Pancytopenia
| Pancytopenia | |
|---|---|
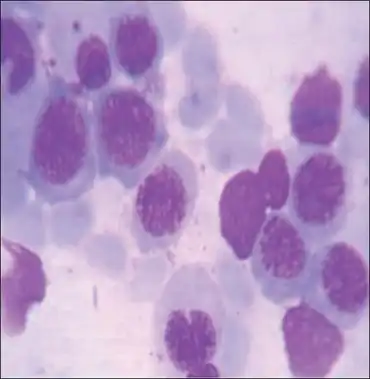 | |
| Bone marrow showing megaloblasts, with royal blue cytoplasm and sieve-like chromatin | |
| Specialty | Hematology |
Pancytopenia is a medical condition in which there is a reduction in the number of red and white blood cells, as well as platelets.
If only two parameters from the complete blood count are low, the term bicytopenia can be used. The diagnostic approach is the same as for pancytopenia.
Signs and symptoms
The clinical presentation of Pancytopenia is as follows:[1]
- Shortness of breath
- Fatigue
- Chest pain
- Infections
Causes
Iatrogenic causes of pancytopenia include chemotherapy for malignancies if the drug or drugs used cause bone marrow suppression. Rarely, drugs (antibiotics, blood pressure medication, heart medication) can cause pancytopenia. For example, the antibiotic chloramphenicol can cause pancytopenia in some individuals.[2]
Rarely, pancytopenia may have other causes, such as mononucleosis or other viral diseases. Increasingly, HIV is itself a cause of pancytopenia.[3]
- Familial hemophagocytic syndrome
- Aplastic anemia
- Gaucher's disease
- Metastatic carcinoma of bone
- Multiple Myeloma
- Overwhelming infections
- Lymphoma
- Myelofibrosis
- Dyskeratosis congenita
- Myelodysplastic syndrome
- Leukemia
- Leishmaniasis
- Severe folate or vitamin B12 deficiency
- Systemic lupus erythematosus
- Paroxysmal nocturnal hemoglobinuria (blood test)
- Viral infections (such as HIV, EBV; an undetermined virus is most common)
- Alimentary toxic aleukia
- Copper deficiency
- Pernicious anemia
- Medication
- Hypersplenism
- Osteopetrosis
- Organic acidurias (Propionic Acidemia, Methylmalonic Aciduria, Isovaleric Aciduria)
- Low dose arsenic poisoning
- Sako disease (Myelodysplastic-cytosis)
- Chronic radiation sickness[4]
- LIG4 syndrome
Mechanism
Common concept is pancytopenia can occur either due to mother cells are decreased themselves in number (aplastic anemia), mother cells are overwhelmed by malignanrt cells (Leukemia, lymphoma, MDS) or they are being sequestrated (spleen)/destroyed (immune) outside bone marrow. The mechanisms for pancytopenia differ according to the etiology. For example, in hemophagocytic lymphohistiocytosis (HLH) there is marked inappropriate and ineffective T cell activation that leads to an increased hemophagocytic activity. The T cell activated macrophages engulf erythrocytes, leukocytes, platelets, as well as their progenitor cells. Along with pancytopenia, HLH is characterized by fever, splenomegaly, and hemophagocytosis in bone marrow, liver, or lymph nodes.[5]
Diagnosis
Pancytopenia usually requires a bone marrow biopsy in order to distinguish among different causes.[6]
- anemia: hemoglobin < 13.5 g/dL (male) or 12 g/dL (female).
- leukopenia: total white cell count < 4.0 x 109/L. Decrease in all types of white blood cells (revealed by doing a differential count).
- thrombocytopenia: platelet count < 150×109/L.
Treatment
Treatment is done to address the underlying cause. To tide over immediate crisis Blood transfusion with packed red blood cells (PRBC) or platelet transfusion may be done. Sometimes there are obvious clinical clues to suggest underlying B12 deficiency for a cause of pancytopenia.[7] In this selected cases even with severe anemia blood product transfusions can be avoided and vitamin B12 treatment itself suffice.[8] In other situations like acute leukemia, Myelodysplastic syndrome, aplastic anemia etc. disease specific therapy is needed.[9]
References
- ↑ Chiravuri, Shalini; De Jesus, Orlando (2022). "Pancytopenia". StatPearls. StatPearls Publishing. Archived from the original on 10 January 2022. Retrieved 13 February 2022.
- ↑ Abdollahi, M.; Mostafalou, S. (2014), "Chloramphenicol", Encyclopedia of Toxicology, Elsevier, pp. 837–840, doi:10.1016/b978-0-12-386454-3.00709-0, ISBN 978-0-12-386455-0, archived from the original on 2022-02-14, retrieved 2020-12-11
- ↑ Jain, Arvind; Naniwadekar, Manjiri (2013-11-06). "An etiological reappraisal of pancytopenia - largest series reported to date from a single tertiary care teaching hospital". BMC Blood Disorders. 13 (1): 10. doi:10.1186/2052-1839-13-10. ISSN 1471-2326. PMC 4177001. PMID 24238033. Archived from the original on 2022-02-14. Retrieved 2022-02-10.
- ↑ Kossenko MM, Akleyev AA, Degteva MO, Kozheurov VP, Degtyaryova RC (August 1994). "Analysis of Chronic Radiation Sickness Cases in the Population of the Southern Urals (AD-A286 238)". DTIC. p. 5. Archived from the original on 8 October 2012. Retrieved 1 August 2013.
Complete blood counts, when taken, revealed pancytopenia.
- ↑ Trottestam, Helena; Horne, AnnaCarin; Aricò, Maurizio; Egeler, R. Maarten; Filipovich, Alexandra H.; Gadner, Helmut; Imashuku, Shinsaku; Ladisch, Stephan; Webb, David; Janka, Gritta; Henter, Jan-Inge (2011-10-27). "Chemoimmunotherapy for hemophagocytic lymphohistiocytosis: long-term results of the HLH-94 treatment protocol". Blood. 118 (17): 4577–4584. doi:10.1182/blood-2011-06-356261. ISSN 0006-4971. PMC 3208276. PMID 21900192.
- ↑ "Rudhiram Hematology Clinic - Google Search". www.google.com. Archived from the original on 2022-02-14. Retrieved 2022-02-02.
- ↑ Devalia, Vinod; Hamilton, Malcolm S.; Molloy, Anne M. (2014). "Guidelines for the diagnosis and treatment of cobalamin and folate disorders". British Journal of Haematology. 166 (4): 496–513. doi:10.1111/bjh.12959. ISSN 1365-2141. PMID 24942828. S2CID 5772424. Archived from the original on 2021-03-08. Retrieved 2022-02-10.
- ↑ Devalia, Vinod; Hamilton, Malcolm S.; Molloy, Anne M. (2014). "Guidelines for the diagnosis and treatment of cobalamin and folate disorders". British Journal of Haematology. 166 (4): 496–513. doi:10.1111/bjh.12959. ISSN 1365-2141. PMID 24942828. S2CID 5772424. Archived from the original on 2021-03-08. Retrieved 2022-02-10.
- ↑ Risitano, Antonio M.; Maciejewski, Jaroslaw P.; Selleri, Carmine; Rotoli, Bruno; Risitano, Antonio M.; Maciejewski, Jaroslaw P. (2007). "Function and Malfunction of Hematopoietic Stem Cells in Primary Bone Marrow Failure Syndromes". Current Stem Cell Research & Therapy. 2 (1): 39–52. doi:10.2174/157488807779316982. PMID 18220891. Archived from the original on 2022-02-03. Retrieved 2022-02-10.
External links
- EID Journal (Volume 6, Number 6) Archived 2011-08-01 at the Wayback Machine, CDC, December 2000.
| Classification |
|---|