Cutaneous small-vessel vasculitis
| Cutaneous small-vessel vasculitis | |
|---|---|
| Other names: Hypersensitivity vasculitis, allergic vasculitis | |
 | |
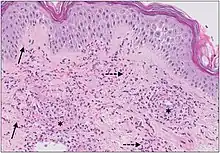
| Example of hypersensitivity vasculitis | |
Cutaneous small-vessel vasculitis (CSVV), also known as hypersensitivity vasculitis, cutaneous leukocytoclastic vasculitis, hypersensitivity angiitis, cutaneous leukocytoclastic angiitis, cutaneous necrotizing vasculitis and cutaneous necrotizing venulitis,[1] is inflammation of small blood vessels (usually post-capillary venules in the dermis), characterized by palpable purpura.[2]: 831 [3] It is the most common vasculitis seen in clinical practice.
"Leukocytoclastic" refers to the damage caused by nuclear debris from infiltrating neutrophils in and around the vessels.[4]
Signs and symptoms
Skin lesions
Initially red to pink, flat spots (formally, "macules") and raised bumps (formally, "papules") may be seen on the skin.[5][6]
Once fully developed, the classic appearance is "non-blanching, palpable purpura".[6][5] [7]This appears as deep red to purple spots that feel raised to the touch. Purpura refers to the red-purple discolored spots, while palpable implies that these spots can be felt as raised from the surrounding skin. Additionally, when gently pressed, the color does not fade to a lighter color ("non-blanching"). The red-purple color of the lesions is due to the inflammation in the blood vessels causing red blood cells to escape into the dermis skin layer.[6]
Small fluid-filled blisters (or "vesicles"), pus-filled bumps resembling a pimple (or "pustules"), or shallow ulcers may also develop but are less common.[6][5]
The location of skin lesions varies but are most commonly found symmetrically below the waist, primarily on the buttocks and legs. Other distributions include localized areas on the upper body or over several areas of the body.[6][5][8]
With treatment, the lesions typically resolve in weeks to months and leave behind flat spots that are darker than the surrounding skin.[5] (see "Postinflammatory hyperpigmentation" on "Hyperpigmentation")
A portion of cases may be persistent or recurrent. This tends to occur when the vasculitis is associated with chronic conditions such as connective tissue diseases.[5][8]
.jpg.webp) Cutaneous vasculitis
Cutaneous vasculitis.jpg.webp) Cutaneous vasculitis
Cutaneous vasculitis.jpg.webp) Small vessel vasculitis
Small vessel vasculitis- Leukocytoclastic vasculitis
 Leukocytoclastic vasculitis
Leukocytoclastic vasculitis Leukocytoclastic vasculitis
Leukocytoclastic vasculitis
Associated symptoms
In most cases skin lesions do not cause symptoms, however itching, burning, or pain may occur.[5]
Frequently reported symptoms include mild fever, muscle pain, joint pain, or an overall feeling of discomfort.[6][8] Additional symptoms depend on the cause of the vasculitis and if other organ systems are involved. For example, if the vasculitis is a manifestation of Henoch-Schönlein purpura, individuals may also experience abdominal pain or blood in the urine.[5]
Cause
Cutaneous vasculitis can have various causes including but not limited to medications, bacterial and viral infections or allergens. It is estimated that 45-55% of cases are idiopathic, meaning the cause is unknown.[5] In cases where a cause can be determined, medications and infectious pathogens are most common in adults, while IgA vasculitis (Henoch-Schönlein purpura) frequently affects children.[6] Other etiologies include autoimmune conditions and malignancies, usually hematologic (related to the blood).[5][6]
| Cause | Frequency | Examples |
|---|---|---|
| Idiopathic | 45-55% | Cause unknown |
| Infection | 15-20% | Staphylococcus and Streptococcus spp. |
| Autoimmune | 15-20% | Rheumatoid arthritis, Systemic lupus erythematosus |
| Medications | 10-15% | Antibiotics, Nonsteroidal anti-inflammatory drugs (NSAIDs) |
The small vessels in the skin affected are located in the superficial dermis and include arterioles (small arteries carrying blood to capillaries), capillaries, and venules (small veins receiving blood from capillaries).[5] In general, immune complexes deposit in vessel walls leading to activation of the complement system. C3a and C5a, proteins produced from the complement system, attract neutrophils to the vessels.[9] Once activated, neutrophils then release preformed substances, including enzymes causing damage to vessel tissue.[9] Evidence of this process can be seen with a sample of removed skin tissue, or biopsy, viewed under a microscope. Neutrophils are seen surrounding blood vessels and their debris within vessel walls, causing fibrinoid necrosis. This finding on histological examination is termed “leukocytoclastic vasculitis”.[5]
Considering the wide range of potential causes leading to cutaneous small vessel vasculitis, there are subtle variations in the underlying pathophysiology for each cause. For example, medications are metabolized to smaller molecules that can attach to proteins in the blood or vessel walls.[10] The immune system senses these altered proteins as foreign and produces antibodies in efforts to eliminate them from the body. A similar process occurs with infectious agents, such as bacteria, in which antibodies target microbial components.[10]
Diagnosis
The diagnostic testing for vasculitis should be guided by the patient's history and physical exam. The clinician should ask about the duration, onset, and presence any associated symptoms such as weight loss or fatigue (that would indicate a systemic cause).[12] It is important to distinguish between IgA and non-IgA vasculitis. IgA vasculitis is more likely to present with abdominal pain, bloody urine, and joint pain.[13] In the case that the cause is not obvious, a reasonable initial workup would include a complete blood count, urinalysis, basic metabolic panel, fecal occult blood testing, erythrocyte sedimentation rate (ESR), and C-reactive protein level.[13] Small vessel cutaneous vasculitis is a diagnosis of exclusion and requires ruling out systemic causes of the skin findings.[14] Skin biopsy (punch or excisional) is the most definitive diagnostic test and should be performed with 48 hours of appearance of the vasculitis.[6] A skin biopsy will be able to determine if the clinical findings are truly due to a vasculitis or due to some other cause.[15]
Classification
Subtypes of small-vessel vasculitis include:[2]: 833–6
- IgA vasculitis (Henoch-Schönlein purpura)[16]
- Acute hemorrhagic edema of infancy
- Urticarial vasculitis
- Cryoglobulinemic vasculitis
- Erythema elevatum diutinum
- Granuloma faciale
- ANCA-associated vasculitis[13]
- Arthropod bites[13]
- Platelet dysfunction or deficiency[13]
- Cholesterol emboli[13]
- Septic emboli[13]
- Livedoid vasculopathy[13]
Treatment
Treatment should be directed towards the specific underlying cause of the vasculitis. If no underlying cause is found and the vasculitis is truly limited to the skin then treatment is primarily supportive.[13] Such treatment involves measures such as leg elevation, stockings, and topical steroids to relieve itching/burning. If the vasculitis does not self-resolve within 3–4 weeks, more aggressive treatment may be warranted.[13] Oral colchicine or dapsone are often used for this purpose. If rapid control of symptoms is needed, a short course of high-dose oral steroids may be given.[12] Immunosuppressive agents such as methotrexate and azathioprine may be used in truly refractory cases not responsive to colchicine or dapsone.[17]
See also
References
- ↑ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 978-1-4160-2999-1.
- 1 2 James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. ISBN 978-0-7216-2921-6.
- ↑ Lotti T, Ghersetich I, Comacchi C, Jorizzo JL (November 1998). "Cutaneous small-vessel vasculitis". J. Am. Acad. Dermatol. 39 (5 Pt 1): 667–87, quiz 688–90. doi:10.1016/S0190-9622(98)70039-8. PMID 9810883.
- ↑ Harrison's Principles of Internal Medicine. 18th edition. Page 2798.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Bolognia, Jean L.; Schaffer, Julie V.; Duncan, Karynne O.; Ko, Christine J. (2014-02-26). Dermatology essentials. Bolognia, Jean,, Schaffer, Julie V.,, Duncan, Karynne O.,, Ko, Christine J. Oxford. ISBN 9780702055393. OCLC 877821912.
- 1 2 3 4 5 6 7 8 9 10 Callen, Jeffrey P.; Jorizzo, Joseph L.; Zone, John J.; Piette, Warren; Rosenbach, Misha A.; Vleugels, Ruth Ann (2016-03-08). Dermatological signs of systemic disease. Callen, Jeffrey P., 1947- (Fifth ed.). Edinburgh. ISBN 9780323358316. OCLC 947111367.
- ↑ Upadhyay, AnimeshA; Kaushik, ShivaniB; Routt, Ethan; Phelps, Robert (2019). "Pustular vasculitis: Different names for same entity?". Indian Dermatology Online Journal. 0 (6): 721–723. doi:10.4103/idoj.idoj_415_18. ISSN 2229-5178. PMC 6859773. PMID 31807459.
- 1 2 3 Dermatopathology. Busam, Klaus J. (1st ed.). [Philadelphia]: Saunders/Elsevier. 2010. ISBN 9780443066542. OCLC 658000389.
{{cite book}}: CS1 maint: others (link) - 1 2 K., Abbas, Abul (2015-11-02). Basic immunology : functions and disorders of the immune system. Lichtman, Andrew H.,, Pillai, Shiv,, Baker, David L. (Medical illustrator),, Baker, Alexandra (Fifth ed.). St. Louis, Mo. ISBN 9780323390828. OCLC 929898069.
- 1 2 Kumar, Vinay; Abbas, Abul K.; Aster, Jon C. (2014). Robbins and Cotran pathologic basis of disease. Kumar, Vinay, 1944-, Abbas, Abul K.,, Aster, Jon C.,, Perkins, James A. (Ninth ed.). Philadelphia, PA. ISBN 9781455726134. OCLC 879416939.
- ↑ Giang, Jenny; Seelen, Marc A. J.; van Doorn, Martijn B. A.; Rissmann, Robert; Prens, Errol P.; Damman, Jeffrey (2018). "Complement Activation in Inflammatory Skin Diseases". Frontiers in Immunology. 9: 639. doi:10.3389/fimmu.2018.00639. ISSN 1664-3224. PMC 5911619. PMID 29713318.
- 1 2 Dermatology. Bolognia, Jean., Jorizzo, Joseph L., Schaffer, Julie V. (3rd ed.). [Philadelphia]: Elsevier Saunders. 2012. ISBN 9780723435716. OCLC 802040381.
{{cite book}}: CS1 maint: others (link) - 1 2 3 4 5 6 7 8 9 10 Small Vessel Vasculitis of the Skin, Rheumatic Disease Clinics of North America, 2015-02-01, Volume 41, Issue 1, Pages 21-32
- ↑ Emergency medicine : clinical essentials. Adams, James, 1962- (2nd ed.). Philadelphia, Pa: Elsevier/ Saunders. 2013. ISBN 9781455733941. OCLC 820203833.
{{cite book}}: CS1 maint: others (link) - ↑ L., BOLOGNIA, JEAN (2017). DERMATOLOGY. [S.l.]: ELSEVIER. ISBN 9780702062759. OCLC 981985926.
- ↑ J. C. Jennette; R. J. Falk; P. A. Bacon; et al. (January 2013). "2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides". Arthritis & Rheumatism. 65 (1): 1–11. doi:10.1002/art.37715. PMID 23045170. S2CID 20891451.
- ↑ 1950-, James, William D. (William Daniel) (2015-04-20). Andrews' diseases of the skin : clinical dermatology. Berger, Timothy G.,, Elston, Dirk M.,, Andrews, George Clinton, 1891-1978. (Twelfth ed.). Philadelphia, PA. ISBN 9780323319676. OCLC 910882314.
{{cite book}}: CS1 maint: numeric names: authors list (link)
External links
| Classification | |
|---|---|
| External resources |
|