Prostatectomy
| Prostatectomy | |
|---|---|
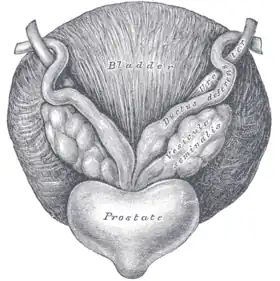 Anatomy of the prostate | |
| ICD-9-CM | 60.2–60.6 |
| MeSH | D011468 |
Prostatectomy (from the Greek προστάτης prostátēs, "prostate" and ἐκτομή ektomē, "excision") as a medical term refers to the surgical removal of all or part of the prostate gland. This operation is done for benign conditions that cause urinary retention, as well as for prostate cancer and for other cancers of the pelvis.
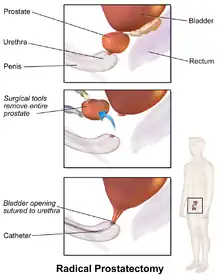
There are two main types of prostatectomies. A simple prostatectomy (also known as a subtotal prostatectomy) involves the removal of only part of the prostate. Surgeons typically carry out simple prostatectomies only for benign conditions.[1] A radical prostatectomy, the removal of the entire prostate gland, the seminal vesicles and the vas deferens, is performed for malignant cancer.[2]
There are multiple ways the operation can be done: with open surgery (via a large incision through the lower abdomen), laparoscopically with the help of a robot (a type of minimally invasive surgery), through the urethra or through the perineum.
Other terms that can be used to describe a prostatectomy include:
- Nerve-sparing: the blood vessels and nerves that promote penile erections are left behind in the body and not taken out with the prostate.
- Limited pelvic lymph node dissection: the lymph nodes surrounding and close to the prostate are taken out (typically the area defined by external iliac vein anteriorly, the obturator nerve posteriorly, the origin of the internal iliac artery proximally, Cooper's ligament distally, the bladder medially and the pelvic side wall laterally).[3]
- Extended pelvic lymph node dissection (PLND): lymph nodes farther away from the prostate are taken out also (typically the area defined in a limited PLND with the posterior boundary as the floor of the pelvis).[3]
Medical uses

Benign
Indications for removal of the prostate in a benign setting include acute urinary retention, recurrent urinary tract infections, uncontrollable hematuria, bladder stones secondary to bladder outlet obstruction, significant symptoms from bladder outlet obstruction that are refractory to medical or minimally invasive therapy, and chronic kidney disease secondary to chronic bladder outlet obstruction.[4]
Malignant
A radical prostatectomy is performed due to malignant cancer. For prostate cancer, the best treatment often depends on the risk level presented by the disease. For most prostate cancers classified as 'very low risk' and 'low risk,' radical prostatectomy is one of several treatment options; others include radiation, watchful waiting, and active surveillance. For intermediate and high risk prostate cancers, radical prostatectomy is often recommended in addition to other treatment options. Radical prostatectomy is not recommended in the setting of known metastases when the cancer has spread through the prostate, to the lymph nodes or other parts of the body.[5] Prior to decision making about the best treatment option for higher risk cancers, imaging studies using CT, MRI or bone scans are done to make sure the cancer has not spread outside of the prostate.
Contraindications
These would be same as the contraindications for any other surgery.
Techniques and approaches
There are several ways a prostatectomy can be done:
Open
In an open prostatectomy, the prostate is accessed through a large single incision through either the lower abdomen or the perineum. Further descriptive terms describe how the prostate is accessed anatomically through this incision (retropubic vs. suprapubic vs. perineal). A retropubic prostatectomy describes a procedure that accesses the prostate by going through the lower abdomen and behind the pubic bone. A suprapubic prostatectomy describes a procedure cuts through the lower abdomen and through the bladder to access the prostate. A perineal prostatectomy is done by making an incision between the rectum and scrotum on the underside of the abdomen.
Minimally invasive
Robotic-assisted instruments are inserted through several small abdominal incisions and controlled by a surgeon. Some use the term 'robotic' for short, in place of the term 'computer-assisted'. However, procedures performed with a computer-assisted device are performed by a surgeon, not a robot. The computer-assisted device gives the surgeon more dexterity and better vision, but no tactile feedback compared to conventional laparoscopy. When performed by a surgeon who is specifically trained and well experienced in computer-assisted laparoscopy (CALP), there can be similar advantages over open prostatectomy, including smaller incisions, less pain, less bleeding, less risk of infection, faster healing time, and shorter hospital stay.[6][7] The cost of this procedure is higher, while long-term functional and oncological superiority have yet to be established.[8][9][10]
Risks and complications
Complications that occur in the period right after any surgical procedure, including a prostatectomy, include a risk of bleeding, a risk of infection at the site of incision or throughout the whole body, a risk of a blood clot occurring in the leg or lung, a risk of a heart attack or stroke, and a risk of death.
Severe irritation takes place if a latex catheter is inserted in the urinary tract of a person allergic to latex. That is especially severe in case of a radical prostatectomy due to the open wound there and the exposure lasting e.g. two weeks. Intense pain may indicate such situation.[11]
Men can experience changes in their sexual responses after radical prostatectomy, including impairments to sexual desire, penile morphology and orgasmic function.[12][13] A 2005 article in the medical journal Reviews in Urology listed the incidence of several complications following radical prostatectomy: mortality <0.3%, impotence >50%, ejaculatory dysfunction 100%, orgasmic dysfunction 50%, incontinence <5–30%, pulmonary embolism <1%, rectal injury <1%, urethral stricture <5%, and transfusion 20%.[14]
Erectile dysfunction
Surgical removal of the prostate contains an increased likelihood that patients will experience erectile dysfunction. Radical prostatectomy is associated with greater decrease in sexual function than external beam radiotherapy. Nerve-sparing surgery reduces the risk that patients will experience erectile dysfunction. However, the experience and the skill of the nerve-sparing surgeon, as well as any surgeon are critical determinants of the likelihood of positive erectile function of the patient.[15]
Following a prostatectomy, patients will not be able to ejaculate semen due to the nature of the procedure, resulting in the permanent necessity of assisted reproductive techniques in case of desires of future fertility.[16] Preservation of normal ejaculation is possible after TUR prostatectomy, open or laser enucleation of adenoma and laser vaporisation of prostate. However, retrograde ejaculation is a common problem. Preservation of ejaculation is the aim of some new techniques.[17] Once the prostate and vesicles are removed, even if partial erection is achieved, ejaculation is a very different experience, with little of the compulsive release that is common to ejaculation with those organs intact.
Urinary incontinence
Prostatectomy patients have an increased risk of leaking small amounts of urine immediately after surgery, and for the long-term, often requiring urinary incontinence devices such as condom catheters or diaper pads. A large analysis of the incidence of urinary incontinence found that 12 months after surgery, 75% of patients needed no pad, while 9–16% did. Factors associated with increased risk of long-term urinary incontinence include older age, higher BMI, more comorbidities, larger prostates surgically excised, as well as experience and technique of the surgeon.[18]
Surgical management options for urinary incontinence secondary to prostatectomy include implantation of perineal slings and artificial urinary sphincters.[19] Although there are limited data on the long-term outcomes in males, perineal slings are offered for mild-to-moderate post-prostatectomy incontinence.[20][21] In a retrospective study the success rate of perineal sling placement in urinary incontinence following prostatectomy achieved 86% at a median follow-up of 22 months.[22] Artificial urinary sphincters are offered for moderate-to-severe urinary incontinence in males and have shown good long-term efficacy and safety.[21][20][23][24] The use of artificial urinary sphincters for post-prostatectomy incontinence is supported by the recommendations of European Association of Urology and International Consultation on Incontinence.[20][21]
Transurethral injection of bulking agents have little role in the management of post-prostatecromy incontinence and there is weak evidence that these agents can offer any improvement.[20][21] Pelvic floor muscle training can speed recovery of urinary incontinence following prostatectomy.[21]
Remedies to post-operative sexual dysfunction
Very few surgeons will claim that patients return to the erectile experience they had prior to surgery. The rates of erectile recovery that surgeons often cite are qualified by the addition of sildenafil to the recovery regimen.[25]
Remedies to the problem of post-operative sexual dysfunction include:[26]
Epidemiology
The use of radical prostatectomy as treatment for prostate cancer increased significantly from 1980 to 1990.[27] As of 2000, the median age of men undergoing radical prostatectomy for localized prostate cancer was 62.[27]
Though a very common procedure, the experience level of the surgeon performing the operation is important in determining the outcomes, rate of complications, and side effects. The more prostatectomies performed by a surgeon, the better the outcomes. This is true for prostatectomies done as open procedures[28] and those done using minimally invasive techniques.[29]
History
William Belfield, MD is generally credited for performing the first intentional prostatectomy via the suprapubic route in 1885, 1886 or 1887 at Cook County Hospital in Chicago.[30][31] Hugh H. Young MD in collaboration with William Stewart Halsted MD developed the open, radical and perineal prostatectomies in 1904 at Johns Hopkins Brady Urological Institute, the first version of the procedure that became generally feasible.[32] The Irish surgeon Terence Millin, MD (1903–1980) developed the radical retropubic prostatectomy in 1945.[33] American urologist Patrick C. Walsh, MD (1938—present) developed the modern nerve-sparing, retropubic prostatectomy with minimal blood loss.[34] The first laparoscopic prostatectomy was performed in 1991 by William Schuessler, MD and colleagues in Texas.[35]
Costs
A 2014 survey of prostatectomy fees for uninsured patients at 70 United States hospitals found an average facility fee of $34,720 and average surgeon and anesthesiologist fees of $8,280.[36]
See also
- List of surgeries by type
References
- ↑ Khera, Mohit (October 23, 2013). "Simple Prostatectomy". Medscape. Retrieved November 8, 2014.
- ↑ McAninch, Jack W. (2008). Smith and Tanagho's General Urology. New York: McGraw Hill Medical. p. 368. ISBN 978-0-07-162497-8.
- 1 2 Wider, Jeff A. (2014). Pocket Guide to Urology. pp. 141–142. ISBN 978-0-9672845-6-9.
- ↑ Khera, Mohit (October 23, 2013). "Simple Prostatectomy". Medscape. Retrieved November 13, 2014.
- ↑ "NCCN Guidelines version 1.2015 – Prostate Cancer" (PDF). NCCN Guidelines. National Comprehensive Cancer Network. October 24, 2014. Retrieved November 13, 2014.
- ↑ Center for the Advancement of Health; August 29, 2005; Robot-assisted Prostate Surgery Has Possible Benefits, High Cost
- ↑ O’Neil, Brock; Koyama, Tatsuki; Alvarez, JoAnn; Conwill, Ralph M.; Albertsen, Peter C.; Cooperberg, Matthew R.; Goodman, Michael; Greenfield, Sheldon; Hamilton, Ann S.; Hoffman, Karen E.; Hoffman, Richard M. (2016). "The Comparative Harms of Open and Robotic Prostatectomy in Population Based Samples". Journal of Urology. 195 (2): 321–329. doi:10.1016/j.juro.2015.08.092. ISSN 0022-5347. PMC 4916911. PMID 26343985.
- ↑ Cost Analysis of Radical Retropubic, Perineal, and Robotic Prostatectomy; Scott V. Burgess, Fatih Atug, Erik P. Castle, Rodney Davis, Raju Thomas; Journal of Endourology 2006 20:10, 827–830
- ↑ Bolenz, C.; Gupta, A.; Hotze, T.; Ho, R.; Cadeddu, J.; Roehrborn, C.; Lotan, Y. (2010). "Cost comparison of robotic, laparoscopic, and open radical prostatectomy for prostate cancer". European Urology. 57 (3): 453–458. doi:10.1016/j.eururo.2009.11.008. PMID 19931979.
- ↑ Barocas, D. A.; Salem, S.; Kordan, Y.; Herrell, S. D.; Chang, S. S.; Clark, P. E.; Davis, R.; Baumgartner, R.; Phillips, S.; Cookson, M. S.; Smith Jr, J. A. (2010). "Robotic Assisted Laparoscopic Prostatectomy Versus Radical Retropubic Prostatectomy for Clinically Localized Prostate Cancer: Comparison of Short-Term Biochemical Recurrence-Free Survival". The Journal of Urology. 183 (3): 990–996. doi:10.1016/j.juro.2009.11.017. PMID 20083261.
- ↑ "Radical Prostatectomy".
- ↑ Levin, R. J. (2018). "Prostate-induced orgasms: A concise review illustrated with a highly relevant case study". Clinical Anatomy. 31 (1): 81–85. doi:10.1002/ca.23006. PMID 29265651.
- ↑ Wehrwein, Peter; Harvard Prostate Knowledge (15 October 2013). "Achieving orgasm after radical prostatectomy". Harvard Health Publishing.
- ↑ Sexual Dysfunction after Radical Prostatectomy; Andrew R McCullough; Reviews in Urology; 2005 7:(Suppl 2), S3–S10.
- ↑ John P. Mulhall, M.D., Saving Your Sex Life: A Guide for Men with Prostate Cancer, Chicago, Hilton Publishing Company, 2008, pp. 56, 58, Table 1: Factors Predicting Erectile Function Recovery after Radical Prostatectomy, p. 65.
- ↑ Tran, Stéphanie; Boissier, Romain; Perrin, Jeanne; Karsenty, Gilles; Lechevallier, Eric (2015). "Review of the Different Treatments and Management for Prostate Cancer and Fertility". Urology. 86 (5): 936–941. doi:10.1016/j.urology.2015.07.010. PMID 26368508.
- ↑ Alloussi, Saladin Helmut; Lang, Christoph; Eichel, Robert; Alloussi, Schahnaz (2013-08-19). "Ejaculation-Preserving Transurethral Resection of Prostate and Bladder Neck: Short- and Long-Term Results of a New Innovative Resection Technique". Journal of Endourology. 28 (1): 84–89. doi:10.1089/end.2013.0093. ISSN 0892-7790. PMID 23952037.
- ↑ Ficarra, Vincenzo; Novara, Giacomo; Rosen, Raymond C.; Artibani, Walter; Carroll, Peter R.; Costello, Anthony; Menon, Mani; Montorsi, Francesco; Patel, Vipul R. (September 2012). "Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy". European Urology. 62 (3): 405–417. doi:10.1016/j.eururo.2012.05.045. ISSN 1873-7560. PMID 22749852.
- ↑ Kretschmer, Alexander; Nitti, Victor (October 2017). "Surgical Treatment of Male Postprostatectomy Incontinence: Current Concepts". European Urology Focus. 3 (4–5): 364–376. doi:10.1016/j.euf.2017.11.007. PMID 29174616.
- 1 2 3 4 Averbeck, Marcio A.; Woodhouse, Christopher; Comiter, Craig; Bruschini, Homero; Hanus, Thomas; Herschorn, Sender; Goldman, Howard B. (23 October 2018). "Surgical treatment of post-prostatectomy stress urinary incontinence in adult men: Report from the 6th International Consultation on Incontinence". Neurourology and Urodynamics. 38 (1): 398–406. doi:10.1002/nau.23845. PMID 30350875. S2CID 53039893.
- 1 2 3 4 5 Burkhard, F.C.; Bosch, J.L.H.R.; Cruz, F.; Lemack, G.E.; Nambiar, A.K.; Thiruchelvam, N.; Tubaro, A. (2018). EAU Guidelines on Urinary Incontinence in Adults (PDF). Arnhem, The Netherlands: European Association of Urology. ISBN 978-94-92671-01-1. Retrieved 21 January 2020.
- ↑ Siracusano, Salvatore; Visalli, Francesco; Favro, Michele; Tallarigo, Carlo; Kugler, Mauro; Kugler, Alexander; Diminutto, Alberto; Talamini, Renato; Artibani, Walter (13 September 2017). "Argus-T Sling in 182 Male Patients: Short-Term Results of a Multicenter Study". Urology. 110: 177–183. doi:10.1016/j.urology.2017.07.058. PMID 28917606. Retrieved 21 January 2020.
- ↑ Haab, Francois; Trockman, Brett A.; Zimmern, Philippe E.; Leach, Gary E. (1 August 1997). "Quality of life and continence assessment of the artificial urinary sphincter in men with minimum 3.5 years of followup". Journal of Urology. 158 (2): 435–439. doi:10.1016/S0022-5347(01)64496-3. PMID 9224318. Retrieved 21 January 2020.
- ↑ Llorens, Christophe; Pottek, Tobias (25 October 2017). "Urinary artificial sphincter ZSI 375 for treatment of stress urinary incontinence in men: 5 and 7 years follow-up report". Urologia Journal. 84 (4): 263–266. doi:10.5301/uj.5000243. PMID 28525665.
- ↑ John P. Mulhall, M.D., Saving Your Sex Life: A Guide for Men with Prostate Cancer, Chicago, Hilton Publishing Company, 2008, p. 69.
- ↑ John P. Mulhall, M.D., Saving Your Sex Life: A Guide for Men with Prostate Cancer, Chicago, Hilton Publishing Company, 2008
- 1 2 Moul, J. W. (August 2002). "Epidemiology of radical prostatectomy for localized prostate cancer in the era of prostate-specific antigen: an overview of the Department of Defense Center for Prostate Disease Research national database". Surgery. 132 (2): 213–9. doi:10.1067/msy.2002.125315. PMID 12219014.
- ↑ Vickers, A., Bianco, F., Cronin, A., Eastham, J., Klein, E., Kattan, M., Scardino, P. (April 2010). "The learning curve for surgical margins after open radical prostatectomy: implications for margin status as an oncological end point". Journal of Urology. 183 (4): 1360–5. doi:10.1016/j.juro.2009.12.015. PMC 2861336. PMID 20171687.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Vickers, A. J., Savage C. J, Hruza, M., Tuerk, I., Koenig, P., Martínez-Piñeiro, L., Janetschek, G., Guillonneau, B. (May 2009). "The surgical learning curve for laparoscopic radical prostatectomy: a retrospective cohort study". Lancet Oncol. 10 (5): 475–80. doi:10.1016/S1470-2045(09)70079-8. PMC 2777762. PMID 19342300.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Thorndike, P (1903). "Present status of the surgery of prostate gland". Boston Med Surg J. 149 (7): 167–171. doi:10.1056/nejm190308131490701.
- ↑ Zorgniotti, AW (2012). "Suprapubic prostatectomy: An Anglo-American success story". In Hinman, Jr, F; Boyarsky, S (eds.). Benign Prostatic Hypertrophy. Spring. pp. 45–58. ISBN 978-1-4612-5478-2.
- ↑ Young, HH (1905). "VIII. Conservative perineal prostatectomy: The results of two years' experience and report of seventy-five cases" (PDF). Ann Surg. 41 (4): 549–557. doi:10.1097/00000658-190504000-00006. PMC 1426005. PMID 17861622. Archived from the original (PDF) on 2016-05-30. Retrieved 2018-01-21.
- ↑ Millin, T (1945). "Retropubic prostatectomy: A new extravesical technique report; report of 20 cases". Lancet. 2 (6380): 693–696. doi:10.1016/S0140-6736(45)91030-0. PMID 21007347.
- ↑ Walsh, PC (2007). "The discovery of the cavernous nerves and development of nerve sparing radical retropubic prostatectomy". J Urol. 177 (5): 1632–1635. doi:10.1016/j.juro.2007.01.012. PMID 17437775.
- ↑ Schuessler, WW; Schulam, PG; Clayman, RV; Kavoussi, LR (1997). "Laparoscopic radical prostatectomy: Initial short-term experience". Urology. 50 (6): 854–857. doi:10.1016/s0090-4295(97)00543-8. PMID 9426713.
- ↑ Pate, S. C., Uhlman, M. A., Rosenthal, J. A., Cram, P., Erickson, B. A. (March 2014). "Variations in the open market costs for prostate cancer surgery: a survey of US hospitals". Urology. 83 (3): 626–30. doi:10.1016/j.urology.2013.09.066. PMID 24439795.
{{cite journal}}: CS1 maint: multiple names: authors list (link)
External links
- The Basics of the Prostatectomy Procedure Explained
- Prostatectomy – slideshow by The New York Times