Hepatic veno-occlusive disease
| Hepatic veno-occlusive disease | |
|---|---|
| Other names: Veno-occlusive disease with immunodeficiency; sinusoidal obstruction syndrome | |
| Symptoms | Weight gain, tender enlargement of the liver, ascites, jaundice |
| Diagnostic method | Liver biopsy |
| Differential diagnosis | Budd–Chiari syndrome |
| Prevention | Ursodeoxycholic acid |
| Treatment | Defibrotide |
| Deaths | 10-20% |
Hepatic veno-occlusive disease or veno-occlusive disease with immunodeficiency is a potentially life-threatening condition in which some of the small veins in the liver are obstructed. It is a complication of high-dose chemotherapy given before a bone marrow transplant and/or excessive exposure to hepatotoxic pyrrolizidine alkaloids. It is classically marked by weight gain due to fluid retention, increased liver size, and raised levels of bilirubin in the blood.[1] The name sinusoidal obstruction syndrome is preferred if hepatic veno-occlusive disease happens as a result of chemotherapy or bone marrow transplantation.[1][2]
Apart from chemotherapy, hepatic veno-occlusive disease may also occur after ingestion of certain plant alkaloids such as pyrrolizidine alkaloids (in some herbal teas),[1] and has been described as part of a rare hereditary disease called hepatic venoocclusive disease with immunodeficiency (which results from mutations in the gene coding for a protein called SP110).[3]
Signs and symptoms
Features of hepatic veno-occlusive disease include weight gain, tender enlargement of the liver, ascites, and yellow discoloration of the skin; it often is associated with acute kidney failure.[4]
Pathophysiology
In the bone marrow transplant setting, hepatic veno-occlusive disease is felt to be due to injury to the hepatic venous endothelium from the conditioning regimen. Toxic agents causing veno-occlusive disease include plants as well as the medication cyclophosphamide.
Diagnosis
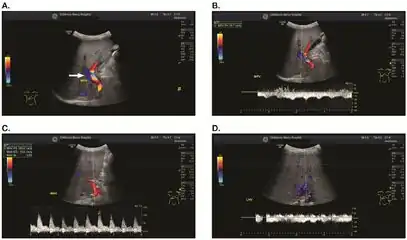
Doppler ultrasound of the liver is typically utilized to confirm or suggest the diagnosis. Common findings on liver doppler ultrasound include increased phasicity of portal veins with eventual development of portal flow reversal. The liver is usually enlarged but maintained normal echogenicity. A liver biopsy is required for a definitive diagnosis.
 a-d) Individual who developed VOD/SOS after HCT for acute myelogenous leukemia
a-d) Individual who developed VOD/SOS after HCT for acute myelogenous leukemia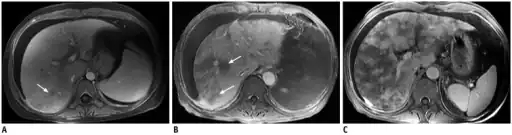 Post contrast-enhanced MR images show severity of patchy liver enhancement in hepatic sinusoidal obstruction syndrome.A. Grade 1. Arrow denotes mild patchy enhancement. B. Grade 2. Arrows denote moderate confluent patchy enhancement. C. Grade 3. Severe case with diffuse confluent patchy enhancement. Note all three cases demonstrate ascites.
Post contrast-enhanced MR images show severity of patchy liver enhancement in hepatic sinusoidal obstruction syndrome.A. Grade 1. Arrow denotes mild patchy enhancement. B. Grade 2. Arrows denote moderate confluent patchy enhancement. C. Grade 3. Severe case with diffuse confluent patchy enhancement. Note all three cases demonstrate ascites.
Treatment
Treatment generally includes supportive care including pain management and possibly diuretics.[5] In those with severe disease due to a bone marrow transplant, defibrotide is a proposed treatment.[6] It has been approved for use in severe cases in Europe and the United States.[7][8] A placebo controlled trial, however, has not been done as of 2016.[5]
Prognosis
Mild disease has a risk of death of about 10% while moderate disease has a risk of death of 20%.[5] When it occurs as a result of bone marrow transplant and multiorgan failure is present, the risk of death is greater than 80%.[6]
History
The first report on veno-occlusive disease, in 1920, was as a result of senecio poisoning in South Africa.[9] Subsequent reports were mostly in Jamaicans who had consumed herbal teas.[1] With the advent of bone marrow transplantation, most cases since its introduction have been in those undergoing treatment for leukemia.[1]
See also
References
- 1 2 3 4 5 Helmy A (January 2006). "Review article: updates in the pathogenesis and therapy of hepatic sinusoidal obstruction syndrome (SOS)". Aliment. Pharmacol. Ther. 23 (1): 11–25. doi:10.1111/j.1365-2036.2006.02742.x. PMID 16393276. S2CID 22462806. Archived from the original on 2012-12-09.
- ↑ DeLeve LD, Shulman HM, McDonald GB (February 2002). "Toxic injury to hepatic sinusoids: sinusoidal obstruction syndrome (veno-occlusive disease)". Semin. Liver Dis. 22 (1): 27–42. doi:10.1055/s-2002-23204. PMID 11928077.
- ↑ Roscioli T, Cliffe ST, Bloch DB (June 2006). "Mutations in the gene encoding the PML nuclear body protein Sp110 are associated with immunodeficiency and hepatic veno-occlusive disease" (PDF). Nat. Genet. 38 (6): 620–2. doi:10.1038/ng1780. PMID 16648851. S2CID 1466106. Archived (PDF) from the original on 2018-07-23. Retrieved 2021-01-19.
- ↑ RESERVED, INSERM US14 -- ALL RIGHTS. "Orphanet: Hepatic veno occlusive disease". www.orpha.net. Archived from the original on 2017-04-17. Retrieved 2016-12-26.
- 1 2 3 Dalle, JH; Giralt, SA (March 2016). "Hepatic Veno-Occlusive Disease after Hematopoietic Stem Cell Transplantation: Risk Factors and Stratification, Prophylaxis, and Treatment". Biology of Blood and Marrow Transplantation : Journal of the American Society for Blood and Marrow Transplantation. 22 (3): 400–9. doi:10.1016/j.bbmt.2015.09.024. PMID 26431626.
- 1 2 Fulgenzi, A; Ferrero, ME (2016). "Defibrotide in the treatment of hepatic veno-occlusive disease". Hepatic Medicine: Evidence and Research. 8: 105–113. doi:10.2147/HMER.S79243. PMC 5098529. PMID 27843363.
- ↑ Keating, GM (December 2014). "Defibrotide: a review of its use in severe hepatic veno-occlusive disease following haematopoietic stem cell transplantation". Clinical Drug Investigation. 34 (12): 895–904. doi:10.1007/s40261-014-0242-x. PMID 25351934. S2CID 21019656.
- ↑ "Press Announcements - FDA approves first treatment for rare disease in patients who receive stem cell transplant from blood or bone marrow". www.fda.gov. Archived from the original on 22 July 2017. Retrieved 18 July 2017.
- ↑ Willmot, F; Robertson, George (1920). "Senecio disease, or cirrhosis of the liver due to senecio poisoning". The Lancet. 196 (5069): 848–849. doi:10.1016/S0140-6736(01)00020-4. Archived from the original on 2019-12-16. Retrieved 2021-01-19.
Further reading
- Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease. St. Louis, Mo: Elsevier Saunders. ISBN 978-0-7216-0187-8.
- Wingard JR, Nichols WG, McDonald GB (2004). "Supportive care". Hematology Am Soc Hematol Educ Program. 1: 372–89. doi:10.1182/asheducation-2004.1.372. PMID 15561693.
- Dignan, Fiona L.; Wynn, Robert F.; Hadzic, Nedim; Karani, John; Quaglia, Alberto; Pagliuca, Antonio; Veys, Paul; Potter, Michael N. (1 November 2013). "BCSH/BSBMT guideline: diagnosis and management of veno-occlusive disease (sinusoidal obstruction syndrome) following haematopoietic stem cell transplantation". British Journal of Haematology. 163 (4): 444–457. doi:10.1111/bjh.12558. ISSN 1365-2141. PMID 24102514.
External links
| Classification | |
|---|---|
| External resources |
|