Haim–Munk syndrome
| Haim–Munk syndrome | |
|---|---|
| Other names: Palmoplantar keratoderma with periodontitis and arachnodactyly and acro-osteolysis | |
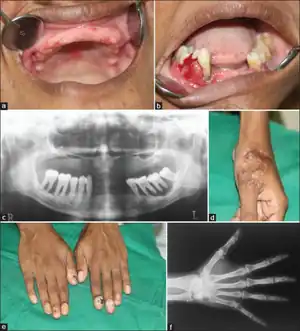 | |
| a) edentulous maxilla, b) aggressive periodontitis, c)orthopantomogram of maxilla , d) healed lesion,e) onychogryphosis of fingers, x-ray of wrist | |
Haim–Munk syndrome (also known as "palmoplantar keratoderma with periodontitis and arachnodactyly and acro-osteolysis"[1]) is a skin disease caused, like Papillon-Lefevre Syndrome, by a mutation in the cathepsin C gene.[1]
It is named after Salim Haim and J. Munk,[2] who first described the disease in 1965.[3]
Symptoms and signs
Most of the signs of Haim–Munk syndrome begin to manifest during the first 2–4 years of life.[4]
Commons signs at this stage are thickening and scaling of the skin of the palms, soles (palmoplantar keratoderma) and elbows, and shedding of the primary dentition caused by recurrent episodes of dental caries and periodontitis. Patients also demonstrate hypertrophy and curving of nails (onychogryphosis), flat foot, extreme length and slenderness of fingers and toes (arachnodactyly), and osteolysis involving the distal phalanges of fingers and toes (acro-osteolysis).[5][6]
Permanent flexion contractures of the large and small joints may occur as the disease progresses.
Causes
Haim–Munk syndrome is an inherited autosomal recessive trait.[5] In some instances, the parents of individuals with Haim–Munk syndrome are consanguineously related.[5] Genetic analysis suggests that Haim–Munk syndrome may be due to the genetic mutation of gene CTSC cathepsin C Archived 2020-10-21 at the Wayback Machine, which is located on the long arm of chromosome 11.[5] Furthermore, analysis demonstrates that in individuals with Haim–Munk syndrome, a haplotype surrounded the gene location and appeared to be transmitted with it as unit. This suggests that the CTSC gene was inherited from a common ancestor.[5]
The CTSC cathepsin C gene regulates the production of the enzyme cathepsin C, which is expressed in various organs and tissues. The CTSC gene is thought to play a role in the differentiation of epithelial cells, resulting in the hyperkeratosis and erythema of the soles of feet and palms of hands,[5][6] and connects the gingiva to the tooth surface.[5]
Diagnosis
Diagnosis comes from the taking of a comprehensive patient history and identification of characteristic symptoms. Identification of the physical symptoms is important to distinguish this disease from Papillon-Lefevre Syndrome.[5]
In many cases diagnosis of Haim–Munk syndrome may be difficult in small children, as many symptoms can be confused with other skin abnormalities. Diagnosis of the disease often comes between the ages of three and five when infant teeth begin to erupt, and the inflammation and degeneration of the tissues surrounding and supporting the teeth becomes apparent.[5]
Treatment
Treatment of HMS is similar to that for Papillon-Lefevre Syndrome.[7]
- Oral retinoids, such as acitretin, etretinate, and isotretinoin, for the treatment of keratoderma and, less effectively, for periodontitis. Topical emollients, salicylic acid and urea preparations can also be used as adjuncts.
- Extraction of the primary teeth combined with oral antibiotics and professional teeth cleaning, for periodontitis.
It has been reported that Inflammation associated with the arthritis caused by HMS can be controlled by removal of the synovial tissue surrounding affected joints (synovectomy), at the cost of permanent handicap.[8]
See also
References
- 1 2 Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 978-1-4160-2999-1.
- ↑ Al Aboud, Khalid; Al Aboud Daifullah (2011). "Salim Haim and the syndrome that bears his name". Dermatol. Online J. United States. 17 (8): 15. PMID 21906495.
- ↑ Haim, S.; Munk, J. (January 1965). "Keratosis palmo-plantaris congenita, with periodontosis, arachnodactyly and a peculiar deformity of the terminal phalanges". The British Journal of Dermatology. 77: 42–54. doi:10.1111/j.1365-2133.1965.tb14565.x. ISSN 0007-0963. PMID 14252683. S2CID 19794326.
- ↑ Janjua, Shahbaz A.; Iftikhar, Nadia; Hussain, Ijaz; Khachemoune, Amor (2008). "Dermatologic, periodontal, and skeletal manifestations of Haim-Munk syndrome in two siblings". Journal of the American Academy of Dermatology. 58 (2): 339–344. doi:10.1016/j.jaad.2007.08.004. PMID 18222334.
- 1 2 3 4 5 6 7 8 9 "Haim-Munk Syndrome - NORD (National Organization for Rare Disorders)". NORD (National Organization for Rare Disorders). Archived from the original on 2016-04-24. Retrieved 2018-04-17.
- 1 2 Pahwa, Priyanka; Lamba, Arundeep K; Faraz, Farrukh; Tandon, Shruti (2010-07-01). "Haim-Munk syndrome". Journal of Indian Society of Periodontology. 14 (3): 201–203. doi:10.4103/0972-124x.75919. PMC 3100867. PMID 21760678.
- ↑ Siragusa, M.; Romano, C.; Batticane, N.; Batolo, D.; Schepis, C. (March 2000). "A new family with Papillon-Lefèvre syndrome: effectiveness of etretinate treatment". Cutis. 65 (3): 151–155. ISSN 0011-4162. PMID 10738634.
- ↑ Lidar, Merav; Zlotogorski, Abraham; Langevitz, Pnina; Tweezer-Zaks, Nurit; Zandman-Goddard, Gisele (April 2004). "Destructive arthritis in a patient with Haim-munk syndrome". The Journal of Rheumatology. 31 (4): 814–817. ISSN 0315-162X. PMID 15088315.
External links
| Classification |
|---|