Congenital clasped thumb
| Congenital clasped thumb | |
|---|---|
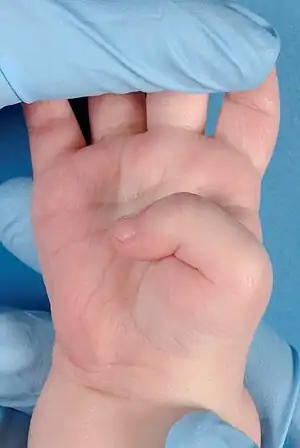 | |
| Congenital clasped thumb |
Infant’s persistent thumb-clutched hand,[1] flexion-adduction deformity of the thumb,[2] pollex varus,[3] thumb in the hand deformity.[4]
Congenital clasped thumb describes an anomaly which is characterized by a fixed thumb into the palm at the metacarpophalangeal joint in one or both hands.[5] The incidence and genetic background are unknown. A study of Weckesser et al. showed that boys are twice as often affected with congenital clasped thumb compared to girls. The anomaly is in most cases bilateral (present in both hands).[5] A congenital clasped thumb can be an isolated anomaly, but can also be attributed to several syndromes.
Causes
The thumb contains five groups of muscle and/or tendons:
- Extensor tendons (to stretch the thumb)
- Flexor muscles/tendons (to bend the thumb)
- Abductor muscles/tendons (to move the thumb outwards)
- Adductor muscle (to move the thumb inwards)
- Opposing muscles (to move the thumb opposite the small finger)
In order for the thumb to maintain a normal position, a strict balance between these groups is required. Weak or absent extensors and/or abductors (the extensor pollicis brevis tendon, the extensor pollicis longus tendon or, rarely, the abductor pollicis longus tendon), can cause a disbalance, leading to an abnormal position of the thumb: congenital clasped thumb. There is also the possibility that two tendons are affected simultaneously.
The following tendon deviations can induce congenital clasped thumb:
- The flexor tendons are too short (the thumb is drawn into the palm)
- The abductor tendons are hypoplastic or absent
- The extensor tendons are hypoplastic or absent
Furthermore, a tight thumb web space (the area between thumb and index finger) can contribute to congenital clasped thumb. The thumb cannot be properly abducted (moved outwards), if the web space is too tight.
To summarize, the causes of congenital clasped thumbs may vary between patients and can sometimes be a combination of the preceding components. Treatment should be tailored to all occurring components in order to achieve good results.
Diagnosis
Diagnosing the congenital clasped thumb is difficult in the first three to four months of life, as it is normal when the thumb is clutched into the palm in these first months.[6] Diagnoses that cause the same flexion or adduction abnormalities of the thumb are:
- Congenital clasped thumb
- Congenital Trigger thumb (flexion of the interphalangeal joint) - Trigger finger
- Spasticity: overstimulation of muscles
Syndrome associated flexion-adduction of the thumb:
- Freeman–Sheldon syndrome (a congenital, heritable affection of the face, the hands, the feet and some joints)[5][7]
- Distal arthrogryposis[5][8]
- MASA syndrome[5][9]
- X-linked hydrocephalus[5][10]
- Adducted thumb syndrome[5]
- Waardenburg syndrome[5]
- Whistling face syndrome (Freeman–Sheldon syndrome)
- Digitotalar dysmorphism [11]
- Multiple pterygium syndrome
Classification
There are a few different classifications conceived to categorize the spectrum of variety of congenital clasped thumb. In literature, X classifications have been described for clasped thumb. The two most relevant of the existing classifications, to our opinion, are the classifications of McCarrol[12] and Tjuyuguchi et al.[13]
The most global format is the classification of McCarrol, which divides the congenital clasped thumbs into two groups. Group I includes the supple clasped thumb, when the thumb is only passively correctable. While complex clasped thumbs, thumbs which cannot be moved neither passively or actively, belong to group II.
Tjuyuguchi et al. designed a classification existing of three groups:
- Group I: The supple clasped thumb, where the thumb is passively abductable and extendable against the resistance of thumb flexors, without other digital anomalies.
- Group II: The clasped thumb with hand contractures, where the thumb is not passively extendable and abductable, with or without other digital anomalies.
- Group III: The clasped thumb which is associated with arthrogryposis.
Treatment
Treatment of congenital clasped thumb includes two types of therapy: conservative and surgical.
Conservative treatment
Treatment of all categories of congenital clasped thumbs should start with either serial plaster casting or wearing a static or dynamic splint for a period of six months,[5] while massaging the hand. Extension by splinting shows reduction of the flexion contracture. To gain optimal results, it is important to start this treatment before the age of six months. The result of this therapy is better in less severe deformities.[14] In most uncomplicated cases, a satisfactory result can be gained when splint therapy starts before the age of six months.[15] Splinting should be tried for at least three months and possibly for as long as six months or longer. If the result of splint therapy stagnates, surgery treatment is indicated.[16]
Surgical treatment
Surgical treatment should be considered in patients who have not been treated at younger age or when conservative therapy fails. Surgery is recommended during the age of three to five years.
Techniques
- Release the thumb web space: it is possible to widen and deepen the area between the thumb and the index finger when it is too tight. To achieve this, a transposition flap or four-flap or five-flap Z-plasty can be used.
- Tendon transfer:[5] a technique usually considered for young children, in which tendons of index finger or little finger are used to make an adequate new extensor tendon for the thumb.
Other procedures
- Arthrodesis: fixing the metacarpophalangeal joint of the thumb in a more extension position.
References
- ↑ White JW, Jensen WE. The infant’s persistent thumb-clutched hand. J Bone Joint Surg. 1952;34A:680-8
- ↑ Broadbent TR, Woolf RM. Flexion-adduction deformity of the thumb – congenital clsped thumb. Plast Reconstr Surg. 1964;34:612-6
- ↑ Miller JM, Pollex varus. A report of two cases. Univ Hosp Bull (Ann Arbor. 1944;10:10-1)
- ↑ Matev I. Surgical treatment of spastc ‘thumb in palm’ deformity. J Bone Joint Surg. 1963;45B:703-8
- 1 2 3 4 5 6 7 8 9 10 11 Miura T: Flexion deformities of the thumb. In Buck-Gramcko D (ed): Congenital Malformations of the Hand and Forearm. London, Churchill Livingstone, 1998, pp 425-429.
- ↑ Gesell A. An atlas of infant behavior. New Haven: Yale University Press; 1934:243-9
- ↑ McCarrol HR, Manske PR. The windblown hand: correction of the complex clasped thumb deformity. Hand Clin. 1992;8:147-59
- ↑ Kanof A, Aronson SM, Volk BW. Arthro gryposis: a clinical and pathological study of three cases. Pediatrics. 1956;17:532-40
- ↑ Bianchine JW, lewis RC Jr. The MASA syndrome; a new heritable mental retardation syndrome. Clin Genet. 1974;5:298-306
- ↑ Edwards JH. The syndrome of sex-linked hydrocephalus. Arch Dis Child. 1961;36:486-93.
- ↑ Dhaliwal AS, Myers TL. Digitotalar dysmorphism. Orthop Rev. 1985; 14:97-101
- ↑ McCarroll HR Jr. Congenital flexion deformities of the thumb. Hand Clin. 1985 Aug;1(3):567-75.
- ↑ Tsuyuguchi et al. Congenital clasped thumb: a review of forty-three cases. J Hand Surg Am. 1985 Sep; 10(5):613-8.
- ↑ S-C Lin et al. A simple splinting method for correction of supple congenital clasped thumbs in infants. The Journal of Hand Surgery, British & European Volume, Volume 25, Issue 5, October 1999.
- ↑ Hisam abdel Ghani et al. Characteristics of patients with congenital clasped thumb: a prospective study of 40 patients with the result of treatment. J Child Orthop. 2007 November; 1(%): 313-322.
- ↑ Medina et al. Flexion deformities of the thumb: clasped thumb and trigger thumb. Chirurgie de la main, Dec 2008;27 Suppl 1:S35-9.
- ↑ Ronald Friedman MD et al. The dorsal transposition flap for congenital contractures of the first web space: A 20-year experience. The Journal of Hand Surgery, Volum 22, Issue 4, July 1997.