Functional neurologic disorder
| Functional neurologic disorder | |
|---|---|
| Specialty | Psychiatric |
| Frequency | Lua error in Module:PrevalenceData at line 5: attempt to index field 'wikibase' (a nil value). |
Functional neurologic disorder or functional neurological disorder (FND) is a condition in which patients experience neurological symptoms such as weakness, movement disorders, sensory symptoms and blackouts. As a functional disorder there is by definition no disease process affecting the structure of the body, yet the person experiences symptoms relating to their body function. Symptoms of functional neurological disorders are clinically recognisable, but are not categorically associated with a definable organic disease.[1][2]
The intended contrast is with an organic brain syndrome, where a pathology (disease process) can be identified which affects the body's physiology. Subsets of functional neurological disorders include functional neurological symptom disorder (FNsD), conversion disorder, functional movement disorder and functional seizures. The diagnosis is made based on positive signs and symptoms in the history and examination during consultation of a neurologist . "FND is the second most common diagnosis in neurology clinics after headaches," and has become more prevalent among adolescents and older adults in the wake of the COVID pandemic and lockdowns.[3]
Physiotherapy is particularly helpful for patients with motor symptoms (weakness, gait disorders, movement disorders) and tailored cognitive behavioural therapy has the best evidence in patients with dissociative (non-epileptic) attacks.[4][5]
Signs and symptoms
There are a great number of symptoms experienced by those with a functional neurological disorder. While these symptoms are very real, their origin is complex, since it can be associated with severe psychological trauma (conversion disorder), and idiopathic neurological dysfunction.[6] The core symptoms are those of motor or sensory dysfunction or episodes of altered awareness:[7][8][9][10]
- Limb weakness or paralysis
- Blackouts (also called dissociative or non-epileptic seizures/attacks) – these may look like epileptic seizures or faints
- Movement disorders including tremors, dystonia (spasms), myoclonus (jerky movements)
- Visual symptoms including loss of vision or double vision
- Speech symptoms including dysphonia (whispering speech), slurred or stuttering speech
- Sensory disturbance including hemisensory syndrome (altered sensation down one side of the body)
- Dizziness and balance problems
Associated conditions
Epidemiological studies and meta-analysis have shown higher rates of depression and anxiety in patients with FND compared to the general population, but rates are similar to patients with other neurological disorders such as epilepsy or Parkinson's disease. This is often the case because of years of misdiagnosis and accusations of malingering.[11][12][13][14]
Causes
A systematic review found that stressful life events and childhood neglect were significantly more common in patients with FND than the general population, although many patients (around 70%) report no stressors.[15]
Converging evidence from several studies using different techniques and paradigms has now demonstrated distinctive brain activation patterns associated with functional deficits, unlike those seen in actors simulating similar deficits. [16] The new findings advance current understanding of the mechanisms involved in this disease, and offer the possibility of identifying markers of the condition and patients' prognosis.[17][18]
FND has been reported as a rare occurrence in the period following general anesthesia.[19]
Diagnosis
A diagnosis of a functional neurological disorder is dependent on positive features from the history and examination.[20]
Positive features of functional weakness on examination include Hoover's sign, when there is weakness of hip extension which normalises with contralateral hip flexion.[21] Signs of functional tremor include entrainment and distractibility. The patient with tremor should be asked to copy rhythmical movements with one hand or foot. If the tremor of the other hand entrains to the same rhythm, stops, or if the patient has trouble copying a simple movement this may indicate a functional tremor. Functional dystonia usually presents with an inverted ankle posture or clenched fist.[22] Positive features of dissociative or non-epileptic seizures include prolonged motionless unresponsiveness, long duration episodes (>2minutes) and symptoms of dissociation prior to the attack. These signs can be usefully discussed with patients when the diagnosis is being made.[23][24][25][26]
Patients with functional movement disorders and limb weakness may experience symptom onset triggered by an episode of acute pain, a physical injury or physical trauma. They may also experience symptoms when faced with a psychological stressor, but this isn't the case for most patients. Patients with functional neurological disorders are more likely to have a history of another illness such as irritable bowel syndrome, chronic pelvic pain or fibromyalgia but this cannot be used to make a diagnosis.[27]
FND does not show up on blood tests or structural brain imaging such as MRI or CT scanning. However, this is also the case for many other neurological conditions so negative investigations should not be used alone to make the diagnosis. FND can occur alongside other neurological diseases and tests may show non-specific abnormalities which cause confusion for doctors and patients.[27]
ICD-11 diagnostic criteria
The International Classification of Disease (ICD-11) have listed functional disorders within the neurology section for the first time,[28] where it's named "Dissociative neurological symptom disorder".[29]
DSM-5 diagnostic criteria
The Diagnostic and Statistical Manual of Mental Illness (DSM-5) lists the following diagnostic criteria for functional neurological symptoms (conversion disorder):
- One or more symptoms of altered voluntary motor or sensory function.
- Clinical findings can provide evidence of incompatibility between the symptom and recognized neurological or medical conditions.
- Another medical or mental disorder does not better explain the symptom or deficit.
- The symptom or deficit results in clinically significant distress or impairment in social, occupational, or other vital areas of functioning or warrants medical evaluation.[30]
Differential diagnoses
Multiple sclerosis has some overlapping symptoms with FND, potentially a source of misdiagnosis.[31]
Treatment
Treatment requires a firm and transparent diagnosis based on positive features which both health professionals and patients can feel confident about.[18] It is essential that the health professional confirms that this is a common problem which is genuine, not imagined and not a diagnosis of exclusion.[33]
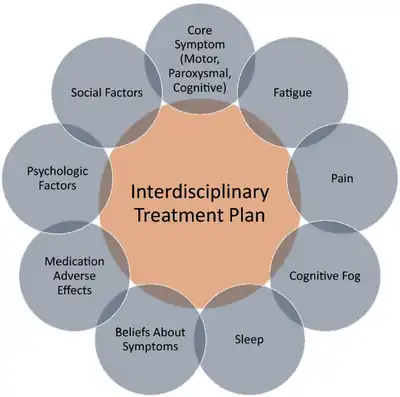
A multi-disciplinary approach to treating functional neurological disorder is recommended. Treatment options can include:[34]
- Physiotherapy and occupational therapy
- Medication such as sleeping tablets, painkillers, anti-epileptic medications and anti-depressants (for patients with depression co-morbid or for pain relief)
Physiotherapy with someone who understands functional disorders may be the initial treatment of choice for patients with motor symptoms such as weakness, gait (walking) disorder and movement disorders. Nielsen et al. have reviewed the medical literature on physiotherapy for functional motor disorders up to 2012 and concluded that the available studies, although limited, mainly report positive results.[35]
For many patients with FND, accessing treatment can be difficult. Availability of expertise is limited and they may feel that they are being dismissed or told 'it's all in your head' especially if psychological input is part of the treatment plan. Some medical professionals are uncomfortable explaining and treating patients with functional symptoms. Changes in the diagnostic criteria, increasing evidence, literature about how to make the diagnosis and how to explain it and changes in medical training is slowly changing this.[36]
Prevalence
Dissociative (non-epileptic) seizures account for about 1 in 7 referrals to neurologists after an initial seizure, and functional weakness has a similar prevalence to multiple sclerosis.[37]
History
From the 18th century, there was a move from the idea of FND being caused by the nervous system. This led to an understanding that it could affect both sexes. Jean Martin Charcot argued that, what would be later called FND, was caused by "a hereditary degeneration of the nervous system, namely a neurological disorder".[38]
In the 18th century, the illness was confirmed as a neurological disorder but a small number of doctors still believed in the previous definition.[38] However, as early as 1874, doctors, including W.B. Carpenter and J.A. Omerod, began to speak out against this other term due to there being no evidence of its existence.[39]
Although the term "conversion disorder" has been used for many years, another term was still being used in the 20th century. However, by this point, it bore little resemblance to the original meaning. It referred instead to symptoms that could not be explained by a recognised organic pathology, and was therefore believed to be the result of stress, anxiety, trauma or depression. The term fell out of favour over time due to the negative connotations. Furthermore, critics pointed out that it can be challenging to find organic pathologies for all symptoms, and so the practice of diagnosing that patients who had such symptoms were imagining them led to the disorder being meaningless, vague and a sham-diagnosis, as it did not refer to any definable disease.[39]
Throughout its history, many patients have been misdiagnosed with conversion disorder when they had organic disorders such as tumours or epilepsy or vascular diseases. This has led to patient deaths, a lack of appropriate care and suffering for the patients. Eliot Slater, after studying the condition in the 1950s, was outspoken against the condition, as there has never been any evidence to prove that it exists. He stated that "The diagnosis of 'hysteria' is a disguise for ignorance and a fertile source of clinical error. It is, in fact, not only a delusion but also a snare".[39]
In 1980, the DSM III added 'conversion disorder' to its list of conditions. The diagnostic criteria for this condition are nearly identical to those used for hysteria. The diagnostic criteria were:
A. The predominant disturbance is a loss of or alteration in physical functioning suggesting a physical disorder. It is involuntary and medically unexplainable
B. One of the following must also be present:
- A temporal relationship between symptom onset and some external event of psychological conflict.
- The symptom allows the individual to avoid unpleasant activity.
- The symptom provides opportunity for support which may not have been otherwise available.
During the COVID-19 pandemic, neurologists noticed an increase in adolescents and young adults presenting with functional tic-like behaviors to clinics around the world.[40] Researchers believe that social media content regarding Tourette Syndrome influenced the sudden increase in functional tic-like behaviors.[41] The majority of the people who experienced functional tic-like behaviors were female, and neurologists have reported an overrepresentation of transgender and non-binary identities within this group of adolescents and young adults.[42]
Today, there is a growing understanding that symptoms are real and distressing, and are caused by an incorrect functioning of the brain rather than being imagined or made up.[43]
Controversy
There was historically much controversy surrounding the FND diagnosis. Many doctors continue to believe that all FND patients have unresolved traumatic events (often of a sexual nature) which are being expressed in a physical way. However, some doctors do not believe this to be the case. Wessely and White have argued that FND may merely be an unexplained somatic symptom disorder.[44] FND remains a stigmatized condition in the healthcare setting.[45][46]
References
- ↑ Stone J, Sharpe M, Rothwell PM, Warlow CP (May 2003). "The 12 year prognosis of unilateral functional weakness and sensory disturbance". Journal of Neurology, Neurosurgery, and Psychiatry. 74 (5): 591–596. doi:10.1136/jnnp.74.5.591. PMC 1738446. PMID 12700300.
- ↑ Aybek S, Perez DL (January 2022). "Diagnosis and management of functional neurological disorder". BMJ. 376: o64. doi:10.1136/bmj.o64. PMID 35074803.
- ↑ Carey, Katie; Watson, Meagan (2003). Reset & Rewire: The FND Workbook for Kids & Teens. Houston, TX: Illustrated Nurse Press. p. 4. ISBN 9798218232047.
- ↑ Lehn A, Gelauff J, Hoeritzauer I, Ludwig L, McWhirter L, Williams S, et al. (March 2016). "Functional neurological disorders: mechanisms and treatment". Journal of Neurology. 263 (3): 611–620. doi:10.1007/s00415-015-7893-2. PMID 26410744. S2CID 23921058.
- ↑ Goldstein LH, Robinson EJ, Chalder T, Reuber M, Medford N, Stone J, et al. (March 2022). "Six-month outcomes of the CODES randomised controlled trial of cognitive behavioural therapy for dissociative seizures: A secondary analysis". Seizure. 96: 128–136. doi:10.1016/j.seizure.2022.01.016. PMC 8970049. PMID 35228117.
- ↑ "Functional neurologic disorders/conversion disorder - Symptoms and causes". Mayo Clinic. Archived from the original on 2017-10-08. Retrieved 2022-01-04.
- ↑ "Functional neurological symptom disorder". www.medicalnewstoday.com. 2022-01-05. Archived from the original on 2020-11-24. Retrieved 2022-01-08.
- ↑ "Functional neurologic disorders/conversion disorder - Symptoms and causes". Mayo Clinic. Archived from the original on 2017-10-08. Retrieved 2022-01-08.
- ↑ "Functional Neurological Disorder". Physiopedia. Archived from the original on 2021-06-24. Retrieved 2022-01-08.
- ↑ "Symptoms – Functional Neurological Disorder (FND)". Archived from the original on 2021-09-26. Retrieved 2022-08-18.
- ↑ Fiszman A, Kanner AM (2010). Schachter SC, LaFrance Jr WC (eds.). Gates and Rowan's nonepileptic seizures (3rd ed.). Cambridge: Cambridge University Press. pp. 225–234. ISBN 978-0-521-51763-8.
- ↑ Henningsen P, Zimmermann T, Sattel H (2003). "Medically unexplained physical symptoms, anxiety, and depression: a meta-analytic review". Psychosomatic Medicine. 65 (4): 528–533. doi:10.1097/01.psy.0000075977.90337.e7. PMID 12883101. S2CID 4138482.
- ↑ Edwards MJ, Stone J, Lang AE (June 2014). "From psychogenic movement disorder to functional movement disorder: it's time to change the name". Movement Disorders. 29 (7): 849–852. doi:10.1002/mds.25562. PMID 23843209. S2CID 24218238.
- ↑ Kranick S, Ekanayake V, Martinez V, Ameli R, Hallett M, Voon V (August 2011). "Psychopathology and psychogenic movement disorders". Movement Disorders. 26 (10): 1844–1850. doi:10.1002/mds.23830. PMC 4049464. PMID 21714007.
- ↑ Ludwig L, Pasman JA, Nicholson T, Aybek S, David AS, Tuck S, et al. (April 2018). "Stressful life events and maltreatment in conversion (functional neurological) disorder: systematic review and meta-analysis of case-control studies". The Lancet. Psychiatry. 5 (4): 307–320. doi:10.1016/S2215-0366(18)30051-8. PMID 29526521. Archived from the original on 2023-01-31. Retrieved 2023-08-13.
- ↑ Aybek S, Vuilleumier P (2016). "Imaging studies of functional neurologic disorders". Functional Neurologic Disorders. Handbook of Clinical Neurology. Vol. 139. pp. 73–84. doi:10.1016/b978-0-12-801772-2.00007-2. ISBN 9780128017722. PMID 27719879.
- ↑ "Imaging Study Provides New Biological Insights on Functional Neurological Disorder". Imaging Technology News. 2019-11-28. Archived from the original on 2022-01-08. Retrieved 2022-01-08.
- 1 2 Bennett K, Diamond C, Hoeritzauer I, Gardiner P, McWhirter L, Carson A, Stone J (January 2021). "A practical review of functional neurological disorder (FND) for the general physician". Clinical Medicine. 21 (1): 28–36. doi:10.7861/clinmed.2020-0987. PMC 7850207. PMID 33479065.
- ↑ D'Souza RS, Vogt MN, Rho EH (August 2020). "Post-operative functional neurological symptom disorder after anesthesia". Bosnian Journal of Basic Medical Sciences. 20 (3): 381–388. doi:10.17305/bjbms.2020.4646. PMC 7416177. PMID 32070267.
- ↑ Espay AJ, Aybek S, Carson A, Edwards MJ, Goldstein LH, Hallett M, et al. (September 2018). "Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders". JAMA Neurology. 75 (9): 1132–1141. doi:10.1001/jamaneurol.2018.1264. PMC 7293766. PMID 29868890.
- ↑ Sonoo M (January 2004). "Abductor sign: a reliable new sign to detect unilateral non-organic paresis of the lower limb". Journal of Neurology, Neurosurgery, and Psychiatry. 75 (1): 121–125. PMC 1757483. PMID 14707320.
- ↑ Thenganatt MA, Jankovic J (27 August 2014). "Psychogenic tremor: a video guide to its distinguishing features". Tremor and Other Hyperkinetic Movements. 4: 253. doi:10.7916/D8FJ2F0Q. PMC 4161970. PMID 25243097.
- ↑ Mellers JD (August 2005). "The approach to patients with "non-epileptic seizures"". Postgraduate Medical Journal. 81 (958): 498–504. doi:10.1136/pgmj.2004.029785. PMC 1743326. PMID 16085740.
- ↑ Pick S, Rojas-Aguiluz M, Butler M, Mulrenan H, Nicholson TR, Goldstein LH (July 2020). "Dissociation and interoception in functional neurological disorder". Cognitive Neuropsychiatry. 25 (4): 294–311. doi:10.1080/13546805.2020.1791061. PMID 32635804. S2CID 220410893.
- ↑ Wiginton K. "What Is Dissociation?". WebMD. Archived from the original on 2020-05-10. Retrieved 2022-01-08.
- ↑ Adams C, Anderson J, Madva EN, LaFrance WC, Perez DL (August 2018). "You've made the diagnosis of functional neurological disorder: now what?". Practical Neurology. 18 (4): 323–330. doi:10.1136/practneurol-2017-001835. PMC 6372294. PMID 29764988.
- 1 2 Stone J, Smyth R, Carson A, Lewis S, Prescott R, Warlow C, Sharpe M (October 2005). "Systematic review of misdiagnosis of conversion symptoms and "hysteria"". BMJ. 331 (7523): 989. doi:10.1136/bmj.38628.466898.55. PMC 1273448. PMID 16223792.
- ↑ Stone J, Hallett M, Carson A, Bergen D, Shakir R (December 2014). "Functional disorders in the Neurology section of ICD-11: A landmark opportunity". Neurology. 83 (24): 2299–2301. doi:10.1212/wnl.0000000000001063. PMC 4277679. PMID 25488992.
- ↑ "ICD-11 for Mortality and Morbidity Statistics". icd.who.int. Archived from the original on 2018-08-01. Retrieved 2023-03-05.
- ↑ Peeling JL, Muzio M (2022). "Conversion Disorder". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 31855394. Archived from the original on 2023-03-02. Retrieved 2023-03-05.
- ↑ Walzl D, Solomon AJ, Stone J (February 2022). "Functional neurological disorder and multiple sclerosis: a systematic review of misdiagnosis and clinical overlap". Journal of Neurology. 269 (2): 654–663. doi:10.1007/s00415-021-10436-6. PMC 8782816. PMID 33611631.
- ↑ Gilmour, Gabriela S.; Nielsen, Glenn; Teodoro, Tiago; Yogarajah, Mahinda; Coebergh, Jan Adriaan; Dilley, Michael D.; Martino, Davide; Edwards, Mark J. (July 2020). "Management of functional neurological disorder". Journal of Neurology. 267 (7): 2164–2172. doi:10.1007/s00415-020-09772-w. ISSN 1432-1459. Retrieved 11 October 2023.
- ↑ "Functional Neurological Disorder". NORD (National Organization for Rare Disorders). Archived from the original on 2022-01-20. Retrieved 2022-01-20.
- ↑ Espay AJ, Aybek S, Carson A, Edwards MJ, Goldstein LH, Hallett M, et al. (September 2018). "Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders". JAMA Neurology. 75 (9): 1132–1141. doi:10.1001/jamaneurol.2018.1264. PMC 7293766. PMID 29868890.
- ↑ Nielsen G, Stone J, Edwards MJ (August 2013). "Physiotherapy for functional (psychogenic) motor symptoms: a systematic review". Journal of Psychosomatic Research. 75 (2): 93–102. doi:10.1016/j.jpsychores.2013.05.006. PMID 23915764.
- ↑ Edwards MJ (February 2016). "Functional neurological symptoms: welcome to the new normal". Practical Neurology. 16 (1): 2–3. doi:10.1136/practneurol-2015-001310. PMID 26769760. S2CID 29823685.
- ↑ Stone J (March 2011). "Functional neurological symptoms". The Journal of the Royal College of Physicians of Edinburgh. 41 (1): 38–41, quiz 42. doi:10.4997/JRCPE.2011.110. PMID 21365066.
- 1 2 Tasca C, Rapetti M, Carta MG, Fadda B (2012-10-19). "Women and hysteria in the history of mental health". Clinical Practice and Epidemiology in Mental Health. 8: 110–119. doi:10.2174/1745017901208010110. PMC 3480686. PMID 23115576.
- 1 2 3 Webster R. "Sigmund Freud: somatization, medicine and misdiagnosis". www.richardwebster.net. Archived from the original on May 11, 2004. Retrieved 2016-02-21.
{{cite web}}: CS1 maint: unfit URL (link) - ↑ Pringsheim T, Ganos C, McGuire JF, Hedderly T, Woods D, Gilbert DL, et al. (December 2021). "Rapid Onset Functional Tic-Like Behaviors in Young Females During the COVID-19 Pandemic". Movement Disorders. 36 (12): 2707–2713. doi:10.1002/mds.28778. PMC 8441698. PMID 34387394.
- ↑ Olvera C, Stebbins GT, Goetz CG, Kompoliti K (November 2021). "TikTok Tics: A Pandemic Within a Pandemic". Movement Disorders Clinical Practice. 8 (8): 1200–1205. doi:10.1002/mdc3.13316. PMC 8564823. PMID 34765687.
- ↑ Ghorayshi A, Bracken A (2023-02-13). "How Teens Recovered From the 'TikTok Tics'". The New York Times. ISSN 0362-4331. Archived from the original on 2023-05-19. Retrieved 2023-05-19.
- ↑ "Functional neurologic disorders/conversion disorder". Mayo Clinic. Archived from the original on 2017-10-08. Retrieved 2023-08-13.
- ↑ Wessely S, White PD (August 2004). "There is only one functional somatic syndrome". The British Journal of Psychiatry. 185 (2): 95–96. doi:10.1192/bjp.185.2.95. PMID 15286058.
- ↑ Kozlowska K, Sawchuk T, Waugh JL, Helgeland H, Baker J, Scher S, Fobian AD (2021). "Changing the culture of care for children and adolescents with functional neurological disorder". Epilepsy & Behavior Reports. 16: 100486. doi:10.1016/j.ebr.2021.100486. PMC 8567196. PMID 34761194.
- ↑ O'Neal MA, Dworetzky BA, Baslet G (2021-01-01). "Functional neurological disorder: Engaging patients in treatment". Epilepsy & Behavior Reports. 16: 100499. doi:10.1016/j.ebr.2021.100499. PMC 8633865. PMID 34877516.
Further reading
- Kwon D (November 2020). "A Disorder of Mind and Brain: A mysterious condition once known as hysteria is challenging the divide between psychiatry and neurology". Scientific American. 323 (5): 58–65 (60).
A variety of conditions that have variously been termed "hysteria", "conversion disorder", or "psychosomatic illness" have most recently been given the name "functional neurological disorder (FND), [which] is deliberately neutral, simply denoting a problem in the functioning of the nervous system