Jaundice
| Jaundice | |
|---|---|
| Other names: Icterus[1] | |
 | |
| Jaundice of the skin caused by pancreatic cancer | |
| Pronunciation |
|
| Specialty | Gastroenterology, hepatology, general surgery |
| Symptoms | Yellowish coloration of skin and whites of the eyes, itchiness[2][3] |
| Causes | High bilirubin levels[3] |
| Diagnostic method | Blood bilirubin, liver panel[3] |
| Differential diagnosis | Carotenemia, taking rifampin[4] |
| Treatment | Based on the underlying cause[5] |
Jaundice, also known as icterus, is a yellowish or greenish pigmentation of the skin and whites of the eyes due to high bilirubin levels.[3][6] Jaundice is commonly associated with itchiness.[2] There may also be pale feces and dark urine.[4] Jaundice in babies is also common with an estimated eighty percent affected during their first week of life.[7] While most cases of newborn jaundice are not harmful, if bilirubin levels are very high, brain damage — kernicterus — may occur.[8][7]
Jaundice is not a disease, but rather a medical sign of another health problem.[9] Normal levels of bilirubin in blood are below 1.0 mg/dL (17 µmol/L), while levels over 2–3 mg/dL (34-51 µmol/L) typically result in jaundice.[10][4] High blood bilirubin is divided into two types: unconjugated (indirect) and conjugated (direct).[11] Conjugated bilirubin can be confirmed with the presence of bilirubin in the urine.[12]
Causes of jaundice vary from non-serious to potentially fatal.[11] High unconjugated bilirubin may be due to excess red blood cell breakdown, large bruises, genetic conditions such as Gilbert's syndrome, not eating for a prolonged period of time, newborn jaundice, or thyroid problems.[4][11] High conjugated bilirubin may be due to liver diseases such as cirrhosis or hepatitis, infections, medications, or blockage of the bile duct.[4] In the developed world, the cause is more often blockage of the bile duct or medications; in the developing world, it is more often infections such as viral hepatitis, leptospirosis, schistosomiasis, or malaria.[4] Blockage of the bile duct may occur due to gallstones, cancer, or pancreatitis.[4] Medical imaging such as ultrasound is useful for detecting bile duct blockage.[12] Other conditions can also cause yellowish skin, but are not jaundice, including carotenemia — which can develop from eating large amounts of foods containing carotene — or medications like rifampin.[4]
Treatment of jaundice is typically determined by the underlying cause.[5] If a bile duct blockage is present, surgery is typically required; otherwise, management is medical.[5] Medical management may involve treating infectious causes and stopping medication that could be contributing to the jaundice.[5] Jaundice in newborns may be treated with phototherapy or exchanged transfusion depending on age and prematurity when the bilirubin is greater than 4–21 mg/dL (68-360 µmol/L).[10] The itchiness may be helped by draining the gallbladder or ursodeoxycholic acid.[2] The word jaundice is from the French jaunisse, meaning "yellow disease".[13][14]
Signs and symptoms
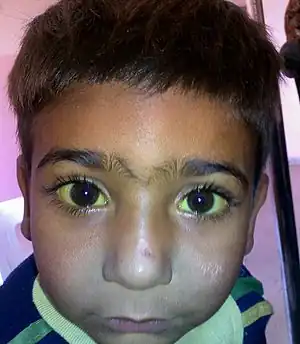
The most common signs of jaundice in adults are a yellowish discoloration of the white area of the eye (sclera) and skin[15] with scleral icterus presence indicating a serum bilirubin of at least 3 mg/dL.[16] Other common signs include dark urine (bilirubinuria) and pale, fatty stool (steatorrhea).[17] Because bilirubin is a skin irritant, jaundice is commonly associated with severe itchiness.[18][19]
Eye conjunctiva have a particularly high affinity for bilirubin deposition due to high elastin content. Slight increases in serum bilirubin can therefore be detected early on by observing yellowing of sclerae. Traditionally referred to as scleral icterus, this term is actually a misnomer because bilirubin deposition technically occurs in the conjunctival membranes overlying the avascular sclera. Thus, the proper term for the yellowing of "white of the eyes" is conjunctival icterus.[20]
A much less common sign of jaundice specifically during childhood is yellowish or greenish teeth. In developing children, hyperbilirubinemia may cause a yellow or green discoloration of teeth due to bilirubin deposition during the process of teeth calcification.[21] While this may occur in children with hyperbilirubinemia, teeth discoloration due to hyperbilirubinemia is not observed in individuals with adult-onset liver disease. Disorders associated with a rise in serum levels of conjugated bilirubin during early development can also cause dental hypoplasia.[22]
Complications
Hyperbilirubinemia, more precisely hyperbilirubinemia due to the unconjugated fraction, may cause bilirubin to accumulate in the gray matter of the central nervous system, potentially causing irreversible neurological damage leading to a condition known as kernicterus. Depending on the level of exposure, the effects range from unnoticeable to severe brain damage and even death. Newborns are especially vulnerable to hyperbilirubinemia-induced neurological damage and therefore must be carefully monitored for alterations in their serum bilirubin levels.
Individuals with parenchymal liver disease who have impaired hemostasis may develop bleeding problems.[23]
Causes
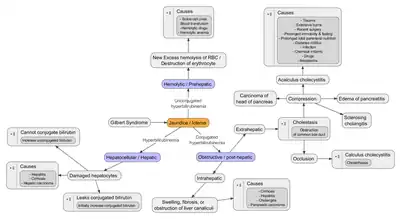
Jaundice is a sign indicating the presence of an underlying diseases involving abnormal bilirubin metabolism, liver dysfunction, or biliary tract obstruction. In general, jaundice is present when blood levels of bilirubin exceed 3 mg/dL.[16] Jaundice is classified into three categories, depending on which part of the physiological mechanism the pathology affects. The three categories are:
| Category | Definition |
|---|---|
| Pre-hepatic/hemolytic | The pathology occurs prior to the liver metabolism, due to either intrinsic causes to red blood cell rupture or extrinsic causes to red blood cell rupture. |
| Hepatic/hepatocellular | The pathology is due to damage of parenchymal liver cells. |
| Post-hepatic/cholestatic | The pathology occurs after bilirubin conjugation in the liver, due to obstruction of the biliary tract and/or decreased bilirubin excretion.[24] |
Before the liver
Pre-hepatic jaundice is most commonly caused by a pathological increased rate of red blood cell (erythrocyte) hemolysis. The increased breakdown of erythrocytes → increased unconjugated serum bilirubin → increased deposition of unconjugated bilirubin into mucosal tissue. The following diseases may cause jaundice due to increased erythrocyte hemolysis:
Liver
Hepatic jaundice is caused by abnormal liver metabolism of bilirubin. The major causes of hepatic jaundice are significant damage to hepatocytes — due to infectious, drug/medication-induced, auto-immune etiology — or, less commonly, due to inheritable genetic diseases. The following is a non-exhaustive list of hepatic causes to jaundice:
- acute hepatitis
- chronic hepatitis
- hepatotoxicity
- cirrhosis
- drug-induced hepatitis
- alcoholic liver disease
- Gilbert's syndrome (found in about 5% of the population, results in induced mild jaundice)
- Crigler-Najjar syndrome, type I
- Crigler-Najjar syndrome, type II
- leptospirosis
After liver
Post-hepatic jaundice (obstructive jaundice), is caused by a blockage of bile ducts which transport bile containing conjugated bilirubin out of the liver for excretion. The following is a list of conditions that can cause post-hepatic jaundice:
- Choledocholithiasis (common bile duct gallstones)
- Pancreatic cancer of the pancreatic head
- Biliary tract strictures
- Biliary atresia
- Primary biliary cholangitis
- Cholestasis of pregnancy
- Acute Pancreatitis
- Chronic Pancreatitis
- Pancreatic pseudocysts
- Mirizzi's syndrome
- Parasites ("liver flukes" of Opisthorchiidae and Fasciolidae)[25]
Newborns
Transient neonatal jaundice is one of the most common conditions occurring in newborns (children under 28 days of age) with more than eighty percent affected during their first week of life.[26] Jaundice in infants, like adults, is characterized by increased bilirubin levels (total serum bilirubin greater than 5 mg/dL). Jaundice in infants spreads in a cephalo-caudal pattern, affecting the face and neck before spreading down to the trunk and lower extremities in more severe cases.[27]
Causes of neonatal jaundice include normal physiologic jaundice, jaundice due to formula supplementation,[28] and hemolytic disorders that include hereditary spherocytosis, glucose-6-phosphate dehydrogenase deficiency, pyruvate kinase deficiency, ABO/Rh blood type autoantibodies, or infantile pyknocytosis. Serum bilirubin normally drops to a low level without any intervention required. In cases where bilirubin rises higher, a brain-damaging condition known as kernicterus can occur, leading to significant disability.[29] This condition has been rising in recent years due to less time spent outdoors. A Bili light is often the tool used for early treatment, which often consists of exposing the baby to intensive phototherapy. Sunbathing is effective treatment,[30][31] and has the advantage of ultra-violet-B, which promotes vitamin D production.[32] Bilirubin count is lowered through bowel movements and urination, so frequent and effective feedings are especially important.[33]
Pathophysiology
Jaundice is typically caused by an underlying pathological process that occurs at some point along the normal physiological pathway heme metabolism. A deeper understanding of the anatomical flow of normal heme metabolism is essential to appreciate the importance of pre-hepatic, hepatic, and post-hepatic categories. Thus, an anatomical approach to heme metabolism precedes a discussion of the pathophysiology of jaundice.
Heme metabolism
Before the liver
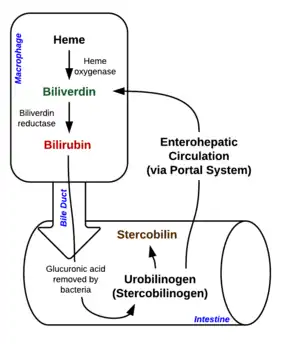
When red blood cells complete their life span of approximately 120 days, or if they are damaged, they rupture as they pass through the reticuloendothelial system and cell content including hemoglobin is released into circulation. Macrophages phagocytose free hemoglobin and split them into heme and globin. Two reactions then take place with the heme molecule. The first oxidation reaction is catalyzed by the microsomal enzyme heme oxygenase and results in biliverdin (green color pigment), iron, and carbon monoxide. The next step is the reduction of biliverdin to a yellow color tetrapyrrole pigment called bilirubin by cytosolic enzyme biliverdin reductase. This bilirubin is "unconjugated," "free" or "indirect" bilirubin. Approximately 4 milligrams of bilirubin per kilogram of blood is produced each day.[34] The majority of this bilirubin comes from the breakdown of heme from expired red blood cells in the process just described. Approximately twenty percent comes from other heme sources, however, including ineffective erythropoiesis, and the breakdown of other heme-containing proteins, such as muscle myoglobin and cytochromes.[34] The unconjugated bilirubin then travels to the liver through the bloodstream. Because this bilirubin is not soluble, it is transported through the blood bound to serum albumin.
Liver
Once unconjugated bilirubin arrives in the liver, a liver enzyme UDP-glucuronyl transferase conjugates bilirubin + glucuronic acid → bilirubin diglucuronide (conjugated bilirubin). Bilirubin that has been conjugated by the liver is water-soluble and excreted into the gallbladder.
After the liver
Bilirubin enters the intestinal tract via bile. In the intestinal tract, bilirubin is converted into urobilinogen by symbiotic intestinal bacteria. Most urobilinogen is converted into stercobilinogen and further oxidized into stercobilin. Stercobilin is excreted via feces, giving stool its characteristic brown coloration.[35] A small portion of urobilinogen is reabsorbed back into the gastrointestinal cells. Most reabsorbed urobilinogen undergoes hepatobiliary recirculation. A smaller portion of reabsorbed urobilinogen is filtrated into the kidneys. In the urine, urobilinogen is converted to urobilin, which gives urine its characteristic yellow color.[35]
Abnormalities
One way to understand jaundice pathophysiology is to organize it into disorders that cause increased bilirubin production (abnormal heme metabolism) or decreased bilirubin excretion (abnormal heme excretion).
Before liver
Pre-hepatic jaundice is attributed to a pathologic increase in bilirubin production. The pathophysiology is quite simple: an increased rate of erythrocyte hemolysis → increased bilirubin production → increased deposition of bilirubin in mucosal tissue → appearance of yellow hue.
Liver
Hepatic jaundice (hepatocellular jaundice) is due to significant damage to liver function → hepatic cell death and necrosis occur → impaired bilirubin transport across hepatocytes. Bilirubin transport across hepatocytes may be impaired at any point between hepatocellular uptake of unconjugated bilirubin and hepatocellular transport of conjugated bilirubin into the gallbladder. In addition, subsequent cellular edema due to inflammation causes mechanical obstruction of intrahepatic biliary tract. Most commonly, interferences in all three major steps of bilirubin metabolism — uptake, conjugation, and excretion — usually occur in hepatocellular jaundice. Thus, an abnormal rise in both unconjugated and conjugated bilirubin will be present. Because excretion (the rate-limiting step) is usually impaired to the greatest extent, conjugated hyperbilirubinemia predominates.[36]
The unconjugated bilirubin still enters the liver cells and becomes conjugated in the usual way. This conjugated bilirubin is then returned to the blood, probably by rupture of the congested bile canaliculi and direct emptying of the bile into the lymph leaving the liver. Thus, most of the bilirubin in the plasma becomes the conjugated type rather than the unconjugated type, and this conjugated bilirubin, which did not go to intestine to become urobilinogen, gives the urine the dark color.[37]
Bilirubinuria is due to excess conjugated bilirubin excreted in the urine.
After liver
Post-hepatic jaundice (obstructive jaundice) is due to a blockage of bile excretion from the biliary tract → increased conjugated bilirubin and bile salts. In complete obstruction of the bile duct, conjugated bilirubin cannot access the intestinal tract → no further bilirubin conversion to urobilinogen → no stercobilin or urobilin. Instead, excess conjugated bilirubin is filtrated into the urine without urobilinogen in obstructive jaundice. Conjugated bilirubin in urine (bilirubinuria) gives urine an abnormally dark brown color. Thus, the presence of pale stool (stercobilin absent from feces) and dark urine (conjugated bilirubin present in urine) suggest an obstructive cause of jaundice. Because these associated signs are also positive in many hepatic jaundice conditions, they cannot be a reliable clinical feature to distinguish obstruction versus hepatocellular jaundice causes.[38]
Diagnosis


Most people presenting with jaundice will have various predictable patterns of liver panel abnormalities, though significant variation does exist. The typical liver panel will include blood levels of enzymes found primarily from the liver, such as the aminotransferases (ALT, AST), and alkaline phosphatase (ALP); bilirubin (which causes the jaundice); and protein levels, specifically, total protein and albumin. Other primary lab tests for liver function include gamma glutamyl transpeptidase (GGT) and prothrombin time (PT). No single test can differentiate between various classifications of jaundice. A combination of liver function tests as well as other physical exam findings is essential to arrive at a diagnosis.
Labs
| Pre-hepatic Jaundice | Hepatic Jaundice | Post-hepatic Jaundice | |
|---|---|---|---|
| Total serum bilirubin | Normal / Increased | Increased | Increased |
| Conjugated bilirubin | Normal | Increased | Increased |
| Unconjugated bilirubin | Normal / Increased | Increased | Normal |
| Urobilinogen | Normal / Increased | Decreased | Decreased / Negative |
| Urine color | Normal[39] | Dark (urobilinogen, conjugated bilirubin) | Dark (conjugated bilirubin) |
| Stool color | Brown | Slightly pale | Pale, white |
| Alkaline phosphatase levels | Normal | Increased | Highly Increased |
| Alanine transferase and aspartate transferase levels | Highly Increased | Increased | |
| Conjugated bilirubin in urine | Not present | Present | Present |
Some bone and heart disorders can lead to an increase in ALP and the aminotransferases, so the first step in differentiating these from liver problems is to compare the levels of GGT, which will only be elevated in liver-specific conditions. The second step is distinguishing from biliary (cholestatic) or liver causes of jaundice and altered laboratory results. ALP and GGT levels will typically rise with one pattern while aspartate aminotransferase (AST) and alanine aminotransferase (ALT) rise in a separate pattern. If the ALP (10–45 IU/L) and GGT (18–85 IU/L) levels rise proportionately as high as the AST (12–38 IU/L) and ALT (10–45 IU/L) levels, this indicates a cholestatic problem. On the other hand, if the AST and ALT rise is significantly higher than the ALP and GGT rise, this indicates a liver problem. Finally, distinguishing between liver causes of jaundice, comparing levels of AST and ALT can prove useful. AST levels will typically be higher than ALT. This remains the case in most liver disorders except for hepatitis (viral or hepatotoxic). Alcoholic liver damage may see fairly normal ALT levels, with AST 10 times higher than ALT. On the other hand, if ALT is higher than AST, this is indicative of hepatitis. Levels of ALT and AST are not well correlated to the extent of liver damage, although rapid drops in these levels from very high levels can indicate severe necrosis. Low levels of albumin tend to indicate a chronic condition, while it is normal in hepatitis and cholestasis.
Lab results for liver panels are frequently compared by the magnitude of their differences, not the pure number, as well as by their ratios. The AST:ALT ratio can be a good indicator of whether the disorder is alcoholic liver damage (above 10), some other form of liver damage (above 1), or hepatitis (less than 1). Bilirubin levels greater than 10 times normal could indicate neoplastic or intrahepatic cholestasis. Levels lower than this tend to indicate hepatocellular causes. AST levels greater than 15 times normal tend to indicate acute hepatocellular damage. Less than this tend to indicate obstructive causes. ALP levels greater than 5 times normal tend to indicate obstruction, while levels greater than 10 times normal can indicate drug (toxin) induced cholestatic hepatitis or cytomegalovirus infection. Both of these conditions can also have ALT and AST greater than 20 times normal. GGT levels greater than 10 times normal typically indicate cholestasis. Levels 5–10 times tend to indicate viral hepatitis. Levels less than 5 times normal tend to indicate drug toxicity. Acute hepatitis will typically have ALT and AST levels rising 20–30 times normal (above 1000), and may remain significantly elevated for several weeks. Acetaminophen toxicity can result in ALT and AST levels greater than 50 times normal.
Laboratory findings depend on the cause of jaundice.
- Urine: conjugated bilirubin present, urobilinogen > 2 units but variable (except in children).
- Plasma proteins show characteristic changes.
- Plasma albumin level is low but plasma globulins are raised due to an increased formation of antibodies.
Unconjugated bilirubin is hydrophobic and therefore cannot be excreted in urine. Thus, the finding of increased urobilinogen in the urine without the presence of bilirubin in the urine (due to its unconjugated state) suggests hemolytic jaundice as the underlying disease process.[40] Urobilinogen will be greater than 2 units (i.e., hemolytic anemia causes increased heme metabolism; exception: infants where gut flora has not developed). Conversely, conjugated bilirubin is hydrophilic and thus can be detected as present in the urine — bilirubinuria — in contrast to unconjugated bilirubin which is absent in the urine.[12]
Imaging
Medical imaging such as ultrasound, CT scan, and HIDA scans are useful for detecting bile duct blockage.[12]
Differential diagnosis
Yellow discoloration of the skin, especially on the palms and the soles, but not of the sclera or inside the mouth is due to carotenemia—a harmless condition.[41]
Treatment
Treatment of jaundice will vary depending on the underlying cause.[5] If a bile duct blockage is present, surgery is typically required; otherwise, management will be medical.[5][42][43][44][45] Surgery in patients with obstructive jaundice are associated with significantly higher rates of complications (69% vs 38%, P=0.002) and mortality.[46] Medical management may involve treating infectious causes and stopping medication that could be contributing to the jaundice.[5] The itchiness may be helped by draining the gallbladder or ursodeoxycholic acid.[2]
Epidemiology
Jaundice in adults is rare.[47][46][48] Under the five year DISCOVERY programme in the UK, annual incidence of jaundice was 0.74 per 1000 individuals over age 45, although this rate may be slightly inflated due to the main goal of the programme collecting and analyzing cancer data in the population.[49] Jaundice is commonly associated with severity of disease with an incidence of up to 40% of patients requiring intensive care in ICU experiencing jaundice.[48] The causes of jaundice in the intensive care setting is both due to jaundice as the primary reason for ICU stay or as a morbidity to an underlying disease (i.e. sepsis).[48]
In the developed world, the most common causes of jaundice are blockage of the bile duct or medication-induced. In the developing world, the most common cause of jaundice is infectious such as viral hepatitis, leptospirosis, schistosomiasis, or malaria.[4]
Risk factors
Risk factors associated with high serum bilirubin levels include male gender, white ethnicities, and active smoking.[50] Mean serum total bilirubin levels in adults were found to be higher in men (0.72 ± 0.004 mg/dL) than women (0.52 ± 0.003 mg/dL).[50] Higher bilirubin levels in adults are found also in non-Hispanic white population (0.63 ± 0.004 mg/dL) and Mexican American population (0.61 ± 0.005 mg/dL) while lower in non-Hispanic black population (0.55 ± 0.005 mg/dL).[50] Bilirubin levels are higher in active smokers.[50]
Etymology
Jaundice comes from the French jaune, meaning yellow, jaunisse meaning "yellow disease". The medical term for it is icterus from the Greek word ikteros.[51] The origin of the word icterus is quite bizarre, coming from an ancient belief that jaundice could be cured from looking at the yellow bird icteria.[52] The term icterus is sometimes incorrectly used to refer to jaundice specifically of sclera.[51][53]
References
- ↑ Torre, Dario M.; Lamb, Geoffrey C.; Ruiswyk, Jerome Van; Schapira, Ralph M. (2009). Kochar's Clinical Medicine for Students. Lippincott Williams & Wilkins. p. 101. ISBN 9780781766999. Archived from the original on 2020-08-03. Retrieved 2020-05-28.
- 1 2 3 4 Bassari R, Koea JB (February 2015). "Jaundice associated pruritis: a review of pathophysiology and treatment". World Journal of Gastroenterology. 21 (5): 1404–13. doi:10.3748/wjg.v21.i5.1404. PMC 4316083. PMID 25663760.
- 1 2 3 4 Jaundice. MedlinePlus. Archived from the original on 27 August 2016. Retrieved 13 August 2016.
- 1 2 3 4 5 6 7 8 9 Jones, Roger (2004). Oxford Textbook of Primary Medical Care. Oxford University Press. p. 758. ISBN 9780198567820. Archived from the original on 2017-09-08.
- 1 2 3 4 5 6 7 Ferri, Fred F. (2014). Ferri's Clinical Advisor 2015: 5 Books in 1. Elsevier Health Sciences. p. 672. ISBN 9780323084307. Archived from the original on 2017-09-08.
- ↑ Buttaro, Terry Mahan; Trybulski, JoAnn; Polgar-Bailey, Patricia; Sandberg-Cook, Joanne (2012). Primary Care: A Collaborative Practice (4 ed.). Elsevier Health Sciences. p. 690. ISBN 978-0323075855. Archived from the original on 2017-09-08.
- 1 2 Kaplan M, Hammerman C (2017). "Hereditary Contribution to Neonatal Hyperbilirubinemia". Fetal and Neonatal Physiology. Elsevier: 933–942.e3. doi:10.1016/b978-0-323-35214-7.00097-4. ISBN 978-0-323-35214-7.
- ↑ "Facts about Jaundice and Kernicterus". CDC. February 23, 2015. Archived from the original on 8 August 2016. Retrieved 13 August 2016.
- ↑ Al-Tubaikh, Jarrah Ali (2016). Internal Medicine: An Illustrated Radiological Guide. Springer. p. 49. ISBN 978-3-319-39747-4. Archived from the original on 2021-08-29. Retrieved 2020-05-30.
- 1 2 Maisels MJ (March 2015). "Managing the jaundiced newborn: a persistent challenge". CMAJ. 187 (5): 335–43. doi:10.1503/cmaj.122117. PMC 4361106. PMID 25384650.
- 1 2 3 Winger J, Michelfelder A (September 2011). "Diagnostic approach to the patient with jaundice". Primary Care. 38 (3): 469–82, viii. doi:10.1016/j.pop.2011.05.004. PMID 21872092.
- 1 2 3 4 Roche SP, Kobos R (January 2004). "Jaundice in the adult patient". American Family Physician. 69 (2): 299–304. PMID 14765767.
- ↑ Dr. Chase's Family Physician, Farrier, Bee-keeper, and Second Receipt Book,: Being an Entirely New and Complete Treatise ... Chase publishing Company. 1873. p. 542. Archived from the original on 2017-09-08.
- ↑ Sullivan, Kara M.; Gourley, Glenn R. (2011). Jaundice. Pediatric Gastrointestinal and Liver Disease. Elsevier. pp. 176–186.e3. doi:10.1016/b978-1-4377-0774-8.10017-x. ISBN 978-1-4377-0774-8.
- ↑ Gondal B, Aronsohn A (December 2016). "A Systematic Approach to Patients with Jaundice". Seminars in Interventional Radiology. 33 (4): 253–258. doi:10.1055/s-0036-1592331. PMC 5088098. PMID 27904243.
- 1 2 Reuben, Adrian (2012). "Jaundice". Textbook of Clinical Gastroenterology and Hepatology. John Wiley & Sons, Ltd. pp. 84–92. doi:10.1002/9781118321386.ch15. ISBN 978-1-118-32138-6.
- ↑ Goroll, Allan H. (2009). Primary care medicine : office evaluation and management of the adult patient (6th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 496. ISBN 9780781775137. Archived from the original on 2017-09-08.
- ↑ James, William D. (2006). Andrews' diseases of the skin : clinical dermatology. Berger, Timothy G., Elston, Dirk M., Odom, Richard B., 1937- (10th ed.). Philadelphia: Saunders Elsevier. ISBN 0-7216-2921-0. OCLC 62736861.
- ↑ Bassari, Ramez (2015). "Jaundice associated pruritis: A review of pathophysiology and treatment". World Journal of Gastroenterology. 21 (5): 1404. doi:10.3748/wjg.v21.i5.1404. ISSN 1007-9327. PMID 25663760.
- ↑ McGee, Steven (2012), Evidence-Based Physical Diagnosis, Elsevier, pp. 63–69, doi:10.1016/b978-1-4377-2207-9.00007-0, ISBN 978-1-4377-2207-9
{{citation}}:|chapter=ignored (help); Missing or empty|title=(help) - ↑ Neville, Brad W. (2012). Oral and Maxillofacial Pathology (3rd ed.). Singapore: Elsevier. p. 798. ISBN 9789814371070.
- ↑ Amin SB, Karp JM, Benzley LP (May 2010). "Unconjugated hyperbilirubinemia and early childhood caries in a diverse group of neonates". American Journal of Perinatology. 27 (5): 393–7. doi:10.1055/s-0029-1243314. PMC 3264945. PMID 20013583.
- ↑ Neville, Brad W. (2012). Oral and Maxillofacial Pathology (3rd ed.). Singapore: Elsevier. p. 798. ISBN 9789814371070.
- ↑ Chatterjea MN, Shinde R (2012). Textbook of medical biochemistry (8th ed.). New Delhi: Jaypee Brothers Medical Publications (P) Ltd. p. 672. ISBN 978-93-5025-484-4.
- ↑ "CDC - Liver Flukes". www.cdc.gov. 2019-04-18. Archived from the original on 2020-06-05. Retrieved 2020-06-05.
- ↑ Maisels, M. Jeffrey (2015-03-17). "Managing the jaundiced newborn: a persistent challenge". Canadian Medical Association Journal. 187 (5): 335–343. doi:10.1503/cmaj.122117. ISSN 0820-3946. PMC 4361106. PMID 25384650. Archived from the original on 2021-08-28. Retrieved 2020-05-28.
- ↑ Telega, Grzegorz W. (2018), "Jaundice", Nelson Pediatric Symptom-Based Diagnosis, Elsevier, pp. 255–274.e1, ISBN 978-0-323-39956-2, archived from the original on 2021-08-28, retrieved 2020-05-28
- ↑ Bertini G, Dani C, Tronchin M, Rubaltelli FF (March 2001). "Is breastfeeding really favoring early neonatal jaundice?". Pediatrics. 107 (3): E41. doi:10.1542/peds.107.3.e41. PMID 11230622.
- ↑ Click R, Dahl-Smith J, Fowler L, DuBose J, Deneau-Saxton M, Herbert J (2013). "An osteopathic approach to reduction of readmissions for neonatal jaundice". Osteopathic Family Physician. 5 (1): 17–23. doi:10.1016/j.osfp.2012.09.005.
- ↑ Sumida K, Kawana M, Kouno E, Itoh T, Takano S, Narawa T, et al. (November 2013). "Importance of UDP-glucuronosyltransferase 1A1 expression in skin and its induction by UVB in neonatal hyperbilirubinemia". Molecular Pharmacology. 84 (5): 679–86. doi:10.1124/mol.113.088112. PMC 3807078. PMID 23950218.
- ↑ Salih FM (December 2001). "Can sunlight replace phototherapy units in the treatment of neonatal jaundice? An in vitro study". Photodermatology, Photoimmunology & Photomedicine. 17 (6): 272–7. doi:10.1034/j.1600-0781.2001.170605.x. PMID 11722753.
- ↑ Nakayama J, Imafuku S, Mori T, Sato C (October 2013). "Narrowband ultraviolet B irradiation increases the serum level of vitamin D₃ in patients with neurofibromatosis 1". The Journal of Dermatology. 40 (10): 829–31. doi:10.1111/1346-8138.12256. PMID 23961975.
- ↑ O'Keefe, Lori (May 2001). "Increased vigilance needed to prevent kernicterus in newborns". American Academy of Pediatrics. 18 (5): 231. Archived from the original on 2007-09-27.
- 1 2 Pashankar D, Schreiber RA (July 2001). "Jaundice in older children and adolescents". Pediatrics in Review. 22 (7): 219–26. doi:10.1542/pir.22-7-219. PMID 11435623. S2CID 11100275.
- 1 2 Berthelot, P.; Duvaldestin, Ph.; Fevery, J. (2018-01-18), "Physiology and Disorders of Human Bilirubin Metabolism", Bilirubin, CRC Press, pp. 173–214, doi:10.1201/9781351070119-6, ISBN 978-1-351-07011-9
- ↑ Mathew KG (2008). Medicine: Prep Manual for Undergraduates (3rd ed.). Elsevier India. pp. 296–297. ISBN 978-8131211540.
- ↑ Hall JE, Guyton AC (2011). Textbook of Medical Physiology. Saunders/Elsevier. p. 841. ISBN 978-1416045748.
- ↑ Beckingham IJ, Ryder SD (January 2001). "ABC of diseases of liver, pancreas, and biliary system. Investigation of liver and biliary disease". BMJ. 322 (7277): 33–6. doi:10.1136/bmj.322.7277.33. PMC 1119305. PMID 11141153.
- ↑ Llewelyn, Huw; Ang, Hock Aun; Lewis, Keir; Al-Abdullah, Anees (2014). Oxford Handbook of Clinical Diagnosis. Oxford University Press. p. 18. ISBN 9780199679867. Archived from the original on 2017-09-08.
- ↑ Cadogen, Mike (2019-04-21). "Bilirubin and Jaundice". Life in the Fast Lane. Archived from the original on 2020-01-26. Retrieved 2019-11-19.
- ↑ Carotenemia at eMedicine
- ↑ Wang, Long; Yu, Wei-Feng (March 2014). "Obstructive jaundice and perioperative management". Acta Anaesthesiologica Taiwanica. 52 (1): 22–29. doi:10.1016/j.aat.2014.03.002. ISSN 1875-4597. PMID 24999215.
- ↑ Dixon, Elijah; Vollmer, Charles M.; May, Gary R., eds. (2015). Management of Benign Biliary Stenosis and Injury. doi:10.1007/978-3-319-22273-8. ISBN 978-3-319-22272-1.
- ↑ Lorenz, Jonathan (2016-10-31). "Management of Malignant Biliary Obstruction". Seminars in Interventional Radiology. 33 (4): 259–267. doi:10.1055/s-0036-1592330. ISSN 0739-9529. PMC 5088103. PMID 27904244.
- ↑ Zhang, Lulu; Sanagapalli, Santosh; Stoita, Alina (2018-05-21). "Challenges in diagnosis of pancreatic cancer". World Journal of Gastroenterology. 24 (19): 2047–2060. doi:10.3748/wjg.v24.i19.2047. ISSN 1007-9327. PMC 5960811. PMID 29785074.
- 1 2 Björnsson, Einar; Gustafsson, Jonas; Borkman, Jakob; Kilander, Anders (2008). "Fate of patients with obstructive jaundice". Journal of Hospital Medicine. 3 (2): 117–123. doi:10.1002/jhm.272. ISSN 1553-5592. PMID 18438808.
- ↑ Ahmad, Jawad; Friedman, Scott L.; Dancygier, Henryk (2014). Mount Sinai Expert Guides: Hepatology. John Wiley & Sons. ISBN 9781118742525. Archived from the original on 2017-09-08.
- 1 2 3 Bansal, Vishal; Schuchert, Vaishali Dixit (December 2006). "Jaundice in the Intensive Care Unit". Surgical Clinics of North America. 86 (6): 1495–1502. doi:10.1016/j.suc.2006.09.007. ISSN 0039-6109. PMID 17116459.
- ↑ Taylor, Anna; Stapley, Sally; Hamilton, William (2012-08-01). "Jaundice in primary care: a cohort study of adults aged >45 years using electronic medical records". Family Practice. 29 (4): 416–420. doi:10.1093/fampra/cmr118. ISSN 0263-2136. PMID 22247287. Archived from the original on 2020-08-02. Retrieved 2020-06-02.
- 1 2 3 4 Zucker, Stephen D.; Horn, Paul S.; Sherman, Kenneth E. (October 2004). "Serum bilirubin levels in the U.S. Population: Gender effect and inverse correlation with colorectal cancer". Hepatology. 40 (4): 827–835. doi:10.1002/hep.1840400412. PMID 15382174.
- 1 2 "Definition of Icterus". MedicineNet.com. 2011. Archived from the original on 7 August 2012. Retrieved 3 February 2013.
- ↑ "Questions and Answers". JAMA: The Journal of the American Medical Association. 186 (6): 615. 1963-11-09. doi:10.1001/jama.1963.03710060101048. ISSN 0098-7484.
- ↑ Icterus | Define Icterus at Dictionary.com Archived 2010-12-31 at the Wayback Machine. Dictionary.reference.com. Retrieved on 2013-12-23.
External links
| Classification | |
|---|---|
| External resources |
 The dictionary definition of jaundice at Wiktionary
The dictionary definition of jaundice at Wiktionary