Linburg–Comstock variation
| Linburg–Comstock variation | |
|---|---|
| Other names | Linburg–Comstock syndrome |
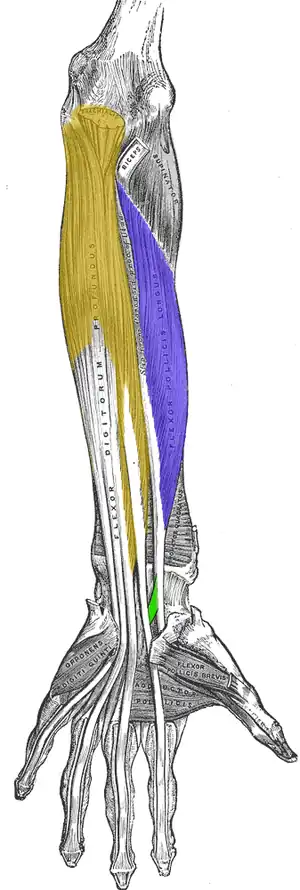 | |
| Linburg and Comstock syndrome is seen as a tendinous connection (green) between flexor pollicis longus (purple) and flexor digitorum profundus (yellow). | |
| Specialty | Orthopedic surgery, plastic surgery |
Linburg–Comstock variation is an occasional tendinous connection between the flexor pollicis longus and the flexor digitorum profundus of the index, the middle finger or both. It is found in around 21% of the population.[1] It is an anatomical variation in human, which may be viewed as a pathology if causes symptoms. It was recognised as early as the 1800s, but was first described by Linburg and Comstock in 1979.[2]
Signs and symptoms
Although Linburg–Comstock variation remains asymptomatic, a number of case reports suggested that symptoms could develop after a forceful extension of the index finger with the thumb in a flexed position.[3][4] Symptoms also develop from heavy and repetitive use of the wrist and forearm and can also develop in those who require fine and independent functionality of the fingers, such as musicians.[3][4]
This abnormality is clinically evident when the patient is unable to flex the thumb without flexing the distal interphalangeal joint of the index or middle finger or vice versa.
Flexor tenosynovitis is a common finding in the patients with Linburg–Comstock syndrome. Another hypothesis is that anatomical variations, which in this case is an additional tendon slip, may act as space-occupying lesions and potentially contribute to carpal tunnel syndrome.[5]
Structure
Development
Linburg–Comstock variation and syndrome may result from phylogenetic differences between human and non-human primates. Phylogenetically, the flexor pollicis longus and the flexor digitorum profundus both originate from a common mesodermal mass.[6] In non-human primates, there is only one flexor muscle for all the fingers, whereas in humans, the flexor pollicis longus becomes distinct.[7] Linburg–Comstock syndrome may be viewed as an evolutionary persistent structure. It is still inconclusive whether or not the connection is congenital or acquired at a later time point in life.[8]
Anatomy
Multiple types of the connection between the flexor pollicis longus and the flexor digitorum profundus were described:[9]
- A tendinous connection between the flexor digitorum profundus of the index to the flexor pollicis longus
- A muscle with a bifurcated (split into two) tendon for the thumb and index finger
- A common muscle with five tendons for the thumb and the long fingers
Diagnosis
The examiner passively restricts the flexion of the fingers while the examinee attempts to actively flex the thumb.[10] A positive test is marked by restricted active thumb flexion with pain or cramping discomfort in the palmar and radial sides of the distal (lower) forearm or wrist.[10] The magnetic resonance imaging (MRI) can confirm and localise Linburg and Comstock syndrome.[10] As reported by Karalezli, magnetic resonance imaging was performed on all patients diagnosed with positive test, and there were tendinous connection in all cases.[11]
Treatment
Surgery may be performed by excising or splitting the tendinous connection to form two separate tendons, depending on the nature of the connection.[12] Muscle belly associated with the symptoms may also be removed.[6]
Epidemiology
This variant occurred bilaterally (in both hands) in 14% and unilaterally in 31% (either in left or right hand) out of 194 patients as reported by the original study.[2] Four cases were responsible for chronic tenosynovitis.[2] A recent meta analysis reported that the connection is present in 21% of the population.[1]
References
- 1 2 Yammine, Kaissar; Erić, Mirela (7 December 2017). "Linburg–Comstock variation and syndrome. A meta-analysis". Surgical and Radiologic Anatomy. 40 (3): 289–296. doi:10.1007/s00276-017-1957-1. ISSN 0930-1038. PMID 29218383. S2CID 4346785.
- 1 2 3 Linburg, R. M.; Comstock, B. E. (1 January 1979). "Anomalous tendon slips from the flexor pollicis longus to the flexor digitorum profundus". Journal of Hand Surgery, American Volume. 4 (1): 79–83. doi:10.1016/s0363-5023(79)80110-0. ISSN 0363-5023. PMID 759509.
- 1 2 Takami, Hiroshi; Takahashi, Sadao; Ando, Masashi (March 1996). "The Linburg Comstock anomaly: A case report". Journal of Hand Surgery, American Volume. 21 (2): 251–252. doi:10.1016/S0363-5023(96)80110-9. PMID 8683056.
- 1 2 Furukawa, Kayoko; Menuki, Kunitaka; Sakai, Akinori; Oshige, Toshihisa; Nakamura, Toshitaka (1 January 2012). "Linburg-comstock syndrome: a case report". Hand Surgery. 17 (2): 217–220. doi:10.1142/S0218810412720197. ISSN 0218-8104. PMID 22745086.
- ↑ Slater, R. R (1 August 2001). "Flexor tendon anomalies in a patient with carpal tunnel syndrome". Journal of Hand Surgery, British Volume. 26 (4): 373–376. doi:10.1054/jhsb.2001.0613. PMID 11469843. S2CID 35725315.
- 1 2 Slater, R. R. (1 August 2001). "Flexor tendon anomalies in a patient with carpal tunnel syndrome". Journal of Hand Surgery, British Volume. 26 (4): 373–376. doi:10.1054/jhsb.2001.0613. ISSN 0266-7681. PMID 11469843. S2CID 35725315.
- ↑ Stahl, Shalom; Stahl, Shy; Calif, Edward (2005). "Failure of Flexor Pollicis Longus Repair Caused By Anomalous Flexor Pollicis Longus to Index Flexor Digitorum Profundus Interconnections: A Case Report". Journal of Hand Surgery, American Volume. 30 (3): 483–486. doi:10.1016/j.jhsa.2005.01.005. PMID 15925156. Retrieved 13 February 2016.
- ↑ Bulut, T; Tahta, M; Ozturk, T; Zengin, EC; Ozcan, C; Sener, M (21 September 2017). "Linburg-Comstock: Is Overuse an Etiological Factor?". Plastic Surgery. 25 (4): 268–271. doi:10.1177/2292550317731763. PMC 5871072. PMID 29619350.
- ↑ Spaepen, D.; De Marteleire, W.; De Smet, Luc (1 October 2003). "Symptomatic Linburg–Comstock syndrome: a case report". Acta Orthopaedica Belgica. 69 (5): 455–457. ISSN 0001-6462. PMID 14648957.
- 1 2 3 Yoon, Hong-Kee; Kim, Chang-Hyun (1 September 2013). "Linburg-Comstock syndrome involving four fingers: a case report and review of the literature". Journal of Plastic, Reconstructive & Aesthetic Surgery. 66 (9): 1291–1294. doi:10.1016/j.bjps.2012.12.032. ISSN 1878-0539. PMID 23379987.
- ↑ Karalezli, Nazım; Karakose, Serdar; Haykir, Rahime; Yagisan, Nihan; Kacira, Burkay; Tuncay, Ibrahim (July 2006). "Linburg–Comstock anomaly in musicians". Journal of Plastic, Reconstructive & Aesthetic Surgery. 59 (7): 768–771. doi:10.1016/j.bjps.2006.01.003. PMID 16782576.
- ↑ Badhe, S.; Lynch, J.; Thorpe, S. K. S.; Bainbridge, L. C. (1 September 2010). "Operative treatment of Linburg–Comstock syndrome". The Journal of Bone and Joint Surgery. British Volume. 92-B (9): 1278–1281. doi:10.1302/0301-620X.92B9.23577. ISSN 2049-4394. PMID 20798448. S2CID 6317353.