Fixation disparity
Fixation disparity is a tendency of the eyes to drift in the direction of the heterophoria. While the heterophoria refers to a fusion-free vergence state, the fixation disparity refers to a small misalignment of the visual axes when both eyes are open in an observer with normal fusion and binocular vision.[1] The misalignment may be vertical, horizontal or both. The misalignment (a few minutes of arc) is much smaller than that of strabismus. While strabismus prevents binocular vision, fixation disparity keeps binocular vision, however it may reduce a patient's level of stereopsis. A patient may or may not have fixation disparity and a patient may have a different fixation disparity at distance than near. Observers with a fixation disparity are more likely to report eye strain in demanding visual tasks; therefore, tests of fixation disparity belong to the diagnostic tools used by eye care professionals:[2][3][4][5][6] remediation includes vision therapy, prism eye glasses, or visual ergonomics at the workplace.
Optimal binocular vision
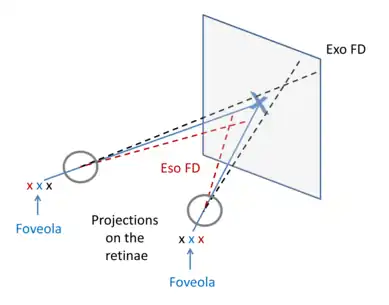
In Fig. 1, the blue lines and characters illustrate the situation of optimal binocular vision: the extra-ocular muscles adjust the vergence angle between the two visual axes so that the fixation target X is projected in each eye onto the centre of the fovea, i.e. the location on the retina with the highest spatial resolution. The fixation point is projected in the two eyes onto retinal points that correspond to the same visual direction in space so that single vision is provided. This means that the visual axes intersect at the fixation target X. On the level of the visual cortex there is a perfect spatial overlap, i.e. the binocular disparity is zero and best binocular summation is possible. Such an optimal state occurs only in a minority of observers.[1]
Sub-optimal condition of fixation disparity (FD)
Most observers have a so-called “normal” binocular vision in the sense that they are able to view stereoscopically, but still many of these observers can have a sub-optimal condition in terms of a fixation disparity (FD). The vergence angle is slightly misadjusted so that the fixation point is projected slightly apart from the centre of the fovea. The visual axes may intersect in front (red lines) of the target plane, or behind (black line); these states of over- or under-convergence are referred to as eso- or exo FD, respectively (see Fig.1). In the visual cortex, a binocular disparity between the two retinal images remains. If this disparity is small enough, sensory and neural mechanisms in binocular neurons still attribute the same visual direction to these slightly disparate images and single vision is provided. This mechanism of sensory fusion with normal retinal correspondence operates within a certain limit of disparity, referred to as Panum’s area. If the disparity is larger, the normal Panum’s fusion mechanism is not sufficient; rather, in order to achieve fusion, a neural remapping of retinal correspondence can occur, which - however - prevents a high quality stereo vision.[7]
Thus, in order to achieve single vision, two physiological mechanisms operate hand in hand:[8][7]
1.) The motor mechanism of the extra-ocular eye muscles adjusts the vergence angle as precisely as possible for the individual, but a small vergence error may remain.
2.) Sensory (neural) mechanisms provide single vision by means of fusion within normal Panum’s area or remapping of retinal correspondence (extended Panum’s areas).
Methods for measuring fixation disparity
The methods can be explained based on the study of Hofmann and Bielschowsky[9] in 1900, who applied a modified Maddox wing: the right eye is presented with a horizontal scale and the left eye with an arrow. The observer perceives that the arrow points onto one of the numbers on the scale which indicates a possible vergence mis-adjustment. The Maddox wing, however, does not test binocular vision since no fusion target is present. For testing the state of binocular vision, Hofmann and Bielschowsky[9] included an additional fusion stimulus to the two eyes and still found a perceived offset of scale and arrow; they referred to this offset as “Disparitätsrest” (in German), which means “residual disparity”. Later, Ogle[10][11] coined the term "fixation disparity".
More generally, this traditional vergence test is a subjective test in the sense that the observer reports his/her perception of the relative position of two test targets that are presented separately to the two eyes, i.e. dichoptic targets. This test relies on the assumption that retinal points are associated with visual directions in space. If physically aligned dichoptic targets appear subjectively aligned, they are projected onto corresponding retinal points and the visual axes intersect at the test target; thus, the vergence angle agrees with the viewing distance. In case of a deviating vergence state, the dichoptic targets need to have a certain physical horizontal offset in order to be perceived in line. These subjective measures agree with objective recordings with eye trackers,[12] if no fusion stimulus is involved.
For measuring subjective fixation disparity, researchers as Ogle,[11] Sheedy and Saladin,[13] Mallett,[14] Wesson[15] constructed test instrumentation including fusion targets and dichoptic targets using cross-polarized filters in front of the eyes; some of these devices are commercially available. If the dichoptic targets are presented to the observer in physical alignment, the angular amount (in the unit minutes of arc) of subjective fixation disparity is indicated by the perceived misalignment of the two dichoptic targets. This can be compensated by the patient's individual amount of a prism eye glass (in the unit prism dioptre) so that the patient perceives alignment. The latter prism needed to reduce the fixation disparity to zero is referred to as aligning prism[4] (earlier called associated phoria). Instrumentations as the Disparometer, the Mallett-unit, or the Wesson Card differ in the type of fusion target: some use small central fixation letters, others use more peripheral fusion targets. The instruments can be swung through 90° to measure any vertical fixation disparity. The test devices can also be used to detect suppression.
The above studies of subjective fixation disparity assumed - partly implicitly - that the dichoptic targets would indicate the vergence misalignment of the visual axes muscles, i.e. the vergence error, as it can be measured with eye tracking methods. This seemed to be justified by the first objective recording of fixation disparity made in 1960 by Hebbard[16] with an eye tracking method based on small mirrors fixed onto contact lenses: he found agreement between the two measures (in the one observer tested). However, subsequent studies[17][18][19][8][20] found that the objective recordings with eye trackers can differ substantially from the subjective test results with dichoptic targets: with central fusion targets and closely adjacent dichoptic targets, the subjective measure can be about 10 times smaller than the objective measure. When the dichoptic targets are gradually shifted by some degree away from the fusion target, then the two measures become more and more similar.[8] This was interpreted as a change in retinal correspondence in the sense that the visual direction associated with the dichoptic targets is modified in the vicinity of the fusion target.

Definition of objective and subjective fixation disparity
Given the discrepancy between objective measures with eye trackers and subjective measures with dichoptic targets, different definitions should be applied (see Fig. 2):[21][22]
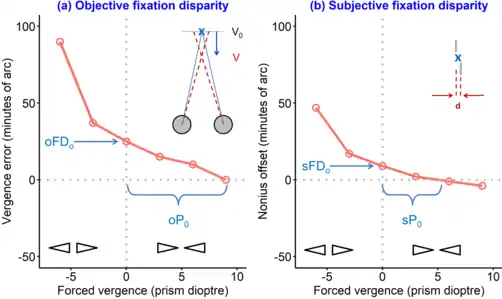
· Objective fixation disparity (oFD) is defined as the oculomotor vergence error that can only be measured with eye trackers, i.e. oFD = V – V0 . This is the difference between the vergence angle in binocular vision (V, red line in Fig. 2a) and the optimal vergence state when a target is projected in each eye onto the center of the foveola (V0=2 arc tan ((pd)/2)/D), blue line in Fig. 2a). V0 is estimated from the monocular calibration[23] of the eye tracker, i.e. the left eye is covered when the right eye calibration is made and vice versa; this procedure assumes that in monocular vision a target is projected onto the centre of the foveola.
· Subjective fixation disparity (sFD) is defined as the angular amount of the offset between dichoptic targets that need to be adjusted to a certain offset d so that the observer perceives the dichoptic targets in alignment (see the pair of nonius lines in Fig. 2b). Note that this definition of sFD = arctan (d/D) does not refer to the current vergence angle. The resulting subjective fixation disparity may depend on the spatial arrangement of dichoptic targets and fusion targets.
The discrepancy between oFD and sFD is shown in Fig. 2 in that the disparity ∆ between the two visual axes is typically larger than angular amount of the nonius offset d.
Physiological properties of both types of fixation disparity
A fixation disparity is not constant within a certain observer, but can vary depending on the viewing conditions. If test prisms with increasing amount are placed in front of the observer’s eyes, the fixation disparity changes in the eso direction with base-in prisms and in the exo direction with base-out prisms (Fig. 3). These prisms force the eyes to change the vergence angle while the viewing distance remains unchanged. Prism-induced fixation disparity curves (prism FD-curves) can be characterized by the following parameters:[8][13][11]
- the y-intercept refers to the naturally occurring fixation disparity without a prism (FD0)
- the x-intercept gives the amount of a prism (P0) that compensates a naturally occurring fixation disparity. This x-intercept is also referred to as aligning prism or – in earlier times – as associated phoria when the subjective nonius method was used (sP0)
- the slope of the curve near zero prism load
These prism FD-curves have widely been used for subjective fixation disparity [13][11] and the clinical implications are described below. Only more recently, subjective and objective prism FD-curves have been measured simultaneously:[17][8] In principle both measures have a similar form of these curves, but they can differ quantitatively; typically, oFD is much larger than sFD. A comparison of subjective versus objective measures revealed a significant correlation (about r = 0.5 – 0.7) for the y-intercept (sFD0 versus oFD0), but not for the slope.[24]
In natural vision without prisms, the vergence state varies as a function of the viewing distance of the target: the subjective fixation disparity may shift towards more exo states from far-vision to near-vision.[25] The effect of proximity is different for objective and subjective fixation disparity.[26]
During reading of text material, the objective fixation disparity can be measured with eye trackers in the moments of fixation.[27][28] This reading fixation disparity has the following properties:
- Fusion is maintained despite a fixation disparity during a reading fixation[29]
- The reading fixation disparity reaches a minimum at a certain moment in time during the fixation[30]
- The reading fixation disparity shifts to more eso conditions in the course of reading a line from left to right[31]
- Blurring the text makes the reading fixation disparity more exo[32]
- The reading fixation disparity is smaller when the text characters have a more pronounced periodic spatial structure[33]
Clinical diagnostic criteria
Fixation disparity can differ considerably between observers with normal binocular vision. The following conditions of subjective fixation disparity tend to be more prevalent in observers with eye strain.
Near-vision subjective fixation disparity (sFD0) tends to be larger in the exo direction and the aligning prisms (sP0) tends to be more base-in, suggesting that the eyes tend to under-converge.[34][35][36][37] Most of these studies used the Mallett-unit, which consists of a small central fixation letter X surrounded by two letters O, one on each side of X.[38]
The prism FD-curve (measured subjectively in near vision) tends to have a steeper slope (see Fig. 3b), meaning that the binocular system is not able to reach a small fixation disparity when vergence is forced by prisms in the base-in and base-out direction.[13] This evidence came predominantly from studies with the Disparometer, an instrument that allows presenting dichoptic nonius lines with different amounts of offset to find a particular physical offset that leads to perceived alignment. These nonius lines are presented within a circular contour of 1.5 deg diameter that is viewed binocularly.[13]
The proximity FD-curve (measured subjectively as a function of viewing distance) tends to be steeper, meaning that the binocular system is not able to keep the fixation disparity small, if a target is shifted closer in the range of about 100 to 20 cm. This evidence came from studies using a computer-controlled test stimulus including a central fusion stimulus.[39][6]
All the above measures in studies of eye strain refer to the subjective fixation disparity, because the procedure with dichoptic targets is technically easy and therefore can conveniently be applied in the clinical setting with some commercial test devices. Some of the cited studies found, that measures of subjective fixation disparity are a better diagnostic criterion for eye strain than the heterophoria, i.e. the vergence state without a fusion stimulus.[34][35][36][13] The technically more complex eye tracking technology for measuring objective fixation disparity has not yet been investigated in relation to eye strain.
Remediation of fixation disparity in observers with eye strain
Given that an observer has a certain fixation disparity and suffers from eye strain, one may consider some of the following ways of remediation.
Eye glasses with an included prism power is the optical method to reduce a fixation disparity. Different procedures have been proposed to determine the required amount of prism for the individual. Based on prism-FD curves (Fig. 3b), one can find the aligning prism sP0 that nullifies the naturally prevailing fixation disparity sFD0. This test procedure is typically made in near vision of 40 cm, e.g. with the Mallett-unit, the Disparometer, or the Wesson card (see above). Experimental evidence for the effectiveness of the aligning prism came from a study of reading speed and corresponding preferences of prism eye glasses.[40] A different approach was suggested by H.-J. Haase [5][41] who proposed a set of dichoptic target tests with both central and more peripheral fusion targets and additional stereo tests that were predominantly used in far vision. Such prisms alleviated eye strain and remained stable over time.[42][43] The usefulness of prism eye glasses has been criticized since the initial fixation disparity may reappear again after some time due to the adaptability of the vergence system.[44] One may consider, however, that vergence tends to be less adaptive in observers with eye strain so that in these observers the prisms may permanently reduce a naturally prevailing fixation disparity.[45][46]
Visual ergonomics of a computer workstation may take into account the individual proximity FD-curve:[6][39] individuals with a larger exo fixation disparity at near may prefer a longer viewing distance where the fixation disparity is smaller.
Visual vergence training (also referred to as orthoptic exercises or vision therapy) aims to improve the physiological condition of binocular vision with eye movement exercises, including e.g. frequent dynamic vergence changes between near and far vision. The effectiveness has been confirmed both in terms of alleviation of visual symptoms and in better physiological conditions, e.g. the prism-FD curves became more flat.[47] The physiological effect of visual vergence training has also been confirmed for other vergence functions.[48][49][50]
See also
- Diplopia
- Eye examination
- Heterophoria
- Ocular dominance
- Vision therapy
- Binocular vision
- Vergence
- Eye Tracking
References
- 1 2 Howard, Ian P. (2012). Perceiving in DepthVolume 1 Basic Mechanisms. Oxford University Press. doi:10.1093/acprof:oso/9780199764143.001.0001. ISBN 978-0-19-976414-3.
- ↑ Eskridge, JB; Amos, JF; Bartlett, JD (1991). Clinical procedures in Optometry. New York: Lippincott Co.
- ↑ Scheiman, Mitchell (4 October 2019). Clinical management of binocular vision : heterophoric, accommodative, and eye movement disorders. Wick, Bruce (Fifth ed.). Philadelphia. ISBN 978-1-4963-9973-1. OCLC 1098229972.
- 1 2 Evans, Bruce J. W. (2007). Pickwell's binocular vision anomalies. Pickwell, David. (5th ed.). Edinburgh: Elsevier Butterworth Heinemann. ISBN 978-0-7020-3925-6. OCLC 785829294.
- 1 2 Schroth, Volkhard. (2012). Binocular correction : aligning prisms according to the Haase approach (2. ed.). [Heemskerk]: Zijdar Books. ISBN 978-90-78376-09-5. OCLC 835292953.
- 1 2 3 Jaschinski, Wolfgang (2002). "The Proximity-Fixation-Disparity Curve and the Preferred Viewing Distance at a Visual Display as an Indicator of Near Vision Fatigue". Optometry and Vision Science. 79 (3): 158–169. doi:10.1097/00006324-200203000-00010. ISSN 1040-5488. PMID 11913842. S2CID 2793623.
- 1 2 Wick, Bruce (1991). "Stability of Retinal Correspondence in Normal Binocular Vision". Optometry and Vision Science. 68 (2): 146–158. doi:10.1097/00006324-199102000-00011. ISSN 1040-5488. PMID 2027655.
- 1 2 3 4 5 Fogt, Nick; Jones, Ronald (1998). "The effect of forced vergence on retinal correspondence". Vision Research. 38 (18): 2711–2719. doi:10.1016/s0042-6989(97)00448-3. ISSN 0042-6989. PMID 9775320.
- 1 2 Hofmann, F. B.; Bielschowsky, A. (1900). "Ueber die der Willkür entzogenen Fusionsbewegungen der Augen". Pflüger, Archiv für die Gesammte Physiologie des Menschen und der Thiere. 80 (1–2): 1–40. doi:10.1007/bf01661926. ISSN 0031-6768. S2CID 26624365.
- ↑ Ogle, KN (1950). Researches in Binocular Vision. Philadelphia: Sauders.
- 1 2 3 4 Ogle, Kenneth N. (1967). Oculomotor imbalance in binocular vision and fixation disparity. Lea & Febiger. OCLC 588191420.
- ↑ Han, Sang J.; Guo, Yi; Granger-Donetti, Bérangère; Vicci, Vincent R.; Alvarez, Tara L. (2010). "Quantification of heterophoria and phoria adaptation using an automated objective system compared to clinical methods: Quantification of heterophoria". Ophthalmic and Physiological Optics. 30 (1): 95–107. doi:10.1111/j.1475-1313.2009.00681.x. PMID 19682268. S2CID 205636232.
- 1 2 3 4 5 6 Sheedy JE, Saladin JJ. Validity of diagnostic criteria and case analysis in binocular vision disorders. In: Schor CM, Ciuffreda KJ, editors. Vergence Eye Movements: Basic and Clinical Aspects. Boston: Butterworths; 1983. p. 517–540.
- ↑ Mallett RJF. The investigation of heterophoria at near and a new fixation disparity technique. Optician. 1974; 148: 547–551.
- ↑ Wesson M.D., Koening R.A., A new method for direct measurement of fixation disparity, Southern Journal of Optometry 1, 1983, pp. 48–52
- ↑ Hebbard, Frederick W. (1962). "Comparison of Subjective and Objective Measurements of Fixation Disparity*†". Journal of the Optical Society of America. 52 (6): 706. doi:10.1364/josa.52.000706. ISSN 0030-3941.
- 1 2 Remole, Arnulf; Code, Stephen M.; Matyas, Cynthia E.; McLeod, Murray A.; White, David J. (1986). "Objective Measurement of Binocular Fixation Misalignment". Optometry and Vision Science. 63 (8): 631–638. doi:10.1097/00006324-198608000-00006. ISSN 1040-5488. PMID 3766692.
- ↑ Kertesz, Andrew E.; Lee, Hyo J. (1987). "Comparison of Simultaneously Obtained Objective and Subjective Measurements of Fixation Disparity". Optometry and Vision Science. 64 (10): 734–738. doi:10.1097/00006324-198710000-00004. ISSN 1040-5488. PMID 3688176. S2CID 27840178.
- ↑ Simonsz, H. J.; Bour, L. J. (1991). "Covering one eye in fixation-disparity measurement causes slight movement of fellow eye". Documenta Ophthalmologica. 78 (3–4): 141–152. doi:10.1007/bf00165674. hdl:1765/40453. ISSN 0012-4486. PMID 1790734. S2CID 754569.
- ↑ Brautaset, RL; Jennings, JA (2006). "Measurements of objective and subjective fixation disparity with and without a central fusion stimulus". Med Sci Monit. 12 (2): MT1-4. PMID 16449958.
- ↑ Fogt, Nick; Jones, Ronald (1998). "Comparison of fixation disparities obtained by objective and subjective methods". Vision Research. 38 (3): 411–421. doi:10.1016/s0042-6989(97)00142-9. ISSN 0042-6989. PMID 9536364.
- ↑ Schroth, Volkhard; Joos, Roland; Jaschinski, Wolfgang (2015). "Effects of Prism Eyeglasses on Objective and Subjective Fixation Disparity". PLOS ONE. 10 (10): e0138871. Bibcode:2015PLoSO..1038871S. doi:10.1371/journal.pone.0138871. ISSN 1932-6203. PMC 4592239. PMID 26431525.
- ↑ Švede, Aiga; Treija, Elīna; Jaschinski, Wolfgang; Krūmiņa, Gunta (2015). "Monocular Versus Binocular Calibrations in Evaluating Fixation Disparity With a Video-Based Eye-Tracker". Perception. 44 (8–9): 1110–1128. doi:10.1177/0301006615596886. ISSN 0301-0066. PMID 26562925. S2CID 24979268.
- ↑ Jaschinski, Wolfgang (2018). "Individual objective versus subjective fixation disparity as a function of forced vergence". PLOS ONE. 13 (7): e0199958. Bibcode:2018PLoSO..1399958J. doi:10.1371/journal.pone.0199958. ISSN 1932-6203. PMC 6035046. PMID 29980146.
- ↑ Jaschinski, Wolfgang (2001). "Fixation disparity and accommodation for stimuli closer and more distant than oculomotor tonic positions". Vision Research. 41 (7): 923–933. doi:10.1016/s0042-6989(00)00322-9. ISSN 0042-6989. PMID 11248277.
- ↑ Jaschinski, Wolfgang (2017). "Individual Objective and Subjective Fixation Disparity in Near Vision". PLOS ONE. 12 (1): e0170190. Bibcode:2017PLoSO..1270190J. doi:10.1371/journal.pone.0170190. ISSN 1932-6203. PMC 5279731. PMID 28135308.
- ↑ Kirkby, Julie A.; Webster, Lisa A. D.; Blythe, Hazel I.; Liversedge, Simon P. (2008). "Binocular coordination during reading and non-reading tasks". Psychological Bulletin. 134 (5): 742–763. doi:10.1037/a0012979. ISSN 1939-1455. PMID 18729571.
- ↑ Nikolova, Mirela (2017). "Binocular Vision in Reading" (PDF). University of Southampton, UK.
- ↑ Liversedge, Simon P. (2008). "Fixation disparity during reading: Fusion, not suppression". Journal of Eye Movement Research. 2 (3). doi:10.16910/jemr.2.3.5. ISSN 1995-8692.
- ↑ Jainta, Stephanie; Hoormann, Joerg; Kloke, Wilhelm Bernhard; Jaschinski, Wolfgang (2010). "Binocularity during reading fixations: Properties of the minimum fixation disparity". Vision Research. 50 (18): 1775–1785. doi:10.1016/j.visres.2010.05.033. ISSN 0042-6989. PMID 20573592.
- ↑ Jainta, Stephanie; Jaschinski, Wolfgang (2010). ""Trait" and "state" aspects of fixation disparity during reading". Journal of Eye Movement Research. 3 (3). doi:10.16910/jemr.3.3.1. ISSN 1995-8692.
- ↑ Jainta, Stephanie; Dehnert, Anne; Heinrich, Sven P.; Jaschinski, Wolfgang (2011). "Binocular Coordination during Reading of Blurred and Nonblurred Text". Investigative Ophthalmology & Visual Science. 52 (13): 9416–24. doi:10.1167/iovs.11-8237. ISSN 1552-5783. PMID 22058330.
- ↑ Jainta, S.; Jaschinski, W.; Wilkins, A. J. (2010). "Periodic letter strokes within a word affect fixation disparity during reading". Journal of Vision. 10 (13): 2. doi:10.1167/10.13.2. ISSN 1534-7362. PMID 21149306.
- 1 2 Mallett, RJF (1974). "Fixation disparity. Its genesis and relation to aesthenopia". Optician. 148: 547–551.
- 1 2 Yekta, A. A.; Jenkins, T.; Pickwell, D. (1987). "The clinical assessment of binocular vision before and after a working day". Ophthalmic & Physiological Optics: The Journal of the British College of Ophthalmic Opticians (Optometrists). 7 (4): 349–352. doi:10.1111/j.1475-1313.1987.tb00759.x. ISSN 0275-5408. PMID 3454909. S2CID 22944265.
- 1 2 Yekta, A. A.; Pickwell, L. D.; Jenkins, T. C. (1989). "Binocular vision without visual stress". Optometry and Vision Science. 66 (12): 815–817. doi:10.1097/00006324-198912000-00002. ISSN 1040-5488. PMID 2626245. S2CID 40413488.
- ↑ Jenkins, T. C.; Pickwell, L. D.; Yekta, A. A. (1989). "Criteria for decompensation in binocular vision". Ophthalmic & Physiological Optics: The Journal of the British College of Ophthalmic Opticians (Optometrists). 9 (2): 121–125. doi:10.1111/j.1475-1313.1989.tb00830.x. ISSN 0275-5408. PMID 2622646. S2CID 40983322.
- ↑ Karania, Rajula; Evans, Bruce J. W. (2006). "The Mallett Fixation Disparity Test: influence of test instructions and relationship with symptoms". Ophthalmic & Physiological Optics: The Journal of the British College of Ophthalmic Opticians (Optometrists). 26 (5): 507–522. doi:10.1111/j.1475-1313.2006.00385.x. ISSN 0275-5408. PMID 16918777.
- 1 2 Jaschinski, W (1998). "Fixation disparity at different viewing distances and the preferred viewing distance in a laboratory near-vision task". Ophthalmic and Physiological Optics. 18 (1): 30–39. doi:10.1016/s0275-5408(97)00039-2. ISSN 0275-5408. PMID 9666908.
- ↑ O'Leary, Claire I.; Evans, Bruce J. W. (2006). "Double-masked randomised placebo-controlled trial of the effect of prismatic corrections on rate of reading and the relationship with symptoms". Ophthalmic & Physiological Optics: The Journal of the British College of Ophthalmic Opticians (Optometrists). 26 (6): 555–565. doi:10.1111/j.1475-1313.2006.00400.x. ISSN 0275-5408. PMID 17040419. S2CID 22818080.
- ↑ London, Richard; Crelier, Roger S. (2006). "Fixation disparity analysis: sensory and motor approaches". Optometry (St. Louis, Mo.). 77 (12): 590–608. doi:10.1016/j.optm.2006.09.006. ISSN 1529-1839. PMID 17157241.
- ↑ Lie, I.; Opheim, A. (1985). "Long-term acceptance of prisms by heterophorics". Journal of the American Optometric Association. 56 (4): 272–278. ISSN 0003-0244. PMID 3989208.
- ↑ Lie, I.; Opheim, A. (1990). "Long-term stability of prism correction of heterophorics and heterotropics; a 5 year follow-up. Part I: Heterophorics". Journal of the American Optometric Association. 61 (6): 491–498. ISSN 0003-0244. PMID 2370416.
- ↑ Rosenfield, M. (1997). "Tonic vergence and vergence adaptation". Optom Vis Sci. 74 (5): 303–328. doi:10.1097/00006324-199705000-00027. PMID 9219290.
- ↑ Henson, D.B. (1981). "Adaptation to prism-induced heterophoria in subjects with abnormal binocular vision or asthenopia". Am J Optom Physiol Opt. 58 (9): 746–752. doi:10.1097/00006324-198109000-00009. PMID 7294146. S2CID 11276047.
- ↑ Schroth, Volkhard; Joos, Roland; Alshuth, Ewald; Jaschinski, Wolfgang (2019). "Short-term effects of aligning prisms on the objective and subjective fixation disparity in far distance". Journal of Eye Movement Research. 12 (4). doi:10.16910/jemr.12.4.8. ISSN 1995-8692. PMC 7880133. PMID 33828739.
- ↑ Hung, GK; Ciuffreda, KJ; Semmlow, JL (1986). "Static vergence and accommodation: population norms and orthoptics effects". Documenta Ophthalmologica. 62 (2): 165–179. doi:10.1007/BF00229128. PMID 3956367. S2CID 33220787.
- ↑ Talasan, Henry; Scheiman, Mitchell; Li, Xiaobo; Alvarez, Tara L. (2016). "Disparity vergence responses before versus after repetitive vergence therapy in binocularly normal controls". Journal of Vision. 16 (1): 7. doi:10.1167/16.1.7. ISSN 1534-7362. PMC 4743712. PMID 26762276.
- ↑ Daniel, François; Morize, Aurélien; Brémond-Gignac, Dominique; Kapoula, Zoï (2016). "Benefits from Vergence Rehabilitation: Evidence for Improvement of Reading Saccades and Fixations". Frontiers in Integrative Neuroscience. 10: 33. doi:10.3389/fnint.2016.00033. ISSN 1662-5145. PMC 5071378. PMID 27812325.
- ↑ Jainta, Stephanie; Bucci, Maria Pia; Wiener-Vacher, Sylvette; Kapoula, Zoï (2011). "Changes in vergence dynamics due to repetition". Vision Research. 51 (16): 1845–1852. doi:10.1016/j.visres.2011.06.014. ISSN 0042-6989. PMID 21745493.