Acute esophageal necrosis
| Acute esophageal necrosis | |
|---|---|
| Other names: Gurvits syndrome, black esophagus, acute necrotizing esophagitis,[1] esophageal infarction | |
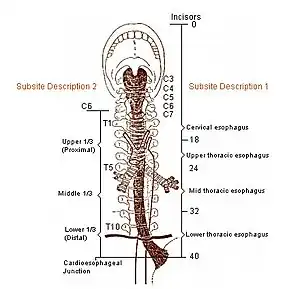 | |
| Areas represented in image (distals) are most common locations for acute esophageal necrosis to occur. AEN defines itself predominantly in the first of three distals of the esophagus.[2] | |
| Specialty | Gastroenterology |
| Risk factors | Cancer, hypertension, chronic lung disease, kidney failure, malnutrition, alcohol use disorder, recreational drug use |
| Diagnostic method | Upper endoscopy (EGD) |
| Treatment | Varies |
| Deaths | Mortality rate 30–50% |
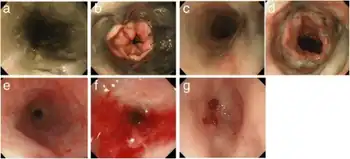
Acute esophageal necrosis (AEN), black esophagus, or Gurvits syndrome is a rare esophageal disorder. AEN defines itself with dark pigmentation of the esophagus, found during an upper gastrointestinal endoscopy.[2] Pigmentation is usually black friable mucosa. The disorder is extremely rare, as only 89 patients over a span of 40 years have received this diagnosis.[2] Specific study of the disorder's mortality rate is mentioned at 31.8%,[2] but new research suggests mortality rates vary from 30–50%.[3][4] The exact triggering mechanism for this disorder is still unknown, but is likely multifactorial.[2]
Signs and symptoms
AEN has never been recorded as a one symptom disorder, but instead present by multiple symptoms.[2] The symptoms vary from the severity of the disorder. The most classic sign of AEN is the dark pigmentation of esophageal mucosa in an upper endoscopy, usually viewed as an ulcer or as an infectious disease.[5] Necrosis can be found mostly between the three distals of the esophagus, but stops abruptly at the gastroesophageal junction.[2] The basic and most common symptoms reported are blood in stool and blood in vomiting. Upper gastrointestinal bleeding then is reported, and is very commonly represented in elderly patients.[3] Black or bloody stools and hematemesis account for over three quarters of the case presentations. Abdominal pain, nausea, vomiting, and unstable vital signs are common. A cardiovascular event (such as a heart attack) was reported in ten percent of the total known cases.[2]
Risk factors
Modifiable
Having cancer (current or previous) is currently one of the most prevalent out of all conditions among patients. High blood pressure, Chronic lung conditions, Alcohol use disorder, excessive alcohol use combined with other recreational drug use (e.g. cocaine), Kidney failure, and malnutrition are other major risk factors.[2][6]
Nonmodifiable
Lesser or unknown of effect
Diagnosis
Acute esophageal necrosis can only be diagnosed by an upper gastrointestinal endoscopy.[2][5][7]
Treatment
Currently, there is no direct treatment for AEN.[6] Only treatment is for the underlying main diseases or conditions. Appropriate hydration is set. Antacids are also added for further recovery support. Common support drugs of antacids are either H2 receptor antagonists, and/or a proton pump inhibitor.[6] Sucralfate was used as an option. Parenteral nutrition greatly increased chance of recovery. An esophagectomy can be issued if the disorder is severe enough.[6]
Prognosis
The prognosis for acute esophageal necrosis is generally poor, as the condition is associated with a high risk of mortality (up to 32%).[8] Most mortality is attributed to the underlying cause; mortality specifically caused by AEN is about 6 percent.[8]
Society and culture
Acute esophageal necrosis made an appearance on an American medical drama show, Dr. G: Medical Examiner. Jan Garavaglia, the show's host, receives a female body, that at time of the autopsy had a severe case of acute esophageal necrosis due to alcohol use disorder.
History
Acute esophageal necrosis was first described by Goldenberg et al. in 1990.[2][6] Cases have emerged since 1960, but have never been described as the common names for AEN. Due to its rarity, only 88 cases have been pronounced AEN, but most likely there are many more. Gurvits et al. describes AEN as "poorly described in medical literature".[2] Abdullah et al. published the first-ever systemic review on acute esophageal necrosis and reviewed around 154 patients reported in the literature at the time of publishing.[9]
References
- ↑ Julián Gómez L, Barrio J, Atienza R, et al. (November 2008). "[Acute esophageal necrosis. An underdiagnosed disease]". Rev Esp Enferm Dig (in español). 100 (11): 701–5. doi:10.4321/s1130-01082008001100006. PMID 19159174.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Gurvits GE, Shapsis A, Lau N, Gualtieri N, Robilotti JG (January 2007). "Acute esophageal necrosis: a rare syndrome". J. Gastroenterol. 42 (1): 29–38. doi:10.1007/s00535-006-1974-z. PMID 17322991. S2CID 32862916.
- 1 2 3 4 5 6 7 8 9 10 Khan AM, Hundal R, Ramaswamy V, Korsten M, Dhuper S (August 2004). "Acute esophageal necrosis and liver pathology, a rare combination". World J. Gastroenterol. 10 (16): 2457–8. doi:10.3748/wjg.v10.i16.2457. PMC 4576312. PMID 15285044.
- ↑ Watermeyer G, Shaw J, Krige J (2007). "Gastroentestinal: Acute necrotizing esophagitis". Journal of Gastroenterology and Hepatology. 22 (7): 1162. doi:10.1111/j.1440-1746.2007.05013.x. PMID 17608863. S2CID 71186463.
- 1 2 3 4 5 6 7 8 9 Trappe R, Pohl H, Forberger A, Schindler R, Reinke P (2007). "Acute esophageal necrosis (black esophagus) in the renal transplant recipient: manifestation of primary cytomegalovirus infection". Transplant Infectious Disease. 9 (1): 42–5. doi:10.1111/j.1399-3062.2006.00158.x. PMID 17313471. S2CID 1857761.
- 1 2 3 4 5 6 7 Carneiro M, Lescano M, Romanello L, et al. (2005). "Acute Esophageal Necrosis". Digestive Endoscopy. 17 (1): 89–92. doi:10.1111/j.1443-1661.2005.00464.x. S2CID 71488115.
- ↑ Grudell A, Mueller P, Viggiano T (2007). "Black esophagus: report of six cases and review of the literature, 1963–2003". Journal of Gastroenterology. 19 (2): 105–110. doi:10.1111/j.1442-2050.2006.00549.x. PMID 16643179.
- 1 2 Dias, E; Santos-Antunes, J; Macedo, G (November 2019). "Diagnosis and management of acute esophageal necrosis". Annals of Gastroenterology. 32 (6): 529–540. doi:10.20524/aog.2019.0418. PMC 6826069. PMID 31700229.
- ↑ Abdullah, Hafez Mohammad; Ullah, Waqas; Abdallah, Mohamed; Khan, Uzma; Hurairah, Abu; Atiq, Muslim (4 May 2019). "Clinical presentations, management, and outcomes of acute esophageal necrosis: a systemic review". Expert Review of Gastroenterology & Hepatology. 13 (5): 507–514. doi:10.1080/17474124.2019.1601555. PMID 30933549. S2CID 195661368.
External links
| Classification |
|---|