Morton's neuroma
| Morton's neuroma | |
|---|---|
| Other names: Morton neuroma, Morton's metatarsalgia, Intermetatarsal neuroma, and Intermetatarsal space neuroma | |
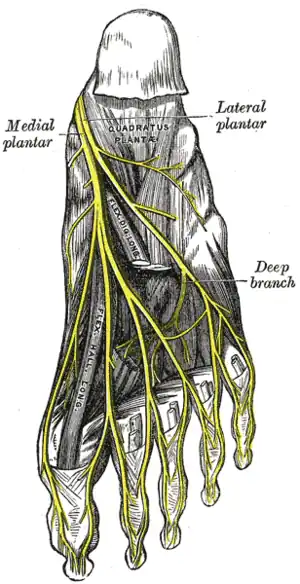 | |
| The plantar nerves. | |
Morton's neuroma is a thickening of a nerve which presents as a swelling usually between the second and third toe.[1] The main symptoms are pain, numbness and burning.[2]
Wearing wide cushioned shoes might help.[2] Other options include steroid injection or surgery.[2]
The condition is named after Thomas George Morton, though it was first correctly described by a chiropodist named Durlacher.[3][4]
Signs and symptoms
Symptoms include pain on weight bearing, frequently after only a short time. The nature of the pain varies widely among individuals. Some people experience shooting pain affecting the contiguous halves of two toes. Others describe a feeling akin to having a pebble in the shoe or walking on razor blades. Burning, numbness, and paresthesia may also be experienced.[5] The symptoms progress over time, often beginning as a tingling sensation in the ball of the foot.[6]
Morton's neuroma lesions have been found using MRI in patients without symptoms.[7]
Diagnosis
Negative signs include a lack of obvious deformities, erythema, signs of inflammation, or limitation of movement. Direct pressure between the metatarsal heads will replicate the symptoms, as will compression of the forefoot between the finger and thumb so as to compress the transverse arch of the foot. This is referred to as Mulder’s Sign.
There are other causes of pain in the forefoot that often lead to miscategorization as neuroma, such as capsulitis, which is an inflammation of ligaments that surround two bones at the level of the joint. If the ligaments that attach the phalanx (bone of the toe) to the metatarsal bone are impacted, the resulting inflammation may put pressure on an otherwise healthy nerve and produce neuroma-type symptoms. Additionally, an intermetatarsal bursitis between the third and fourth metatarsal bones will also give neuroma-type symptoms because it too puts pressure on the nerve. Freiberg disease, which is an osteochondritis of the metatarsal head, causes pain on weight-bearing or compression. Other conditions that could be clinically confused with a neuroma include stress fractures/reactions and plantar plate disruption.[8][9]
Histopathology

Microscopically, the affected nerve is markedly distorted, with extensive concentric perineural fibrosis. The arterioles are thickened and occlusion by thrombi are occasionally present.[10][11]
Imaging
Though a neuroma is a soft-tissue abnormality and will not be visualized by standard radiographs, the first step in the assessment of forefoot pain is an X-ray to detect the presence of arthritis and exclude stress fractures/reactions and focal bone lesions, which may mimic the symptoms of a neuroma. Ultrasound (sonography) accurately demonstrates thickening of the interdigital nerve within the web space of greater than 3mm, diagnostic of a Morton’s neuroma. This typically occurs at the level of the intermetatarsal ligament. Frequently, intermetatarsal bursitis coexists with the diagnosis. MRI can distinguish conditions that mimic the symptoms of Morton's neuroma, but when more than one abnormality exists, ultrasound has the added advantage of determining the precise source of the patient’s pain by applying direct pressure with the probe. Ultrasound may also be used to guide treatment such as cortisone injections into the webspace, as well as alcohol ablation of the nerve.
Treatment
Orthotics and corticosteroid injections are widely used conservative treatments for Morton’s neuroma. In addition to traditional orthotic arch supports, a small foam or fabric pad may be positioned under the space between the two affected metatarsals, immediately behind the bone ends. This pad helps to splay the metatarsal bones and create more space for the nerve so as to relieve pressure and irritation. However, it may also elicit mild uncomfortable sensations of its own, such as the feeling of having an awkward object under one's foot. Corticosteroid injections can relieve inflammation in some patients and help end the symptoms. For some patients, however, the inflammation and pain recur after some weeks or months, and corticosteroids may only be used a limited number of times because they cause progressive degeneration of ligamentous and tendinous tissues.
Sclerosing alcohol injections are an increasingly available treatment alternative if other management approaches fail. Dilute alcohol (4%) is injected directly into the area of the neuroma, causing toxicity to the fibrous nerve tissue. Frequently, treatment must be performed two to four times, with one to three weeks between interventions. A 60–80% success rate has been achieved in clinical studies, equal to or exceeding the success rate for surgical neurectomy, with fewer risks and less significant recovery. If done with more concentrated alcohol under ultrasound guidance, the success rate is considerably higher and fewer repeat procedures are needed.[12]
Radiofrequency ablation is also used in the treatment of Morton's neuroma.[13] The outcomes appear to be similar to, or even more reliable than, alcohol injections, especially if the procedure is performed under ultrasound guidance.[14]
A 2019 systematic review of randomised controlled trials found that corticosteroid injections or manipulation/mobilisation reduced pain more than control, extracorporeal shockwave therapy or varus/valgus foot wedges (which did not reduce pain more than control or comparison treatment, and pain reduction was not reported in any wider foot/metatarsal padding studies). The review also found no randomised controlled trials for sclerosing alcohol injections, radiofrequency ablations, cryoneurolysis or botulinum toxin injections. These treatments have only been assessed with pre-test/post-test case series, which do not measure the benefit of treatment beyond any placebo effect, sham treatment or any natural improvement over time.[15]
If such interventions fail, patients are commonly offered neurectomy, a surgery that involves removing the affected piece of nerve tissue. Postoperative scar tissue formation (known as stump neuroma) can occur in approximately 20–30% of cases, causing a return of neuroma symptoms.[16] Neurectomy may be performed using one of two general methods. Making the incision from the dorsal side (the top of the foot) is the more common method but requires cutting the deep transverse metatarsal ligament that connects the third and fourth metatarsals in order to access the nerve beneath it. This results in exaggerated postoperative splaying of the third and fourth digits (toes) resulting from the loss of the supporting ligamentous structure. This has aesthetic concerns for some patients and possible, though unquantified, long-term implications for foot structure and health. Alternatively, making the incision from the ventral side (the sole of the foot) allows more direct access to the affected nerve without cutting other structures. However, this approach requires a greater post-operative recovery time in which the patient must avoid weight-bearing on the affected foot, because the ventral aspect of the foot is more highly enervated and impacted by pressure when standing. It also carries an increased risk of scar-tissue formation in a location that causes ongoing pain.
Cryogenic neuroablation (also known as cryoinjection therapy, cryoneurolysis, cryosurgery or cryoablation) is a lesser-known alternative to neurectomy surgery. It involves the destruction of axons to prevent them from carrying painful impulses. This is accomplished by making a small incision (~3 mm) and inserting a cryoneedle that applies extremely low temperatures of between −50 °C to −70 °C to the nerve/neuroma,[17] resulting in degeneration of the intracellular elements, axons and myelin sheath (which houses the neuroma) with wallerian degeneration. The epineurium and perineurium remain intact, thus preventing the formation of stump neuroma. The preservation of these structures differentiates cryogenic neuroablation from surgical excision and neurolytic agents such as alcohol. An initial study showed that cryoneuroablation is initially equal in effectiveness to surgery but does not have the risk of stump neuroma formation.[18]
An increasing range of procedures are being performed at specialist centers to treat Morton's neuroma[6][12] under ultrasound guidance. Recent studies have shown excellent results for the treatment of the condition with ultrasound-guided sclerosing alcohol injections,[14][19] radiofrequency ablation[13] and cryoablation.[20]
In popular culture
Aerosmith frontman Steven Tyler was affected by Morton's neuroma and underwent surgery for it.[21] Near the end of the 2019 Major League Baseball season, Los Angeles Angels center fielder Mike Trout missed several September games before being scheduled for surgery to remove a Morton's neuroma in the ball of his right foot.[22]
In Season 1, Episode 18 of the Golden Girls, Dorothy requires an operation due to Morton’s neuroma.
References
- ↑ Bhatia, Maneesh; Thomson, Lauren (May 2020). "Morton's neuroma – Current concepts review". Journal of Clinical Orthopaedics and Trauma. 11 (3): 406–409. doi:10.1016/j.jcot.2020.03.024.
- 1 2 3 Rahman, Anisur; Giles, Ian (2020). "18. Rheumatology". In Feather, Adam; Randall, David; Waterhouse, Mona (eds.). Kumar and Clark's Clinical Medicine (10th ed.). Elsevier. p. 428. ISBN 978-0-7020-7870-5. Archived from the original on 2021-12-15. Retrieved 2021-12-13.
- ↑ "Thomas George Morton". Who Named It. Archived from the original on 2019-04-24. Retrieved 2019-03-03.
- ↑ Morton's Neuroma: Interdigital Perineural Fibrosis Archived 2019-04-01 at the Wayback Machine Wheeless' Textbook of Orthopaedics
- ↑ "What is Morton's Neuroma?". The Center for Morton's Neuroma. Archived from the original on 2019-10-18. Retrieved 2021-08-21.
- 1 2 "Cryosurgery for Morton's Neuroma, UK Clinic". Archived from the original on 2019-10-18. Retrieved 2022-03-14.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ Bencardino J, Rosenberg ZS, Beltran J, Liu X, Marty-Delfaut E (September 2000). "Morton's neuroma: is it always symptomatic?". American Journal of Roentgenology. 175 (3): 649–653. doi:10.2214/ajr.175.3.1750649. PMID 10954445.
{{cite journal}}: CS1 maint: uses authors parameter (link) - ↑ Gregg JM, Schneider T, Marks P (2008). "MR imaging and ultrasound of metatarsalgia--the lesser metatarsals". Radiological Clinics of North America. 46 (6): 1061–1078. doi:10.1016/j.rcl.2008.09.004. PMID 19038613.
- ↑ Gregg JM, Marks P (2007). "Metatarsalgia: an ultrasound perspective". Australasian Radiology. 51 (6): 493–499. doi:10.1111/j.1440-1673.2007.01886.x. PMID 17958682.
- ↑ Reed, RJ; Bliss, BO (February 1973). "Morton's neuroma. Regressive and productive intermetatarsal elastofibrositis". Archives of Pathology. 95 (2): 123–129. PMID 4118941.
- ↑ Scotti, TM (January 1957). "The lesion of Morton's metatarsalgia (Morton's toe)". AMA Archives of Pathology. 63 (1): 91–102. PMID 13381291.
- 1 2 "The Center for Morton's Neuroma". Archived from the original on 2019-07-25. Retrieved 2021-08-21.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 Chuter GS1, Chua YP, Connell DA, Blackney MC. (January 2013). "Ultrasound guided radiofrequency ablation in the management of interdigital (Morton's) neuroma". Skeletal Radiol. 42 (1): 107–11. doi:10.1007/s00256-012-1527-x. PMID 23073898. S2CID 25166343.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - 1 2 Hughes RJ, Ali K, Jones H, Kendall S, Connell DA (June 2007). "Treatment of Morton's neuroma with alcohol injection under sonographic guidance: follow-up of 101 cases". Acta Orthop Belg. 188 (6): 1535–9. doi:10.2214/AJR.06.1463. PMID 17515373.
- ↑ Matthews, Barry G.; Hurn, Sheree E.; Harding, Michael P.; Henry, Rachel A.; Ware, Robert S. (13 February 2019). "The effectiveness of non-surgical interventions for common plantar digital compressive neuropathy (Morton's neuroma): a systematic review and meta-analysis". Journal of Foot and Ankle Research. 12 (12): 1–21. doi:10.1186/s13047-019-0320-7. ISSN 1757-1146. PMC 6375221. PMID 30809275.
- ↑ "Morton's neuroma". www.nhs.uk. NHS choices. Archived from the original on 12 August 2015. Retrieved 15 March 2016.
- ↑ "Cryosurgery Or Sclerosing Injections: Which Is Better For Neuromas?". Archived from the original on 2019-03-06. Retrieved 2021-08-21.
- ↑ A Caporusso EF, Fallat LM, Savoy-Moore R (Sep–Oct 2002). "Cryogenic Neuroablation for the treatment of lower extremity neuromas". J Foot Ankle Surg. 41 (5): 286–290. doi:10.1016/S1067-2516(02)80046-1. PMID 12400711. Archived from the original on 2012-05-10. Retrieved 2021-08-21.
- ↑ Musson RE1, Sawhney JS, Lamb L, Wilkinson A, Obaid H. (March 2012). "Ultrasound guided alcohol ablation of Morton's neuroma". Foot & Ankle International. 33 (3): 196–201. doi:10.3113/fai.2012.0196. PMID 22734280.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Talia Friedman, MD, Daniel Richman, MD and Ronald Adler, MD (2012). "Sonographically Guided Cryoneurolysis Preliminary Experience and Clinical Outcomes". J Ultrasound Med. 31 (12): 2025–2034. doi:10.7863/jum.2012.31.12.2025. PMID 23197557. Archived from the original on 2019-12-16. Retrieved 2021-08-21.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ "Steven Tyler Q&A: On Making 'Noise in My Head,' Aerosmith & 'Idol,' Johnny Depp & More". Archived from the original on 2019-03-07. Retrieved 2021-08-21.
- ↑ "Trout to have surgery for nerve issue in foot". ESPN.com. September 15, 2019. Archived from the original on September 22, 2019. Retrieved September 15, 2019.
External links
| Classification | |
|---|---|
| External resources |