Fever
| Fever | |
|---|---|
| Other names: Pyrexia, febrile response, febrile[1][2] | |
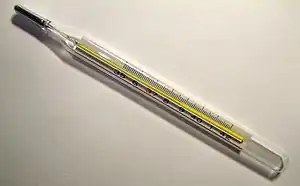 | |
| An analog medical thermometer showing a temperature of 38.7 °C or 101.7 °F | |
| Specialty | Infectious disease, pediatrics |
| Symptoms | Initially: shivering, feeling cold[3] Later: flushed, sweating[4] |
| Complications | Febrile seizure[5] |
| Causes | Increase in the body's temperature set point[6][7] |
| Diagnostic method | Temperature > between 37.2 and 38.3 °C (99.0 and 100.9 °F)[1][2][8] |
| Differential diagnosis | Hyperthermia[2] |
| Treatment | Based on underlying cause, not required for fever itself[3][9] |
| Medication | Ibuprofen, paracetamol (acetaminophen)[9][10] |
| Frequency | Common[3][11] |
Fever, also referred to as pyrexia, is defined as having a temperature above the normal range due to an increase in the body's temperature set point.[1][6][7] There is not a single agreed-upon upper limit for normal temperature with sources using values between 37.2 and 38.3 °C (99.0 and 100.9 °F) in humans.[1][2][8] The increase in set point triggers increased muscle contractions and causes a feeling of cold.[3] This results in greater heat production and efforts to conserve heat.[4] When the set point temperature returns to normal, a person feels hot, becomes flushed, and may begin to sweat.[4] Rarely a fever may trigger a febrile seizure, with this being more common in young children.[5] Fevers do not typically go higher than 41 to 42 °C (105.8 to 107.6 °F).[7]
A fever can be caused by many medical conditions ranging from non-serious to life-threatening.[12] This includes viral, bacterial, and parasitic infections—such as influenza, the common cold, meningitis, urinary tract infections, appendicitis, COVID-19, and malaria.[12][13] Non-infectious causes include vasculitis, deep vein thrombosis, connective tissue disease, side effects of medication, and cancer.[12][14] It differs from hyperthermia, in that hyperthermia is an increase in body temperature over the temperature set point, due to either too much heat production or not enough heat loss.[2]
Treatment to reduce fever is generally not required.[3][9] Treatment of associated pain and inflammation, however, may be useful and help a person rest.[9] Medications such as ibuprofen or paracetamol (acetaminophen) may help with this as well as lower temperature.[9][10] Measures such as putting a cool damp cloth on the forehead and having a slightly warm bath are not useful and may simply make a person more uncomfortable.[9] Children younger than three months require medical attention, as might people with serious medical problems such as a compromised immune system or people with other symptoms.[15] Hyperthermia does require treatment.[3]
Fever is one of the most common medical signs.[3] It is part of about 30% of healthcare visits by children[3] and occurs in up to 75% of adults who are seriously sick.[11] While fever evolved as a defense mechanism, treating fever does not appear to worsen outcomes.[16][17] Fever is often viewed with greater concern by parents and healthcare professionals than is usually deserved, a phenomenon known as fever phobia.[3][18]
Associated symptoms
A fever is usually accompanied by sickness behavior, which consists of lethargy, depression, loss of appetite, sleepiness, hyperalgesia, and the inability to concentrate. [19]
Diagnosis
| Temperature classification | ||||||||||||
|
||||||||||||
| Note: The difference between fever and hyperthermia is the underlying mechanism. Different sources have different cut-offs. | ||||||||||||
A range for normal temperatures has been found.[8] Central temperatures, such as rectal temperatures, are more accurate than peripheral temperatures.[25] Fever is generally agreed to be present if the elevated temperature is caused by a raised set point and:
- Temperature in the anus (rectum/rectal) is at or over 37.5–38.3 °C (99.5–100.9 °F)[2][8] An ear (tympanic) or forehead (temporal) temperature may also be used.[26][27]
- Temperature in the mouth (oral) is at or over 37.2 °C (99.0 °F) in the morning or over 37.7 °C (99.9 °F) in the afternoon[1][28]
- Temperature under the arm (axillary) is at or over 37.2 °C (99.0 °F)
In adults, the normal range of oral temperatures in healthy individuals is 33.2–38.2 °C (91.8–100.8 °F), while when taken rectally it is 34.4–37.8 °C (93.9–100.0 °F), for ear measurement it is 35.4–37.8 °C (95.7–100.0 °F), and for armpit (axillary) measurement it is 35.5–37.0 °C (95.9–98.6 °F).[29] Harrison's Principles of Internal Medicine defines a fever as a morning oral temperature of >37.2 °C (>98.9 °F) or an afternoon oral temperature of >37.7 °C (>99.9 °F) although normal daily temperature variation has been described as 0.5 °C (0.9 °F).[1]: 4012 Normal body temperatures vary depending on many factors, including age, sex, time of day, ambient temperature, activity level, and more.[30][31] A raised temperature is not always a fever; for example, the temperature of a healthy person rises when he or she exercises, but this is not considered a fever, as the set point is normal. On the other hand, a "normal" temperature may be a fever, if it is unusually high for that person; for example, medically frail elderly people have a decreased ability to generate body heat, so a "normal" temperature of 37.3 °C (99.1 °F) may represent a clinically significant fever.
Hyperthermia
Hyperthermia is an increase in body temperature over the temperature set point, due to either too much heat production or not enough heat loss.[2] It is an example of a high temperature phenomenon that is not a fever; rather, it occurs from a number of causes including heatstroke, neuroleptic malignant syndrome, malignant hyperthermia, as well as in response to stimulants such as substituted amphetamines and cocaine, and in idiosyncratic drug reactions, and serotonin syndrome.[32][1]: 117–121 Hyperthermia differs from hyperpyrexia, see section following.
Types
Various patterns of measured patient temperatures have been observed, some of which may be indicative of a particular medical diagnosis:
- Continuous fever, where temperature remains above normal throughout the day and does not fluctuate more than 1 °C in 24 hours (e.g. in lobar pneumonia, typhoid, meningitis, urinary tract infection, or typhus[33]);
- Intermittent fever, where the temperature elevation is present only for a certain period, later cycling back to normal (e.g., in malaria, leishmaniasis, pyemia, or sepsis);
- Remittent fever, where the temperature remains above normal throughout the day and fluctuates more than 1 °C in 24 hours (e.g., in infective endocarditis, or brucellosis).
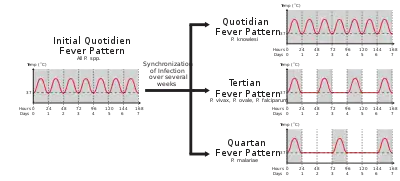
Among the types of intermittent fever are ones specific to cases of malaria caused by different pathogens. These are:[34][35]
- Quotidian fever, with a 24-hour periodicity, typical of malaria caused by Plasmodium knowlesi (P. knowlesi);
- Tertian fever, with a 48-hour periodicity, typical of later course malaria caused by P. falciparum, P. vivax, or P. ovale;[34]
- Quartan fever, with a 72-hour periodicity, typical of later course malaria caused by P. malariae.[34]
In addition, there is disagreement regarding whether a specific fever pattern is associated with Hodgkin's lymphoma—the Pel–Ebstein fever, with patient's argued to present high temperature for one week, followed by low for the next week, and so on, where the generality of this pattern is debated.[36]
Persistent fever that cannot be explained after repeated routine clinical inquiries is called fever of unknown origin.[1] A neutropenic fever, also called febrile neutropenia, is a fever in the absence of normal immune system function. Because of the lack of infection-fighting neutrophils, a bacterial infection can spread rapidly; this fever is, therefore, usually considered to require urgent medical attention. This kind of fever is more commonly seen in people receiving immune-suppressing chemotherapy than in apparently healthy people.
An old term, febricula, has been used to refer to low-grade fever, especially if the cause is unknown, no other symptoms are present, and the patient recovers fully in less than a week.[37]
Hyperpyrexia
Hyperpyrexia is an extreme elevation of body temperature which, depending upon the source, is classified as a core body temperature greater than or equal to 40.0 or 41.0 °C (104.0 or 105.8 °F); the range of hyperpyrexias include cases considered severe (≥ 40 °C) and extreme (≥ 42 °C).[1][38][39] It differs from hyperthermia in that one’s thermoregulatory system's set point for body temperature is set above normal, then heat is generated to achieve it. In contrast, hyperthermia involves body temperature rising above its set point due to outside factors.[1][40] The high temperatures of hyperpyrexia are considered medical emergencies, as they may indicate a serious underlying condition or lead to severe morbidity (including permanent brain damage), or to death.[41] A common cause of hyperpyrexia is an intracranial hemorrhage.[1] Other causes in emergency room settings include sepsis, Kawasaki syndrome,[42] neuroleptic malignant syndrome, drug overdose, serotonin syndrome, and thyroid storm.[41]
Differential diagnosis
Fever is a common symptom of many medical conditions:
- Infectious disease, e.g., COVID-19[13], Dengue, Ebola, gastroenteritis, HIV, influenza, Lyme disease, malaria, mononucleosis, as well as infections of the skin, e.g., abscesses and boils.
- Immunological diseases, e.g., relapsing polychondritis,[43] autoimmune hepatitis, granulomatosis with polyangiitis, Horton disease, inflammatory bowel diseases, Kawasaki disease, lupus erythematosus, sarcoidosis, and Still's disease;
- Tissue destruction, as a result of cerebral bleeding, crush syndrome, hemolysis, infarction, rhabdomyolysis, surgery, etc.;
- Cancers, particularly blood cancers such as leukemia and lymphomas;[44]
- Metabolic disorders, e.g., gout, and porphyria; and
- Inherited metabolic disorder, e.g., Fabry disease.[1]
Adult and pediatric manifestations for the same disease may differ; for instance, in COVID-19, one metastudy describes 92.8% of adults versus 43.9% of children presenting with fever.[13]
In addition, fever can result from a reaction to an incompatible blood product.[45]
Pathophysiology
Hypothalamus
Temperature is regulated in the hypothalamus. The trigger of a fever, called a pyrogen, results in the release of prostaglandin E2 (PGE2). PGE2 in turn acts on the hypothalamus, which creates a systemic response in the body, causing heat-generating effects to match a new higher temperature set point. Hence, the hypothalamus can be seen as working like a thermostat.[1] When the set point is raised, the body increases its temperature through both active generation of heat and retention of heat. Peripheral vasoconstriction both reduces heat loss through the skin and causes the person to feel cold. Norepinephrine increases thermogenesis in brown adipose tissue, and muscle contraction through shivering raises the metabolic rate.[47]
If these measures are insufficient to make the blood temperature in the brain match the new set point in the hypothalamus, the brain orchestrates heat effector mechanisms via the autonomic nervous system or primary motor center for shivering. These may be:
- Increased heat production by increased muscle tone, shivering (muscle movements to produce heat) and release of hormones like epinephrine; and
- Prevention of heat loss, e.g., through vasoconstriction.
When the hypothalamic set point moves back to baseline—either spontaneously or via medication—normal functions such as sweating, and the reverse of the foregoing processes (e.g., vasodilation, end of shivering, and nonshivering heat production) are used to cool the body to the new, lower setting.
This contrasts with hyperthermia, in which the normal setting remains, and the body overheats through undesirable retention of excess heat or over-production of heat. Hyperthermia is usually the result of an excessively hot environment (heat stroke) or an adverse reaction to drugs. Fever can be differentiated from hyperthermia by the circumstances surrounding it and its response to anti-pyretic medications.[1]
In infants, the autonomic nervous system may also activate brown adipose tissue to produce heat (non-exercise-associated thermogenesis, also known as non-shivering thermogenesis).
Increased heart rate and vasoconstriction contribute to increased blood pressure in fever.
Pyrogens
A pyrogen is a substance that induces fever.[48] In the presence of an infectious agent, such as bacteria, viruses, viroids, etc., the immune response of the body is to inhibit their growth and eliminate them. The most common pyrogens are endotoxins, which are lipopolysaccharides (LPS) produced by Gram-negative bacteria such as E. coli. But pyrogens include non-endotoxic substances (derived from microorganisms other than gram-negative-bacteria or from chemical substances) as well.[49] The types of pyrogens include internal (endogenous) and external (exogenous) to the body.
The "pyrogenicity" of given pyrogens varies: in extreme cases, bacterial pyrogens can act as superantigens and cause rapid and dangerous fevers.
Endogenous
Endogenous pyrogens are cytokines released from monocytes (which are part of the immune system).[50] In general, they stimulate chemical responses, often in the presence of an antigen, leading to a fever. Whilst they can be a product of external factors like exogenous pyrogens, they can also be induced by internal factors like damage associated from molecular patterns such as cases like rheumatoid arthritis or lupus.[51]
Major endogenous pyrogens are interleukin 1 (α and β)[52]: 1237–1248 and interleukin 6 (IL-6).[53] Minor endogenous pyrogens include interleukin-8, tumor necrosis factor-β, macrophage inflammatory protein-α and macrophage inflammatory protein-β as well as interferon-α, interferon-β, and interferon-γ.[52]: 1237–1248 Tumor necrosis factor-α (TNF) also acts as a pyrogen, mediated by interleukin 1 (IL-1) release.[54] These cytokine factors are released into general circulation, where they migrate to the brain's circumventricular organs where they are more easily absorbed than in areas protected by the blood–brain barrier. The cytokines then bind to endothelial receptors on vessel walls to receptors on microglial cells, resulting in activation of the arachidonic acid pathway.
Of these, IL-1β, TNF, and IL-6 are able to raise the temperature setpoint of an organism and cause fever. These proteins produce a cyclooxygenase which induces the hypothalamic production of PGE2 which then stimulates the release of neurotransmitters such as cyclic adenosine monophosphate and increases body temperature.[55]
Exogenous
Exogenous pyrogens are external to the body and are of microbial origin. In general, these pyrogens, including bacterial cell wall products, may act on Toll-like receptors in the hypothalamus and elevate the thermoregulatory setpoint.[56]
An example of a class of exogenous pyrogens are bacterial lipopolysaccharides (LPS) present in the cell wall of gram-negative bacteria. According to one mechanism of pyrogen action, an immune system protein, lipopolysaccharide-binding protein (LBP), binds to LPS, and the LBP–LPS complex then binds to a CD14 receptor on a macrophage. The LBP-LPS binding to CD14 results in cellular synthesis and release of various endogenous cytokines, e.g., interleukin 1 (IL-1), interleukin 6 (IL-6), and tumor necrosis factor-alpha (TNFα). A further downstream event is activation of the arachidonic acid pathway.[57]
PGE2 release
PGE2 release comes from the arachidonic acid pathway. This pathway (as it relates to fever), is mediated by the enzymes phospholipase A2 (PLA2), cyclooxygenase-2 (COX-2), and prostaglandin E2 synthase. These enzymes ultimately mediate the synthesis and release of PGE2.
PGE2 is the ultimate mediator of the febrile response. The set point temperature of the body will remain elevated until PGE2 is no longer present. PGE2 acts on neurons in the preoptic area (POA) through the prostaglandin E receptor 3 (EP3). EP3-expressing neurons in the POA innervate the dorsomedial hypothalamus (DMH), the rostral raphe pallidus nucleus in the medulla oblongata (rRPa), and the paraventricular nucleus (PVN) of the hypothalamus . Fever signals sent to the DMH and rRPa lead to stimulation of the sympathetic output system, which evokes non-shivering thermogenesis to produce body heat and skin vasoconstriction to decrease heat loss from the body surface. It is presumed that the innervation from the POA to the PVN mediates the neuroendocrine effects of fever through the pathway involving pituitary gland and various endocrine organs.
Selective advantage
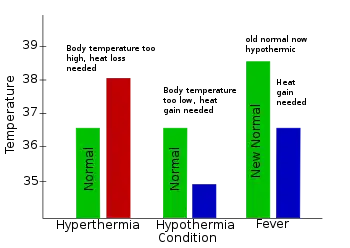
Hypothermia: Characterized in the center: Normal body temperature is shown in green, while the hypothermic temperature is shown in blue. As can be seen, hypothermia can be conceptualized as a decrease below the thermoregulatory set point.
Fever: Characterized on the right: Normal body temperature is shown in green. It reads "New Normal" because the thermoregulatory set point has risen. This has caused what was the normal body temperature (in blue) to be considered hypothermic.
Scholars viewing fever from an organismal and evolutionary perspective note the value to an organism of having a fever response, in particular in response to infective disease.[16][58][59] On the other hand, while fever evolved as a defense mechanism, treating fever does not appear to worsen outcomes.[16][17] Studies using warm-blooded vertebrates suggest that they recover more rapidly from infections or critical illness due to fever.[60] Other studies suggest reduced mortality in bacterial infections when fever was present.[61] Fever is thought to contribute to host defense,[16] as the reproduction of pathogens with strict temperature requirements can be hindered, and the rates of some important immunological reactions are increased by temperature.[62] Fever has been described in teaching texts as assisting the healing process in various ways, including:
Management
Fever does not necessarily need to be treated,[65] and most febrile cases recover without specific medical attention.[66] Although it is unpleasant, fever rarely rises to a dangerous level even if untreated. Damage to the brain generally does not occur until temperatures reach 42 °C (107.6 °F), and it is rare for an untreated fever to exceed 40.6 °C (105 °F).[67] Treating fever in people with sepsis does not affect outcomes.[68]
Conservative measures
Limited evidence supports sponging or bathing feverish children with tepid water.[69] The use of a fan or air conditioning may somewhat reduce the temperature and increase comfort. If the temperature reaches the extremely high level of hyperpyrexia, aggressive cooling is required (generally produced mechanically via conduction by applying numerous ice packs across most of the body or direct submersion in ice water).[41] In general, people are advised to keep adequately hydrated.[70] Whether increased fluid intake improves symptoms or shortens respiratory illnesses such as the common cold is not known.[71]
Medications
Medications that lower fevers are called antipyretics. The antipyretic ibuprofen is effective in reducing fevers in children.[72] It is more effective than acetaminophen (paracetamol) in children.[72] Ibuprofen and acetaminophen may be safely used together in children with fevers.[73][74] The efficacy of acetaminophen by itself in children with fevers has been questioned.[75] Ibuprofen is also superior to aspirin in children with fevers.[76] Additionally, aspirin is not recommended in children and young adults (those under the age of 16 or 19 depending on the country) due to the risk of Reye's syndrome.[77]
Using both paracetamol and ibuprofen at the same time or alternating between the two is more effective at decreasing fever than using only paracetamol or ibuprofen.[78] It is not clear if it increases child comfort.[78] Response or nonresponse to medications does not predict whether or not a child has a serious illness.[79]
With respect to the effect of antipyretics on the risk of death in those with infection, studies have found mixed results as of 2019.[80] Animal models have found worsened outcomes with the use of antipyretics in influenza as of 2010 but they have not been studied for this use in humans.[81]
Epidemiology
Fever is one of the most common medical signs.[3] It is part of about 30% of healthcare visits by children,[3] and occurs in up to 75% of adults who are seriously sick.[11] About 5% of people who go to an emergency room have a fever.[82]
History
A number of types of fever were known as early as 460 BC to 370 BC when Hippocrates was practicing medicine including that due to malaria (tertian or every 2 days and quartan or every 3 days).[83] It also became clear around this time that fever was a symptom of disease rather than a disease in and of itself.[83]
Society and culture
Fever is often viewed with greater concern by parents and healthcare professionals than might be deserved, a phenomenon known as fever phobia,[3][84] which is based in both caregiver's and parents' misconceptions about fever in children. Among them, many parents incorrectly believe that fever is a disease rather than a medical sign, that even low fevers are harmful, and that any temperature even briefly or slightly above the oversimplified "normal" number marked on a thermometer is a clinically significant fever.[84] They are also afraid of harmless side effects like febrile seizures and dramatically overestimate the likelihood of permanent damage from typical fevers.[84] The underlying problem, according to professor of pediatrics Barton D. Schmitt, is "as parents we tend to suspect that our children’s brains may melt."[85] As a result of these misconceptions parents are anxious, give the child fever-reducing medicine when the temperature is technically normal or only slightly elevated, and interfere with the child's sleep to give the child more medicine.[84]
Other species
Fever is an important feature for the diagnosis of disease in domestic animals. The body temperature of animals, which is taken rectally, is different from one species to another. For example, a horse is said to have a fever above 101 °F (38.3 °C).[86] In species that allow the body to have a wide range of "normal" temperatures, such as camels,[87] it is sometimes difficult to determine a febrile stage. Fever can also be behaviorally induced by invertebrates that do not have immune-system based fever. For instance, some species of grasshopper will thermoregulate to achieve body temperatures that are 2–5 °C higher than normal in order to inhibit the growth of fungal pathogens such as Beauveria bassiana and Metarhizium acridum.[88] Honeybee colonies are also able to induce a fever in response to a fungal parasite Ascosphaera apis.[88]
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Dinarello CA, Porat R (2018). "Chapter 15: Fever". In Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo, J (eds.). Harrison's Principles of Internal Medicine. Vol. 1–2 (20th ed.). New York, NY: McGraw-Hill. ISBN 9781259644030. Archived from the original on 1 August 2020. Retrieved 31 March 2020.
- 1 2 3 4 5 6 7 8 9 Axelrod YK, Diringer MN (May 2008). "Temperature management in acute neurologic disorders". Neurologic Clinics. 26 (2): 585–603, xi. doi:10.1016/j.ncl.2008.02.005. PMID 18514828.
- 1 2 3 4 5 6 7 8 9 10 11 12 Sullivan JE, Farrar HC (March 2011). "Fever and antipyretic use in children". Pediatrics. 127 (3): 580–87. doi:10.1542/peds.2010-3852. PMID 21357332.
- 1 2 3 Huether, Sue E. (2014). Pathophysiology: The Biologic Basis for Disease in Adults and Children (7th ed.). Elsevier Health Sciences. p. 498. ISBN 978-0323293754. Archived from the original on 1 August 2020. Retrieved 29 July 2020.
- 1 2 CDC Staff (31 March 2020). "Taking Care of Someone Who is Sick: Caring for Someone Sick at Home". Archived from the original on 24 March 2015. Retrieved 8 May 2015.
- 1 2 Kluger, Matthew J. (2015). Fever: Its Biology, Evolution, and Function. Princeton University Press. p. 57. ISBN 978-1400869831.
- 1 2 3 Garmel GM, Mahadevan SV, eds. (2012). "Fever in adults". An introduction to clinical emergency medicine (2nd ed.). Cambridge: Cambridge University Press. p. 375. ISBN 978-0521747769. Archived from the original on 1 August 2020. Retrieved 29 July 2020.
- 1 2 3 4 5 6 Laupland KB (July 2009). "Fever in the critically ill medical patient". Critical Care Medicine. 37 (7 Suppl): S273-8. doi:10.1097/CCM.0b013e3181aa6117. PMID 19535958.
- 1 2 3 4 5 6 Richardson M, Purssell E (September 2015). "Who's afraid of fever?". Archives of Disease in Childhood. 100 (9): 818–20. doi:10.1136/archdischild-2014-307483. PMID 25977564. S2CID 206857750.
- 1 2 Garmel GM, Mahadevan SV, eds. (2012). An introduction to clinical emergency medicine (2nd ed.). Cambridge: Cambridge University Press. p. 401. ISBN 978-0521747769.
- 1 2 3 Kiekkas P, Aretha D, Bakalis N, Karpouhtsi I, Marneras C, Baltopoulos GI (August 2013). "Fever effects and treatment in critical care: literature review". Australian Critical Care. 26 (3): 130–35. doi:10.1016/j.aucc.2012.10.004. PMID 23199670.
- 1 2 3 Garmel GM, Mahadevan SV, eds. (2012). An introduction to clinical emergency medicine (2nd ed.). Cambridge: Cambridge University Press. p. 5. ISBN 978-0521747769.
- 1 2 3 Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, Villamizar-Peña R, Holguin-Rivera Y, Escalera-Antezana JP, Alvarado-Arnez LE, Bonilla-Aldana DK, Franco-Paredes C (13 March 2020). "Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis". Travel Medicine and Infectious Disease. 34: 101623. doi:10.1016/j.tmaid.2020.101623. PMC 7102608. PMID 32179124.
- ↑ Dayal R, Agarwal D (January 2016). "Fever in Children and Fever of Unknown Origin". Indian Journal of Pediatrics. 83 (1): 38–43. doi:10.1007/s12098-015-1724-4. PMID 25724501. S2CID 34481402.
- ↑ "Fever". MedlinePlus. 30 August 2014. Archived from the original on 11 May 2009.
- 1 2 3 4 Schaffner A (March 2006). "Fieber – nützliches oder schädliches, zu behandelndes Symptom?" [Fever–useful or noxious symptom that should be treated?]. Therapeutische Umschau (in Deutsch). 63 (3): 185–88. doi:10.1024/0040-5930.63.3.185. PMID 16613288. Abstract alone is in German and in English.
- 1 2 Niven DJ, Stelfox HT, Laupland KB (June 2013). "Antipyretic therapy in febrile critically ill adults: A systematic review and meta-analysis". Journal of Critical Care. 28 (3): 303–10. doi:10.1016/j.jcrc.2012.09.009. PMID 23159136.
- ↑ Crocetti M, Moghbeli N, Serwint J (June 2001). "Fever Phobia Revisited: Have Parental Misconceptions About Fever Changed in 20 Years?". Pediatrics. 107 (6): 1241–1246. doi:10.1542/peds.107.6.1241. PMID 11389237.
- ↑ Kelley KW, Bluthé RM, Dantzer R, Zhou JH, Shen WH, Johnson RW, Broussard SR (February 2003). "Cytokine-induced sickness behavior". Brain, Behavior, and Immunity. 17 Suppl 1 (1): S112–18. doi:10.1016/S0889-1591(02)00077-6. PMID 12615196. S2CID 25400611.
- ↑ Marx, John (2006). Rosen's emergency medicine : concepts and clinical practice (6th ed.). Philadelphia: Mosby/Elsevier. p. 2239. ISBN 978-0-323-02845-5. OCLC 58533794.
{{cite book}}: CS1 maint: date and year (link) - ↑ Hutchison JS, Ward RE, Lacroix J, Hébert PC, Barnes MA, Bohn DJ, et al. (June 2008). "Hypothermia therapy after traumatic brain injury in children". The New England Journal of Medicine. 358 (23): 2447–56. doi:10.1056/NEJMoa0706930. PMID 18525042.
- ↑ Pryor, Jennifer A.; Prasad, Ammani S. (2008). Physiotherapy for Respiratory and Cardiac Problems: Adults and Paediatrics. Elsevier Health Sciences. p. 8. ISBN 978-0702039744.
Body temperature is maintained within the range 36.5-37.5 °C. It is lowest in the early morning and highest in the afternoon.
- ↑ Grunau BE, Wiens MO, Brubacher JR (September 2010). "Dantrolene in the treatment of MDMA-related hyperpyrexia: a systematic review". Cjem. 12 (5): 435–42. doi:10.1017/s1481803500012598. PMID 20880437.
Dantrolene may also be associated with improved survival and reduced complications, especially in patients with extreme (≥ 42 °C) or severe (≥ 40 °C) hyperpyrexia
- ↑ Sharma HS, ed. (2007). Neurobiology of Hyperthermia (1st ed.). Elsevier. pp. 175–177, 485. ISBN 9780080549996. Retrieved 19 November 2016.
Despite the myriad of complications associated with heat illness, an elevation of core temperature above 41.0 °C (often referred to as fever or hyperpyrexia) is the most widely recognized symptom of this syndrome.
- ↑ Niven DJ, Gaudet JE, Laupland KB, Mrklas KJ, Roberts DJ, Stelfox HT (November 2015). "Accuracy of peripheral thermometers for estimating temperature: a systematic review and meta-analysis". Annals of Internal Medicine. 163 (10): 768–77. doi:10.7326/M15-1150. PMID 26571241. S2CID 4004360.
- ↑ "Measuring a Baby's Temperature". www.hopkinsmedicine.org. Archived from the original on 3 November 2019. Retrieved 10 September 2019.
- ↑ "Tips for taking your child's temperature". Mayo Clinic. Archived from the original on 3 November 2019. Retrieved 10 September 2019.
- ↑ Barone JE (August 2009). "Fever: Fact and fiction". The Journal of Trauma. 67 (2): 406–09. doi:10.1097/TA.0b013e3181a5f335. PMID 19667898.
- ↑ Sund-Levander M, Forsberg C, Wahren LK (June 2002). "Normal oral, rectal, tympanic and axillary body temperature in adult men and women: a systematic literature review". Scandinavian Journal of Caring Sciences. 16 (2): 122–28. doi:10.1046/j.1471-6712.2002.00069.x. PMID 12000664.
- ↑ Garami, András; Székely, Miklós (6 May 2014). "Body temperature". Temperature: Multidisciplinary Biomedical Journal. 1 (1): 28–29. doi:10.4161/temp.29060. ISSN 2332-8940. PMC 4972507. PMID 27583277.
- ↑ "Body temperature: What is the new normal?". www.medicalnewstoday.com. Archived from the original on 31 July 2020. Retrieved 7 April 2020.
- ↑ Tintinalli, Judith (2004). Emergency Medicine: A Comprehensive Study Guide (Sixth ed.). McGraw-Hill Professional. p. 1187. ISBN 9780071388757.
- ↑ Typhoid fever may show a specific fever pattern, a Wunderlich curve, with a slow stepwise increase and a high plateau (drops due to fever-reducing drugs are excluded).
- 1 2 3 Ferri FF (2009). "Chapter 332. Protozoal infections". Ferri's Color Atlas and Text of Clinical Medicine. Elsevier Health Sciences. pp. 1159ff. ISBN 9781416049197. Archived from the original on 3 June 2016. Retrieved 31 March 2020.
- ↑ Muhammad I, Nasir, SA (2009). Bedside Techniques: Methods of Clinical Examination. Multan, Pakistan: Saira Publishers/Salamat Iqbal Press.
- ↑ Hilson AJ (July 1995). "Pel-Ebstein fever". The New England Journal of Medicine. 333 (1): 66–67. doi:10.1056/NEJM199507063330118. PMID 7777006., which cites Richard Asher's lecture, "Making Sense" [Lancet (1959) 2: 359].
- ↑ Thomas, RL (1906). The Eclectic Practice of Medicine. Scudder Brothers. p. 261. Retrieved 31 March 2020.
- ↑ Grunau BE, Wiens MO, Brubacher JR (September 2010). "Dantrolene in the treatment of MDMA-related hyperpyrexia: a systematic review". Canadian Journal of Emergency Medicine. 12 (5): 435–42. doi:10.1017/s1481803500012598. PMID 20880437.
Dantrolene may also be associated with improved survival and reduced complications, especially in patients with extreme (≥ 42 °C) or severe (≥ 40 °C) hyperpyrexia
- ↑ Sharma HS, ed. (2007). Neurobiology of Hyperthermia (1st ed.). Elsevier. pp. 175–77, 485. ISBN 978-0080549996. Archived from the original on 8 September 2017. Retrieved 19 November 2016.
Despite the myriad of complications associated with heat illness, an elevation of core temperature above 41.0 °C (often referred to as fever or hyperpyrexia) is the most widely recognized symptom of this syndrome.
- ↑ See section in Chapter 15 therein, the section on "Fever versus hyperthermia".
- 1 2 3 McGugan EA (March 2001). "Hyperpyrexia in the emergency department". Emergency Medicine. 13 (1): 116–20. doi:10.1046/j.1442-2026.2001.00189.x. PMID 11476402.
- ↑ Marx (2006), p. 2506.
- ↑ Puéchal X, Terrier B, Mouthon L, Costedoat-Chalumeau N, Guillevin L, Le Jeunne C (March 2014). "Relapsing polychondritis". Joint, Bone, Spine. 81 (2): 118–24. doi:10.1016/j.jbspin.2014.01.001. PMID 24556284.
- ↑ "Signs and Symptoms of Cancer | Do I Have Cancer?". www.cancer.org. Archived from the original on 30 November 2020. Retrieved 20 June 2020.
- ↑ Dean, Laura (2005). Blood transfusions and the immune system. National Center for Biotechnology Information (US). Archived from the original on 10 September 2015. Retrieved 29 July 2020.
- ↑ Massignan C, Cardoso M, Porporatti AL, Aydinoz S, Canto G, Mezzomo LA, Bolan M (March 2016). "Signs and Symptoms of Primary Tooth Eruption: A Meta-analysis". Pediatrics. 137 (3): e20153501. doi:10.1542/peds.2015-3501. PMID 26908659. Archived from the original on 21 February 2016.
- ↑ Evans SS, Repasky EA, Fisher DT (June 2015). "Fever and the thermal regulation of immunity: the immune system feels the heat". Nature Reviews. Immunology. 15 (6): 335–49. doi:10.1038/nri3843. PMC 4786079. PMID 25976513.
- ↑ Hagel, Lars; Jagschies, Günter; Sofer, Gail (1 January 2008). "5 - Analysis". Handbook of Process Chromatography (2nd ed.). Academic Press. pp. 127–145. doi:10.1016/b978-012374023-6.50007-5. ISBN 978-0-12-374023-6.
- ↑ Kojima K (1 January 2012). "17 - Biological evaluation and regulation of medical devices in Japan". In Boutrand J (ed.). Biocompatibility and Performance of Medical Devices. Woodhead Publishing Series in Biomaterials. Woodhead Publishing. pp. 404–448. doi:10.1533/9780857096456.4.404. ISBN 978-0-85709-070-6.
- ↑ Constable, Peter D.; Hinchcliff, Kenneth W.; Done, Stanley H.; Grünberg, Walter, eds. (1 January 2017). "4 - General Systemic States". =Veterinary Medicine (11th ed.). W.B. Saunders. pp. 43–112. doi:10.1016/b978-0-7020-5246-0.00004-8. ISBN 978-0-7020-5246-0. S2CID 214758182.
- ↑ Dinarello CA (31 March 2015). "The history of fever, leukocytic pyrogen and interleukin-1". Temperature. 2 (1): 8–16. doi:10.1080/23328940.2015.1017086. PMC 4843879. PMID 27226996.
- 1 2 Stitt, John (2008). "Chapter 59: Regulation of Body Temperature". In Boron WF, Boulpaep, EL (eds.). Medical Physiology: A Cellular and Molecular Approach (2nd ed.). Philadelphia, PA: Elsevier Saunders. ISBN 9781416031154. Archived from the original on 1 August 2020. Retrieved 2 April 2020.
- ↑ Murphy, Kenneth (Kenneth M.) (2017). Janeway's immunobiology. Weaver, Casey (9th ed.). New York, NY, USA. pp. 118–119. ISBN 978-0-8153-4505-3. OCLC 933586700.
- ↑ Stefferl A, Hopkins SJ, Rothwell NJ, Luheshi GN (August 1996). "The role of TNF-alpha in fever: opposing actions of human and murine TNF-alpha and interactions with IL-beta in the rat". British Journal of Pharmacology. 118 (8): 1919–24. doi:10.1111/j.1476-5381.1996.tb15625.x. PMC 1909906. PMID 8864524.
- ↑ Srinivasan, Lakshmi; Harris, Mary Catherine; Kilpatrick, Laurie E. (1 January 2017). "128 - Cytokines and Inflammatory Response in the Fetus and Neonate". In Polin, Richard A.; Abman, Steven H.; Rowitch, David H.; Benitz, William E. (eds.). Fetal and Neonatal Physiology (5th ed.). Elsevier. pp. 1241–1254.e4. doi:10.1016/b978-0-323-35214-7.00128-1. ISBN 978-0-323-35214-7.
- ↑ Wilson, Mary E.; Boggild, Andrea K. (1 January 2011). "130 - Fever and Systemic Symptoms". In Guerrant, Richard L.; Walker, David H.; Weller, Peter F. (eds.). Tropical Infectious Diseases: Principles, Pathogens and Practice (3rd ed.). W.B. Saunders. pp. 925–938. doi:10.1016/b978-0-7020-3935-5.00130-0. ISBN 978-0-7020-3935-5.
- ↑ Roth J, Blatteis CM (October 2014). "Mechanisms of fever production and lysis: Lessons from experimental LPS fever". Comprehensive Physiology. 4 (4): 1563–604. doi:10.1002/cphy.c130033. ISBN 9780470650714. PMID 25428854.
- ↑ Soszyński D (2003). "[The pathogenesis and the adaptive value of fever]". Postepy Higieny I Medycyny Doswiadczalnej (in Polish). 57 (5): 531–54. PMID 14737969.
{{cite journal}}: CS1 maint: unrecognized language (link) - ↑ Kluger MJ, Kozak W, Conn CA, Leon LR, Soszynski D (September 1998). "Role of fever in disease". Annals of the New York Academy of Sciences. 856 (1): 224–33. Bibcode:1998NYASA.856..224K. doi:10.1111/j.1749-6632.1998.tb08329.x. PMID 9917881.
- ↑ Su F, Nguyen ND, Wang Z, Cai Y, Rogiers P, Vincent JL (June 2005). "Fever control in septic shock: beneficial or harmful?". Shock. 23 (6): 516–20. PMID 15897803.
- ↑ Rantala S, Vuopio-Varkila J, Vuento R, Huhtala H, Syrjänen J (April 2009). "Predictors of mortality in beta-hemolytic streptococcal bacteremia: a population-based study". The Journal of Infection. 58 (4): 266–72. doi:10.1016/j.jinf.2009.01.015. PMID 19261333.
- ↑ Fischler MP, Reinhart WH (May 1997). "[Fever: friend or enemy?]". Schweizerische Medizinische Wochenschrift (in German). 127 (20): 864–70. PMID 9289813.
{{cite journal}}: CS1 maint: unrecognized language (link) - 1 2 3 4 Craven RF, Hirnle CJ (2003). Fundamentals of Nursing: Human Health and Function (4th ed.). Philadelphia, PA: Lippincott Williams & Wilkins. ISBN 9780781758185. Retrieved 2 April 2020.
{{cite book}}: CS1 maint: uses authors parameter (link) - ↑ Lewis SM, Dirksen SR, Heitkemper MM (2005). Medical-Surgical Nursing: Assessment and Management of Clinical Problems (6th ed.). Amsterdam, NL: Elsevier-Health Sciences. ISBN 9780323031059. Archived from the original on 1 August 2020. Retrieved 2 April 2020.
{{cite book}}: CS1 maint: uses authors parameter (link) - ↑ "Fever". Medline Plus Medical Encyclopedia. U.S. National Library of Medicine. Archived from the original on 11 May 2009. Retrieved 20 May 2009.
- ↑ "What To Do If You Get Sick: 2009 H1N1 and Seasonal Flu". Centers for Disease Control and Prevention. 7 May 2009. Archived from the original on 3 November 2009. Retrieved 1 November 2009.
- ↑ Edward James Walter and Mike Carraretto (2016). "The neurological and cognitive consequences of hyperthermia". Critical Care. 20 (1): 199. doi:10.1186/s13054-016-1376-4. PMC 4944502. PMID 27411704.
{{cite journal}}: CS1 maint: uses authors parameter (link) - ↑ Drewry AM, Ablordeppey EA, Murray ET, Stoll CR, Izadi SR, Dalton CM, Hardi AC, Fowler SA, Fuller BM, Colditz GA (May 2017). "Antipyretic Therapy in Critically Ill Septic Patients: A Systematic Review and Meta-Analysis". Critical Care Medicine. 45 (5): 806–13. doi:10.1097/CCM.0000000000002285. PMC 5389594. PMID 28221185.
- ↑ Meremikwu M, Oyo-Ita A (2003). Meremikwu MM (ed.). "Physical methods for treating fever in children". The Cochrane Database of Systematic Reviews (2): CD004264. doi:10.1002/14651858.CD004264. PMC 6532675. PMID 12804512.
- ↑ "Fever". National Institute of Health. Archived from the original on 30 April 2016.
- ↑ Guppy MP, Mickan SM, Del Mar CB, Thorning S, Rack A (February 2011). "Advising patients to increase fluid intake for treating acute respiratory infections". The Cochrane Database of Systematic Reviews (2): CD004419. doi:10.1002/14651858.CD004419.pub3. PMC 7197045. PMID 21328268.
- 1 2 Perrott DA, Piira T, Goodenough B, Champion GD (June 2004). "Efficacy and safety of acetaminophen vs ibuprofen for treating children's pain or fever: a meta-analysis". Archives of Pediatrics & Adolescent Medicine. 158 (6): 521–26. doi:10.1001/archpedi.158.6.521. PMID 15184213.
- ↑ Hay AD, Redmond NM, Costelloe C, Montgomery AA, Fletcher M, Hollinghurst S, Peters TJ (May 2009). "Paracetamol and ibuprofen for the treatment of fever in children: the PITCH randomised controlled trial". Health Technology Assessment. 13 (27): iii–iv, ix–x, 1–163. doi:10.3310/hta13270. PMID 19454182.
- ↑ Southey ER, Soares-Weiser K, Kleijnen J (September 2009). "Systematic review and meta-analysis of the clinical safety and tolerability of ibuprofen compared with paracetamol in paediatric pain and fever". Current Medical Research and Opinion. 25 (9): 2207–22. doi:10.1185/03007990903116255. PMID 19606950. S2CID 31653539.
- ↑ Meremikwu M, Oyo-Ita A (2002). "Paracetamol for treating fever in children". The Cochrane Database of Systematic Reviews (2): CD003676. doi:10.1002/14651858.CD003676. PMC 6532671. PMID 12076499.
- ↑ Autret E, Reboul-Marty J, Henry-Launois B, Laborde C, Courcier S, Goehrs JM, Languillat G, Launois R (1997). "Evaluation of ibuprofen versus aspirin and paracetamol on efficacy and comfort in children with fever". European Journal of Clinical Pharmacology. 51 (5): 367–71. doi:10.1007/s002280050215. PMID 9049576. S2CID 27519225.
- ↑ "2.9 Antiplatelet drugs". British National Formulary for Children. British Medical Association and Royal Pharmaceutical Society of Great Britain. 2007. p. 151.
- 1 2 Wong T, Stang AS, Ganshorn H, Hartling L, Maconochie IK, Thomsen AM, Johnson DW (October 2013). "Combined and alternating paracetamol and ibuprofen therapy for febrile children". The Cochrane Database of Systematic Reviews (10): CD009572. doi:10.1002/14651858.CD009572.pub2. PMC 6532735. PMID 24174375.
- ↑ King D (August 2013). "Question 2: does a failure to respond to antipyretics predict serious illness in children with a fever?". Archives of Disease in Childhood. 98 (8): 644–46. doi:10.1136/archdischild-2013-304497. PMID 23846358. S2CID 32438262.
- ↑ Ludwig J, McWhinnie H (May 2019). "Antipyretic drugs in patients with fever and infection: literature review". British Journal of Nursing. 28 (10): 610–618. doi:10.12968/bjon.2019.28.10.610. PMID 31116598.
- ↑ Eyers S, Weatherall M, Shirtcliffe P, Perrin K, Beasley R (October 2010). "The effect on mortality of antipyretics in the treatment of influenza infection: systematic review and meta-analysis". Journal of the Royal Society of Medicine. 103 (10): 403–11. doi:10.1258/jrsm.2010.090441. PMC 2951171. PMID 20929891.
- ↑ Nassisi D, Oishi ML (January 2012). "Evidence-based guidelines for evaluation and antimicrobial therapy for common emergency department infections". Emergency Medicine Practice. 14 (1): 1–28, quiz 28–29. PMID 22292348.
- 1 2 Sajadi MM, Bonabi R, Sajadi MR, Mackowiak PA (October 2012). "Akhawayni and the first fever curve". Clinical Infectious Diseases. 55 (7): 976–80. doi:10.1093/cid/cis596. PMID 22820543.
- 1 2 3 4 Crocetti M, Moghbeli N, Serwint J (June 2001). "Fever Phobia Revisited: Have Parental Misconceptions About Fever Changed in 20 Years?". Pediatrics. 107 (6): 1241–1246. doi:10.1542/peds.107.6.1241. PMID 11389237. Archived from the original on 21 May 2020. Retrieved 31 March 2020.
- ↑ Klass, Perri (10 January 2011). "Lifting a Veil of Fear to See a Few Benefits of Fever". The New York Times. Archived from the original on 29 September 2015.
- ↑ "Equusite Vital Signs". equusite.com. Archived from the original on 26 March 2010. Retrieved 22 March 2010.
- ↑ Schmidt-Nielsen K, Schmidt-Nielsen B, Jarnum SA, Houpt TR (January 1957). "Body temperature of the camel and its relation to water economy". The American Journal of Physiology. 188 (1): 103–12. doi:10.1152/ajplegacy.1956.188.1.103. PMID 13402948.
- 1 2 Thomas MB, Blanford S (July 2003). "Thermal biology in insect-parasite interactions". Trends in Ecology & Evolution. 18 (7): 344–50. doi:10.1016/S0169-5347(03)00069-7.
Further reading
- Rhoades R, Pflanzer RG (1996). "Chapter 27: Regulation of Body Temperature (Clinical Focus: Pathogenesis of Fever)". Human Physiology (3rd ed.). Philadelphia, PA: Saunders College. ISBN 9780030051593. Retrieved 2 April 2020.
{{cite book}}: CS1 maint: uses authors parameter (link)
External links
| Classification | |
|---|---|
| External resources |
- Fever and Taking Your Child's Temperature Archived 13 December 2015 at the Wayback Machine
- US National Institute of Health factsheet Archived 11 May 2009 at the Wayback Machine
- Drugs most commonly associated with the adverse event Pyrexia (Fever) as reported the FDA Archived 9 March 2012 at the Wayback Machine
- "Fever". MedlinePlus. U.S. National Library of Medicine. Archived from the original on 30 April 2016. Retrieved 29 July 2020.