055. PMID 21792780.
- ↑ Banka, N; Bunagan, MJ; Shapiro, J (January 2013). "Pattern hair loss in men: diagnosis and medical treatment". Dermatologic Clinics. 31 (1): 129–140. doi:10.1016/j.det.2012.08.003. PMID 23159182.
- 1 2 Levy, LL; Emer, JJ (29 August 2013). "Female pattern alopecia: current perspectives". International Journal of Women's Health. 5: 541–556. doi:10.2147/IJWH.S49337. PMC 3769411. PMID 24039457.
- 1 2 Rogers, NE; Avram, MR (October 2008). "Medical treatments for male and female pattern hair loss". Journal of the American Academy of Dermatology. 59 (4): 547–566, quiz 567–8. doi:10.1016/j.jaad.2008.07.001. PMID 18793935.
- ↑ Rondanelli, M; Perna, S (29 June 2016). "A bibliometric study of scientific literature in Scopus on botanicals for treatment of androgenetic alopecia". Journal of Cosmetic Dermatology. 15 (2): 120–130. doi:10.1111/jocd.12198. PMID 26608588.
- ↑ Prager, N; Bickett, K; French, N; Marcovici, G (April 2002). "A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia". Journal of Alternative and Complementary Medicine. 8 (2): 143–152. doi:10.1089/107555302317371433. PMID 12006122. Archived from the original on 2021-08-28. Retrieved 2020-01-28.
- ↑ "Women and Hair Loss: The Causes". Archived from the original on 30 June 2010. Retrieved 2010-06-29.
- ↑ Henss (2001). "Social Perceptions of Male Pattern Baldness. A Review". Dermatology and Psychosomatics. 2 (2): 63–71. doi:10.1159/000049641. Archived from the original on 2021-08-28. Retrieved 2020-01-31.
- ↑ Castle, Sue (2002). "IT LOCKS LIKE GIRLS GO FOR DARKER HAIR; Bald men sexy too says survey". The Free Library. Archived from the original on 2015-05-18. Retrieved 2015-05-14.
- ↑ Dunn, Robb (2012). "Why haven't bald men gone extinct?". New Scientist. 214 (2869): 44–47. Bibcode:2012NewSc.214...44D. doi:10.1016/s0262-4079(12)61567-x. Archived from the original on June 27, 2012. Retrieved Dec 16, 2012.
- ↑ Lotufo, P. A.; Chae, C. U.; Ajani, U. A.; Hennekens, C. H.; Manson, J. E. (2000). "Male Pattern Baldness and Coronary Heart Disease: The Physicians' Health Study". Archives of Internal Medicine. 160 (2): 165–171. doi:10.1001/archinte.160.2.165. PMID 10647754.
- ↑ Gatherwright, J.; Amirlak, B.; Rowe, D.; Liu, M.; Gliniak, C.; Totonchi, A.; Guyuron, B. (2011). "The Relative Contribution of Endogenous and Exogenous Factors to Male Alopecia". Plastic and Reconstructive Surgery. 128: 14. doi:10.1097/01.prs.0000406222.54557.75.
- ↑ Schmidt, J. B. (1994). "Hormonal Basis of Male and Female Androgenic Alopecia: Clinical Relevance". Skin Pharmacology and Physiology. 7 (1–2): 61–66. doi:10.1159/000211275. PMID 8003325.
- ↑ Remes, K.; Kuoppasalmi, K.; Adlercreutz, H. (2008). "Effect of Physical Exercise and Sleep Deprivation on Plasma Androgen Levels: Modifying Effect of Physical Fitness". International Journal of Sports Medicine. 6 (3): 131–135. doi:10.1055/s-2008-1025825. PMID 4040893.
- ↑ Toone, B. K.; Wheeler, M.; Nanjee, M.; Fenwick, P.; Grant, R. (1983). "Sex hormones, sexual activity and plasma anticonvulsant levels in male epileptics". Journal of Neurology, Neurosurgery & Psychiatry. 46 (9): 824–826. doi:10.1136/jnnp.46.9.824. PMC 1027564. PMID 6413659.
- ↑ Davidson, J. M.; Kwan, M.; Greenleaf, W. J. (1982). "Hormonal replacement and sexuality in men". Clinics in Endocrinology and Metabolism. 11 (3): 599–623. doi:10.1016/S0300-595X(82)80003-0. PMID 6814798.
- ↑ Mantzoros, C. S.; Georgiadis, E. I.; Trichopoulos, D. (1995). "Contribution of dihydrotestosterone to male sexual behaviour". BMJ. 310 (6990): 1289–1291. doi:10.1136/bmj.310.6990.1289. PMC 2549675. PMID 7773040.
- ↑ Exton, M. S.; Krüger, T. H. C.; Bursch, N.; Haake, P.; Knapp, W.; Schedlowski, M.; Hartmann, U. (2001). "Endocrine response to masturbation-induced orgasm in healthy men following a 3-week sexual abstinence". World Journal of Urology. 19 (5): 377–382. doi:10.1007/s003450100222. PMID 11760788. Archived from the original on 2021-08-28. Retrieved 2020-01-31.
- ↑ Severi, G.; Sinclair, R.; Hopper, J. L.; English, D. R.; McCredie, M. R. E.; Boyle, P.; Giles, G. G. (2003). "Androgenetic alopecia in men aged 40–69 years: Prevalence and risk factors". British Journal of Dermatology. 149 (6): 1207–1213. doi:10.1111/j.1365-2133.2003.05565.x. PMID 14674898.
- ↑ Crabtree, J. S.; Kilbourne, E. J.; Peano, B. J.; Chippari, S.; Kenney, T.; McNally, C.; Wang, W.; Harris, H. A.; Winneker, R. C.; Nagpal, S.; Thompson, C. C. (2010). "A Mouse Model of Androgenetic Alopecia". Endocrinology. 151 (5): 2373–2380. doi:10.1210/en.2009-1474. PMID 20233794.
- ↑ Sundberg, J. P.; King, L. E.; Bascom, C. (2001). "Animal models for male pattern (androgenetic) alopecia". European Journal of Dermatology. 11 (4): 321–325. PMID 11399538.
- ↑ Sundberg, J. P.; Beamer, W. G.; Uno, H.; Van Neste, D.; King, L. E. (1999). "Androgenetic Alopecia: In Vivo Models". Experimental and Molecular Pathology. 67 (2): 118–130. doi:10.1006/exmp.1999.2276. PMID 10527763.
- ↑ Borzo, Greg (2002). "Unique social system found in famous Tsavo lions". EurekAlert. Archived from the original on 2014-02-22. Retrieved 2013-09-21.
External links
- NLM- Genetics Home Reference Archived 2009-02-03 at the Wayback Machine
- Scow, D. T.; Nolte, R. S.; Shaughnessy, A. F. (1999). "Medical treatments for balding in men". American Family Physician. 59 (8): 2189–2194, 2196. PMID 10221304.
| Classification | |
|---|---|
| External resources |