Episiotomy
| Episiotomy | |
|---|---|
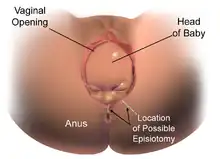
 Medio-lateral episiotomy as baby crowns. | |
| Pronunciation | /əˌpiːziˈɒtəmi, ˌɛpəsaɪˈ-/ |
| Other names | Perineotomy |
| Specialty | obstetrics |
| ICD-9-CM | 73.6 |
| MeSH | D004841 |
| MedlinePlus | 002920 |
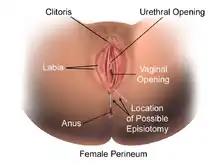
Episiotomy, also known as perineotomy, is a surgical incision of the perineum and the posterior vaginal wall generally done by a midwife or obstetrician. Episiotomy is usually performed during second stage of labor to quickly enlarge the opening for the baby to pass through. The incision, which can be done from the posterior midline of the vulva straight toward the anus or at an angle to the right or left (medio-lateral episiotomy), is performed under local anesthetic (pudendal anesthesia), and is sutured after delivery.
Its routine use is no longer recommended.[1] Despite this, it is one of the most common medical procedures performed on women. In the United States, as of 2012, it was performed in 12% of vaginal births.[1] It is still widely practiced in many parts of the world, including Korea, Japan, Taiwan, China, and Spain.[2][3]
Uses
Vaginal tears can occur during childbirth, most often at the vaginal opening as the baby's head passes through, especially if the baby descends quickly. Episiotomy is done in an effort to prevent against soft-tissue tearing (perineal tear) which may involve the anal sphincter and rectum. Tears can involve the perineal skin or extend to the muscles and the anal sphincter and anus. The midwife or obstetrician may decide to make a surgical cut to the perineum with scissors or a scalpel to make the baby's birth easier and prevent severe tears that can be difficult to repair. The cut is repaired with stitches (sutures). Some childbirth facilities have a policy of routine episiotomy.[4]
Specific reasons to do an episiotomy are unclear.[1] Though indications on the need for episiotomy vary and may even be controversial (see discussion below), where the technique is applied, there are two main variations. Both are depicted in the above image.
- In one variation, the midline episiotomy, the line of incision is central over the anus. This technique bifurcates the perineal body, which is essential for the integrity of the pelvic floor. Precipitous birth can also sever—and more severely sever—the perineal body, leading to long-term complications such as incontinence. Therefore, the oblique technique is often applied (also pictured above).
- In the oblique technique, the perineal body is avoided, cutting only the vagina epithelium, skin, and muscles (transversalius and bulbospongiosus). This technique aids in avoiding trauma to the perineal body by either surgical or traumatic means.
In 2009, a Cochrane meta-analysis based on studies with over 5,000 women concluded that: "Restrictive episiotomy policies appear to have a number of benefits compared to policies based on routine episiotomy. There is less posterior perineal trauma, less suturing and fewer complications, no difference for most pain measures and severe vaginal or perineal trauma, but there was an increased risk of anterior perineal trauma with restrictive episiotomy".[4] The authors were unable to find quality studies that compared mediolateral versus midline episiotomy.[4]
Types
There are four main types of episiotomy:[5]
- Medio-lateral: The incision is made downward and outward from the midpoint of the fourchette either to the right or left. It is directed diagonally in a straight line which runs about 2.5 cm (1 in) away from the anus (midpoint between the anus and the ischial tuberosity).
- Median: The incision commences from the centre of the fourchette and extends on the posterior side along the midline for 2.5 cm (1 in).
- Lateral: The incision starts from about 1 cm (0.4 in) away from the centre of the fourchette and extends laterally. Drawbacks include the chance of injury to the Bartholin's duct, therefore some practitioners have strongly discouraged lateral incisions.
- J-shaped: The incision begins in the centre of the fourchette and is directed posteriorly along the midline for about 1.5 centimetres (0.59 in) and then directed downwards and outwards along the 5 or 7 o'clock position to avoid the internal and external anal sphincter. This procedure is also not widely practised.
Controversy
Traditionally, physicians have used episiotomies in an effort to deflect the cut in the perineal skin away from the anal sphincter muscle, as control over stool (faeces) is an important function of the anal sphincter, i.e. lessen perineal trauma, minimize postpartum pelvic floor dysfunction, and as muscles have a good blood supply, by avoiding damaging the anal sphincter muscle, reduce the loss of blood during delivery, and protect against neonatal trauma. While episiotomy is employed to obviate issues such as post-partum pain, incontinence, and sexual dysfunction, some studies suggest that episiotomy surgery itself can cause all of these problems.[6] Research has shown that natural tears typically are less severe (although this is perhaps not surprising since an episiotomy is designed for when natural tearing will cause significant risks or trauma). Slow delivery of the head in between contractions will result in the least perineal damage.[7] Studies in 2010 based on interviews with postpartum women have concluded that limiting perineal trauma during birth is conducive to continued sexual function after birth. At least one study has recommended that routine episiotomy be abandoned for this reason.[8]
In various countries, routine episiotomy has been accepted medical practice for many years. Since about the 1960s, routine episiotomies have been rapidly losing popularity among obstetricians and midwives in almost all countries in Europe, Australia, Canada, and the United States. A nationwide U.S. population study suggested that 31% of women having babies in U.S. hospitals received episiotomies in 1997, compared with 56% in 1979.[9] In Latin America it remains popular, and is performed in 90% of hospital births.[10]
Discussion
Having an episiotomy may increase perineal pain during postpartum recovery, resulting in trouble defecating, particularly in midline episiotomies.[11] In addition, it may complicate sexual intercourse by making it painful and replacing erectile tissues in the vulva with scar tissue.[12]
In cases where an episiotomy is indicated, a mediolateral incision may be preferable to a median (midline) incision, as the latter is associated with a higher risk of injury to the anal sphincter and the rectum.[13] Damage to the anal sphincter caused by episiotomy can result in fecal incontinence (loss of control over defecation). Conversely, one of the reasons episiotomy is performed is to prevent tearing of the anal sphincter, which is also associated with faecal incontinence.
Impacts on sexual intercourse
Some midwives compare routine episiotomy to female genital mutilation.[14] One study found that women who underwent episiotomy reported more painful intercourse and insufficient lubrication 12–18 months after birth but did not find any problems with orgasm or arousal.[15]
Pain management
Perineal pain after episiotomy has immediate and long-term negative effects for women and their babies. These effects can interfere with breastfeeding and the care of the infant.[16] The pain from injection sites and episiotomy is managed by the frequent assessment of the report of pain from the mother. Pain can come from possible lacerations, incisions, uterine contractions and sore nipples. Appropriate medications are usually administered. Nonpharmacologic interventions can also be used: a warm sitz bath increases blood flow to the area, decreases local discomfort, and promotes healing.[17] Routine episiotomies have not been found to reduce the level of pain after the birth.[18]
See also
References
- 1 2 3 American College of Obstetricians Gynecologists' Committee on Practice Bulletins—Obstetrics (July 2016). "Practice Bulletin No. 165: Prevention and Management of Obstetric Lacerations at Vaginal Delivery". Obstetrics and Gynecology. 128 (1): e1–e15. doi:10.1097/AOG.0000000000001523. PMID 27333357. S2CID 20952144.
- ↑ Chang,S-R; Chen,K-H; Lin,H-H; Chao,Y-M Y; Lai,Y-H (April 2011). "Comparison of the effects of episiotomy and no episiotomy on pain, urinary incontinence, and sexual function 3 months postpartum: A prospective follow-up study". International Journal of Nursing Studies. 48 (4): 409–418. doi:10.1016/j.ijnurstu.2010.07.017. PMID 20800840.
- ↑ Graham,I.D.; Carroli,G.; Davies,C.; Medves,J.M. (August 2005). "Episiotomy Rates Around the World: An Update". Birth. 32 (3): 219–223. doi:10.1111/j.0730-7659.2005.00373.x. PMID 16128977.
- 1 2 3 Carroli, G, Mignini, L. "Episiotomy for vaginal birth". Cochrane Database Syst Rev. 2009 Jan 21; (1): CD000081.
- ↑ D. C. Dutta, Textbook of Obstetrics, 7th edition, 2011.
- ↑ Thacker, S. B.; Banta, H. D. (1983). "Benefits and risks of episiotomy: An interpretative review of the English language literature, 1860-1980". Obstet Gynecol Surv. 38 (6): 322–38. doi:10.1097/00006254-198306000-00003. PMID 6346168.
- ↑ Albers L. L.; et al. (2006). "Factors Related to Genital Tract Trauma in Normal Spontaneous Vaginal Births". Birth. 33 (2): 94–100. doi:10.1111/j.0730-7659.2006.00085.x. PMID 16732773.
- ↑ Rathfisch, G. et al. "Effects of perineal trauma on postpartum sexual function." Journal of Advanced Nursing. 2010 Aug 23.
- ↑ Weber, A. M.; Meyn, L. (2002). "Episiotomy use in the United States, 1979-1997". Obstetrics & Gynecology. 100 (6): 1177–82. doi:10.1016/S0029-7844(02)02449-3. PMID 12468160. S2CID 28134959.
- ↑ Althabe, F.; Belizán, J. M.; Bergel, E. (2002). "Episiotomy rates in primiparous women in Latin America: hospital-based descriptive study". BMJ. 324 (7343): 945–6. doi:10.1136/bmj.324.7343.945. PMC 102327. PMID 11964339.
- ↑ Signorello, L. B.; Harlow, B. L.; Chekos, A. K.; Repke, J. T. (2000). "Midline episiotomy and anal incontinence: retrospective cohort study". BMJ. 320 (7227): 86–90. doi:10.1136/bmj.320.7227.86. PMC 27253. PMID 10625261.
- ↑ "Total Health For Women Painful Intercourse". mothernature.com. Archived from the original on 15 June 2006. Retrieved 6 June 2006.
- ↑ American College of Obstetricians-Gynecologists (2006). "ACOG Practice Bulletin. Episiotomy. Clinical Management Guidelines for Obstetrician-Gynecologists. Number 71, April 2006" (PDF). Obstetrics & Gynecology. 107 (4): 956–62. doi:10.1097/00006250-200604000-00049. Retrieved 16 January 2012. Abstract.
- ↑ Joan Cameron; Karen Rawlings-Anderson (1 March 2001). "Female circumcision and episiotomy: both mutilation?". British Journal of Midwifery. 9 (3): 137–142. doi:10.12968/bjom.2001.9.3.7997. Retrieved 16 January 2012.
- ↑ Hanna Ejegård; Elsa Lena Ryding; Berit Sjögren (17 January 2008). "Sexuality after Delivery with Episiotomy: A Long-Term Follow-Up". Gynecologic and Obstetric Investigation. 66 (1): 1–7. doi:10.1159/000113464. PMID 18204265. S2CID 25348363.
- ↑ Shepherd, Emily; Grivell, Rosalie M. (24 July 2020). "Aspirin (single dose) for perineal pain in the early postpartum period". The Cochrane Database of Systematic Reviews. 2020 (7): CD012129. doi:10.1002/14651858.CD012129.pub3. ISSN 1469-493X. PMC 7388929. PMID 32702783.
- ↑ Joyce, Hasegawa; Leventhal, Lucila (1 March 2009). "Pharmacological and non pharmacological treatment for relief of perineal pain after vaginal delivery". Einstein. 7.
- ↑ Jiang, H; Qian, X; Carroli, G; Garner, P (8 February 2017). "Selective versus routine use of episiotomy for vaginal birth". The Cochrane Database of Systematic Reviews. 2017 (2): CD000081. doi:10.1002/14651858.CD000081.pub3. PMC 5449575. PMID 28176333.
External links
- Episiotomy, Merck Manual Professional Edition
- Stages of Labor, Merck Manual Professional Edition
- What I Don’t Tell My Students About ‘The Husband Stitch’, Electricliterature.com