Pulmonary hypoplasia
| Pulmonary hypoplasia | |
|---|---|
| Other names: Familial primary pulmonary hypoplasia | |
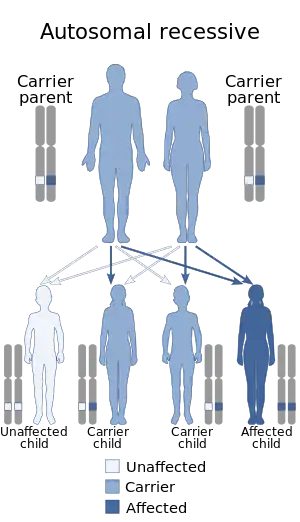 | |
| This condition is inherited in an autosomal recessive manner | |
| Specialty | Pulmonology |
Pulmonary hypoplasia is incomplete development of the lungs, resulting in an abnormally low number or small size of bronchopulmonary segments or alveoli. A congenital malformation, it most often occurs secondary to other fetal abnormalities that interfere with normal development of the lungs. Primary (idiopathic) pulmonary hypoplasia is rare and usually not associated with other maternal or fetal abnormalities.
Incidence of pulmonary hypoplasia ranges from 9–11 per 10,000 live births and 14 per 10,000 births.[1] Pulmonary hypoplasia is a relatively common cause of neonatal death.[2] It also is a common finding in stillbirths, although not regarded as a cause of these.
Signs and symptoms
The presentation of pulmonary hypoplasia is consistent with the following:[3]
- Mild/severe respiratory insufficiency
- Decreased fetal movement
Causes
Causes of pulmonary hypoplasia include a wide variety of congenital malformations and other conditions in which pulmonary hypoplasia is a complication.[1] These include congenital diaphragmatic hernia, congenital cystic adenomatoid malformation, fetal hydronephrosis, caudal regression syndrome, mediastinal tumor, and sacrococcygeal teratoma with a large component inside the fetus.[4][5][6][7] Large masses of the neck (such as cervical teratoma) also can cause pulmonary hypoplasia, presumably by interfering with the fetus's ability to fill its lungs. In the presence of pulmonary hypoplasia, the EXIT procedure to rescue a baby with a neck mass is not likely to succeed.[8]
Fetal hydrops can be a cause,[9] or conversely a complication.[10]
Pulmonary hypoplasia is associated with oligohydramnios through multiple mechanisms. Both conditions can result from blockage of the urinary bladder. Blockage prevents the bladder from emptying, and the bladder becomes very large and full. The large volume of the full bladder interferes with normal development of other organs, including the lungs. Pressure within the bladder becomes abnormally high, causing abnormal function in the kidneys hence abnormally high pressure in the vascular system entering the kidneys. This high pressure also interferes with normal development of other organs. An experiment in rabbits showed that PH also can be caused directly by oligohydramnios.[11]
Pulmonary hypoplasia is associated with dextrocardia of embryonic arrest in that both conditions can result from early errors of development, resulting in Congenital cardiac disorders.
PH is a common direct cause of neonatal death resulting from pregnancy induced hypertension.[12]
Diagnosis

Medical diagnosis of pulmonary hypoplasia in utero may use imaging, usually ultrasound or MRI.[13][14] The extent of hypoplasia is a very important prognostic factor.[15] One study of 147 fetuses (49 normal, 98 with abnormalities) found that a simple measurement, the ratio of chest length to trunk (torso) length, was a useful predictor of postnatal respiratory distress.[16] In a study of 23 fetuses, subtle differences seen on MRIs of the lungs were informative.[17] In a study of 29 fetuses with suspected pulmonary hypoplasia, the group that responded to maternal oxygenation had a more favorable outcome.[18]
Pulmonary hypoplasia is diagnosed also clinically.
Management
Management has three components: interventions before delivery, timing and place of delivery, and therapy after delivery.
In some cases, fetal therapy is available for the underlying condition; this may help to limit the severity of pulmonary hypoplasia. In exceptional cases, fetal therapy may include fetal surgery.[19][20]
A 1992 case report of a baby with a sacrococcygeal teratoma (SCT) reported that the SCT had obstructed the outlet of the urinary bladder causing the bladder to rupture in utero and fill the baby's abdomen with urine (a form of ascites). The outcome was good. The baby had normal kidneys and lungs, leading the authors to conclude that obstruction occurred late in the pregnancy and to suggest that the rupture may have protected the baby from the usual complications of such an obstruction.[21] Subsequent to this report, use of a vesicoamniotic shunting procedure (VASP) has been attempted, with limited success.[22][23][24]
Often, a baby with a high risk of pulmonary hypoplasia will have a planned delivery in a specialty hospital such as (in the United States) a tertiary referral hospital with a level 3 neonatal intensive-care unit. The baby may require immediate advanced resuscitation and therapy.[25]
Early delivery may be required in order to rescue the fetus from an underlying condition that is causing pulmonary hypoplasia. However, pulmonary hypoplasia increases the risks associated with preterm birth, because once delivered the baby requires adequate lung capacity to sustain life. The decision whether to deliver early includes a careful assessment of the extent to which delaying delivery may increase or decrease the pulmonary hypoplasia. It is a choice between expectant management and active management. An example is congenital cystic adenomatoid malformation with hydrops; impending heart failure may require a preterm delivery.[26] Severe oligohydramnios of early onset and long duration, as can occur with early preterm rupture of membranes, can cause increasingly severe PH; if delivery is postponed by many weeks, PH can become so severe that it results in neonatal death.[27]
After delivery, most affected babies will require supplemental oxygen. Some severely affected babies may be saved with extracorporeal membrane oxygenation (ECMO).[28] Not all specialty hospitals have ECMO, and ECMO is considered the therapy of last resort for pulmonary insufficiency.[29] An alternative to ECMO is high-frequency oscillatory ventilation.[30]
History
In 1908, Maude Abbott documented pulmonary hypoplasia occurring with certain defects of the heart.[31] In 1915, Abbott and J. C. Meakins showed that pulmonary hypoplasia was part of the differential diagnosis of dextrocardia.[32] In 1920, decades before the advent of prenatal imaging, the presence of pulmonary hypoplasia was taken as evidence that diaphragmatic hernias in babies were congenital, not acquired.[33]
See also
References
- 1 2 Cadichon, Sandra B. (2007), "Chapter 22: Pulmonary hypoplasia", in Kumar, Praveen; Burton, Barbara K. (eds.), Congenital malformations: evidence-based evaluation and management, archived from the original on 2023-11-13, retrieved 2023-10-31
- ↑ Pinar H (August 2004). "Postmortem findings in term neonates". Seminars in Neonatology. 9 (4): 289–302. doi:10.1016/j.siny.2003.11.003. PMID 15251146.
- ↑ Tisekar, Owais R.; Ak, Ajith Kumar (2023). "Hypoplastic Lung Disease". StatPearls. StatPearls Publishing. Archived from the original on 2022-12-18. Retrieved 2023-11-10.
- ↑ Walton JM, Rubin SZ, Soucy P, Benzie R, Ash K, Nimrod C (September 1993). "Fetal tumors associated with hydrops: the role of the pediatric surgeon". Journal of Pediatric Surgery. 28 (9): 1151–3. doi:10.1016/0022-3468(93)90152-b. PMID 8308682.
- ↑ Seo T, Ando H, Watanabe Y, Harada T, Ito F, Kaneko K, Mimura S (November 1999). "Acute respiratory failure associated with intrathoracic masses in neonates". Journal of Pediatric Surgery. 34 (11): 1633–7. doi:10.1016/s0022-3468(99)90632-2. PMID 10591558.
- ↑ Goto M, Makino Y, Tamura R, Ikeda S, Kawarabayashi T (2000). "Sacrococcygeal teratoma with hydrops fetalis and bilateral hydronephrosis". Journal of Perinatal Medicine. 28 (5): 414–8. doi:10.1515/JPM.2000.054. PMID 11125934. S2CID 23998257.
- ↑ Merello E, De Marco P, Mascelli S, Raso A, Calevo MG, Torre M, Cama A, Lerone M, Martucciello G, Capra V (March 2006). "HLXB9 homeobox gene and caudal regression syndrome". Birth Defects Research. Part A, Clinical and Molecular Teratology. 76 (3): 205–9. doi:10.1002/bdra.20234. PMID 16498628.
- ↑ Liechty KW, Hedrick HL, Hubbard AM, Johnson MP, Wilson RD, Ruchelli ED, Howell LJ, Crombleholme TM, Flake AW, Adzick NS (January 2006). "Severe pulmonary hypoplasia associated with giant cervical teratomas". Journal of Pediatric Surgery. 41 (1): 230–3. doi:10.1016/j.jpedsurg.2005.10.081. PMID 16410139.
- ↑ Kaiser L, Arany A, Veszprémi B, Vizer M (March 2007). "[Hydrops fetalis--a retrospective study]". Orvosi Hetilap (in magyar). 148 (10): 457–63. doi:10.1556/OH.2007.27951. PMID 17350912.
- ↑ Zembala-Nozyńska E, Oslislo A, Zajecki W, Kamiński K, Radzioch J (2005). "[Mediastinal tumor as a cause of fetal hydrops]". Wiadomości Lekarskie (in polski). 58 (7–8): 462–5. PMID 16425805.
- ↑ Yoshimura S, Masuzaki H, Miura K, Hayashi H, Gotoh H, Ishimaru T (July 1997). "The effects of oligohydramnios and cervical cord transection on lung growth in experimental pulmonary hypoplasia in rabbits". American Journal of Obstetrics and Gynecology. 177 (1): 72–7. doi:10.1016/s0002-9378(97)70440-x. PMID 9240585.
- ↑ Zhou X, Du X (July 1997). "[Analysis of the causes of neonatal deaths at term in pregnancy induced hypertension patients]". Zhonghua Fu Chan Ke Za Zhi (in 中文). 32 (7): 409–11. PMID 9639726.
- ↑ Quinn TM, Hubbard AM, Adzick NS (April 1998). "Prenatal magnetic resonance imaging enhances fetal diagnosis". Journal of Pediatric Surgery. 33 (4): 553–8. doi:10.1016/s0022-3468(98)90315-3. PMID 9574750.
- ↑ Kasprian G, Balassy C, Brugger PC, Prayer D (February 2006). "MRI of normal and pathological fetal lung development". European Journal of Radiology. 57 (2): 261–70. doi:10.1016/j.ejrad.2005.11.031. PMID 16413987.
- ↑ Lally KP, Lally PA, Lasky RE, Tibboel D, Jaksic T, Wilson JM, Frenckner B, Van Meurs KP, Bohn DJ, Davis CF, Hirschl RB (September 2007). "Defect size determines survival in infants with congenital diaphragmatic hernia". Pediatrics. 120 (3): e651–7. doi:10.1542/peds.2006-3040. PMID 17766505. S2CID 21529283.
- ↑ Ishikawa S, Kamata S, Usui N, Sawai T, Nose K, Okada A (May 2003). "Ultrasonographic prediction of clinical pulmonary hypoplasia: measurement of the chest/trunk-length ratio in fetuses". Pediatric Surgery International. 19 (3): 172–5. doi:10.1007/s00383-002-0912-2. PMID 12687395. S2CID 12453659.
- ↑ Kuwashima S, Nishimura G, Iimura F, Kohno T, Watanabe H, Kohno A, Fujioka M (September 2001). "Low-intensity fetal lungs on MRI may suggest the diagnosis of pulmonary hypoplasia". Pediatric Radiology. 31 (9): 669–72. doi:10.1007/s002470100512. PMID 11512012. S2CID 24016373.
- ↑ Broth RE, Wood DC, Rasanen J, Sabogal JC, Komwilaisak R, Weiner S, Berghella V (October 2002). "Prenatal prediction of lethal pulmonary hypoplasia: the hyperoxygenation test for pulmonary artery reactivity". American Journal of Obstetrics and Gynecology. 187 (4): 940–5. doi:10.1067/mob.2002.127130. PMID 12388982.
- ↑ Evans MI, Harrison MR, Flake AW, Johnson MP (October 2002). "Fetal therapy". Best Practice & Research. Clinical Obstetrics & Gynaecology. 16 (5): 671–83. doi:10.1053/beog.2002.0331. PMID 12475547.
- ↑ Menon P, Rao KL (May 2005). "Current status of fetal surgery". Indian Journal of Pediatrics. 72 (5): 433–6. doi:10.1007/bf02731743. PMID 15973028. S2CID 19578605.
- ↑ Zaninovic AC, Westra SJ, Hall TR, Sherman MP, Wong L, Boechat MI (1992). "Congenital bladder rupture and urine ascites secondary to a sacrococcygeal teratoma". Pediatric Radiology. 22 (7): 509–11. doi:10.1007/bf02012995. PMID 1491908. S2CID 42647757.
- ↑ Lewis KM, Pinckert TL, Cain MP, Ghidini A (May 1998). "Complications of intrauterine placement of a vesicoamniotic shunt". Obstetrics and Gynecology. 91 (5 Pt 2): 825–7. doi:10.1016/s0029-7844(97)00693-5. PMID 9572177. S2CID 29058662.
- ↑ Makino Y, Kobayashi H, Kyono K, Oshima K, Kawarabayashi T (January 2000). "Clinical results of fetal obstructive uropathy treated by vesicoamniotic shunting". Urology. 55 (1): 118–22. doi:10.1016/S0090-4295(99)00403-3. PMID 10654907.
- ↑ Makin EC, Hyett J, Ade-Ajayi N, Patel S, Nicolaides K, Davenport M (February 2006). "Outcome of antenatally diagnosed sacrococcygeal teratomas: single-center experience (1993-2004)". Journal of Pediatric Surgery. 41 (2): 388–93. doi:10.1016/j.jpedsurg.2005.11.017. PMID 16481257.
- ↑ Diana W. Bianchi; Timothy M. Crombleholme; Mary E. D'Alton (2000). Fetology: diagnosis & management of the fetal patient. McGraw-Hill Professional. p. 1081. ISBN 978-0-8385-2570-8.
- ↑ Bruner JP, Jarnagin BK, Reinisch L (2000). "Percutaneous laser ablation of fetal congenital cystic adenomatoid malformation: too little, too late?". Fetal Diagnosis and Therapy. 15 (6): 359–63. doi:10.1159/000021037. PMID 11111218. S2CID 2303014.
- ↑ Carroll SG, Blott M, Nicolaides KH (July 1995). "Preterm prelabor amniorrhexis: outcome of live births". Obstetrics and Gynecology. 86 (1): 18–25. doi:10.1016/0029-7844(95)00085-6. PMID 7784017. S2CID 22292146.
- ↑ Muratore CS, Wilson JM (December 2000). "Congenital diaphragmatic hernia: where are we and where do we go from here?". Seminars in Perinatology. 24 (6): 418–28. doi:10.1053/sper.2000.21111. PMID 11153903.
- ↑ Thibeault DW, Haney B (February 1998). "Lung volume, pulmonary vasculature, and factors affecting survival in congenital diaphragmatic hernia". Pediatrics. 101 (2): 289–95. doi:10.1542/peds.101.2.289. PMID 9445506.
- ↑ Azarow K, Messineo A, Pearl R, Filler R, Barker G, Bohn D (March 1997). "Congenital diaphragmatic hernia--a tale of two cities: the Toronto experience". Journal of Pediatric Surgery. 32 (3): 395–400. doi:10.1016/s0022-3468(97)90589-3. PMID 9094001.
- ↑ Abbott, Maude (1908), "Chapter IX: Congenital cardiac disease", in Osler, William (ed.), Modern Medicine: Its Theory and Practice, vol. IV: Diseases of the circulatory system, diseases of the blood, diseases of the spleen, thymus, and lymph-glands, Philadelphia and New York: Lea & Febiger, archived from the original on 2023-11-13, retrieved 2023-10-31
- ↑ M. E. Abbott; J. C. Meakins (1915). "On the differentiation of two forms of congenital dextrocardia". Bulletin of the International Association of Medical Museums (5): 134–138.
- ↑ Elmer H. Funk; W. F. Manges (1920). "Eventration of the diaphragm with report of a case". Transactions of the Association of American Physicians. 35: 138–143. Archived from the original on 2023-11-13. Retrieved 2023-10-31.
External links
| Classification | |
|---|---|
| External resources |