Risk factors for tuberculosis
There are a number risk factors for tuberculosis infection; worldwide the most important of these is HIV. Co-infection with HIV is a particular problem in Sub-Saharan Africa, due to the high incidence of HIV in these countries.[1][2] Smoking more than 20 cigarettes a day increases the risk of TB by two to four times[3] while silicosis increases the risk about 30 fold.[4] Diabetes mellitus is also an important risk factor that is growing in importance in developing countries.[5] Other disease states that increase the risk of developing tuberculosis are Hodgkin lymphoma, end-stage renal disease, chronic lung disease, malnutrition, and alcoholism.[6] A person's genetics also play a role.[7]
Silicosis
People with silicosis have an approximately 30-fold greater risk for developing TB.[4] Silica particles irritate the respiratory system, causing immunogenic responses such as phagocytosis, which results in high lymphatic vessel deposits.[8] It is probably this interference and blockage of macrophage function that increases the risk of tuberculosis.[9] Persons with chronic kidney failure and also on hemodialysis have an increased risk.[10] Given that silicosis greatly increases the risk of tuberculosis, more research about the effect of various indoor or outdoor air pollutants on the disease would be necessary. Some possible indoor sources of silica include paint, concrete, and Portland cement. Crystalline silica is found in concrete, masonry, sandstone, rock, paint, and other abrasives. The cutting, breaking, crushing, drilling, grinding, or abrasive blasting of these materials may produce fine silica dust. It can also be in soil, mortar, plaster, and shingles.[11]
Some drugs, including rheumatoid arthritis drugs that work by blocking tumor necrosis factor-alpha (an inflammation-causingcytokine), raise the risk of activating a latent infection due to the importance of this cytokine in the immune defense against TB.[12]
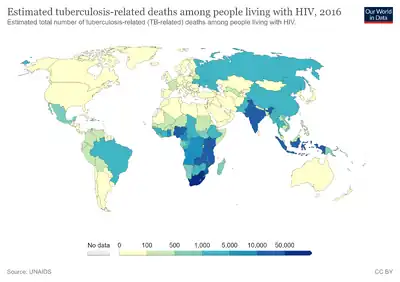
HIV
HIV is a major risk factor for tuberculosis. The risk of developing TB is estimated to be between 20 and 37 times greater in people living with HIV than among those without HIV infection. TB is a leading cause of morbidity and mortality among people living with HIV.[13] In 2009, there were 9.4 million new cases of TB, of which 1.2 (13%) million were among people living with HIV. Of the 1.7 million people who died of TB, 400,000 (24%) were living with HIV.[13]
Nutrition
Low body weight is associated with risk of tuberculosis. A body mass index (BMI) below 18.5 increases the risk by 2 to 3 times. An increase in body weight lowers the risk.[14] People with diabetes mellitus are at increased risk of contracting tuberculosis,[15] and they have a poorer response to treatment, possibly due to poorer drug absorption.[16]
Other clinical conditions that have been associated with active TB include gastrectomy with attendant weight loss and malabsorption, jejunoileal bypass, renal and cardiac transplantation, carcinoma of the head or neck, and other neoplasms (e.g., lung cancer, lymphoma, and leukemia).[4]
Diet may also modulate risk. For example, among immigrants in London from the Indian subcontinent, vegetarian Hindu Asians were found to have an 8.5 fold increased risk of tuberculosis, compared to Muslims who ate meat and fish daily.[17] Although a causal link is not proved by this data,[18] this increased risk could be caused by micronutrient deficiencies: possibly iron, vitamin B12 or vitamin D.[17] Further studies have provided more evidence of a link between vitamin D deficiency and an increased risk of contracting tuberculosis.[19][20] Globally, the severe malnutrition common in parts of the developing world causes a large increase in the risk of developing active tuberculosis, due to its damaging effects on the immune system.[21][22] Along with overcrowding, poor nutrition may contribute to the strong link observed between tuberculosis and poverty.[23][24]
Crowding
Prisoners are particularly vulnerable to infectious diseases such as HIV/AIDS and TB. Imprisonment facilities provide conditions that allow TB to spread rapidly due to overcrowding, poor nutrition, and a lack of health services. TB outbreaks have been reported in prisons and jails throughout the world, and is particularly concerning in the United States,[25] which incarcerates a larger proportion of its population than any other nation. The prevalence of TB in prisons is much higher than among the general population—in some countries as much as 40 times higher.[26][27]
Diabetes mellitus
There is also a very high 3 fold increased risk of infection with TB for patients who have diabetes mellitus.[28] Higher associations have been found between diabetes mellitus and TB in study populations from Central America, Europe, and Asia.[28] Developing countries with exponential economic growth such as India and China that account for 40% of incident TB cases in 2010 and are estimated to have a 69% increase in people with diabetes mellitus are of concern for the joint burden of disease between diabetes mellitus and tuberculosis.[28]
Other
Other conditions that increase risk include the sharing of needles among IV drug users, recent TB infection or a history of inadequately treated TB, chest X-ray suggestive of previous TB, showing fibrotic lesions and nodules, prolonged corticosteroid therapy and other immunosuppressive therapy, compromised immune system (30–40% of people with AIDS worldwide also have TB), hematologic and reticuloendothelial diseases, such as leukemia and Hodgkin's disease, end-stage kidney disease, intestinal bypass, chronic malabsorption syndromes, vitamin D deficiency,[29] and low body weight.[6][30] There is also genetic susceptibility.[7]
References
- ↑ World Health Organization. "Global tuberculosis control–surveillance, planning, financing WHO Report 2006". Archived from the original on 12 December 2006. Retrieved 13 October 2006.
- ↑ Chaisson, RE; Martinson, NA (2008-03-13). "Tuberculosis in Africa--combating an HIV-driven crisis". The New England Journal of Medicine. 358 (11): 1089–92. doi:10.1056/NEJMp0800809. PMID 18337598.
- ↑ Davies PD, Yew WW, Ganguly D, Davidow AL, Reichman LB, Dheda K, Rook GA (April 2006). "Smoking and tuberculosis: the epidemiological association and immunopathogenesis". Transactions of the Royal Society of Tropical Medicine and Hygiene. 100 (4): 291–8. doi:10.1016/j.trstmh.2005.06.034. PMID 16325875.
- 1 2 3 ATS/CDC Statement Committee on Latent Tuberculosis Infection (June 2000). "Targeted tuberculin testing and treatment of latent tuberculosis infection. American Thoracic Society". MMWR Recomm Rep. 49 (RR–6): 1–51. PMID 10881762. Archived from the original on 2004-12-17. Retrieved 2022-07-11.
- ↑ Restrepo, BI (2007-08-15). "Convergence of the tuberculosis and diabetes epidemics: renewal of old acquaintances". Clinical Infectious Diseases. 45 (4): 436–8. doi:10.1086/519939. PMC 2900315. PMID 17638190.
- 1 2 Kumar V, Abbas AK, Fausto N, Mitchell RN (2007). Robbins Basic Pathology (8th ed.). Saunders Elsevier. pp. 516–522. ISBN 978-1-4160-2973-1.
- 1 2 Möller, M; Hoal, EG (March 2010). "Current findings, challenges and novel approaches in human genetic susceptibility to tuberculosis". Tuberculosis (Edinburgh, Scotland). 90 (2): 71–83. doi:10.1016/j.tube.2010.02.002. PMID 20206579.
- ↑ Lee JH (1948). "Tuberculosis and Silicosis". Can Med Assoc J. 58 (4): 349–353. PMC 1591092. PMID 18916106.
- ↑ Varkey B (26 January 2011). "Silicosis". WebMD. Archived from the original on 17 July 2011. Retrieved 26 July 2011.
- ↑ Segall L, Covic A (June 2010). "Diagnosis of tuberculosis in dialysis patients: current strategy". Clin J Am Soc Nephrol. 5 (6): 1114–22. doi:10.2215/CJN.09231209. PMID 20413440. Archived from the original on 2022-07-14. Retrieved 2022-07-11.
- ↑ "NIOSH – Silicosis: Learn the Facts!". CDC.gov. 2004. doi:10.26616/NIOSHPUB2004108. Archived from the original on 8 March 2010. Retrieved 13 April 2010.
- ↑ Mutlu G, Mutlu E, Bellmeyer A, Rubinstein I (2006). "Pulmonary adverse events of anti-tumor necrosis factor-alpha antibody therapy". Am J Med. 119 (8): 639–46. doi:10.1016/j.amjmed.2006.01.015. PMID 16887405.
- 1 2 "Tuberculosis". Archived from the original on July 21, 2006. Retrieved 24 November 2011.
- ↑ Leung CC (June 2007). "Lower risk of tuberculosis in obesity". Arch. Intern. Med. 167 (12): 1297–304. doi:10.1001/archinte.167.12.1297. PMID 17592104.
Figures OI70054T5, OI70054F1
{{cite journal}}: External link in|quote= - ↑ Restrepo, BI (2007). "Convergence of the tuberculosis and diabetes epidemics: renewal of old acquaintances". Clin Infect Dis. 45 (4): 436–8. doi:10.1086/519939. PMC 2900315. PMID 17638190.
- ↑ Nijland HMJ, et al. (2006). "Exposure to rifampicin is strongly reduced in patients with tuberculosis and type 2 diabetes". Clin Infect Dis. 43 (7): 848–854. doi:10.1086/507543. PMID 16941365.
- 1 2 Strachan DP, Powell KJ, Thaker A, Millard FJ, Maxwell JD (February 1995). "Vegetarian diet as a risk factor for tuberculosis in immigrant south London Asians". Thorax. 50 (2): 175–80. doi:10.1136/thx.50.2.175. PMC 473919. PMID 7701458.
- ↑ Davis L (1995). "Vegetarian diet and tuberculosis in immigrant Asians". Thorax. 50 (8): 915–6. doi:10.1136/thx.50.8.915-c. PMC 474924. PMID 7570453.
- ↑ Ustianowski A, Shaffer R, Collin S, Wilkinson RJ, Davidson RN (2005). "Prevalence and associations of vitamin D deficiency in foreign-born persons with tuberculosis in London". J Infect. 50 (5): 432–7. doi:10.1016/j.jinf.2004.07.006. PMID 15907552.
- ↑ Nnoaham KE, Clarke A (2008). "Low serum vitamin D levels and tuberculosis: a systematic review and meta-analysis". Int J Epidemiol. 37 (1): 113–9. doi:10.1093/ije/dym247. PMID 18245055. Archived from the original on 2022-07-14. Retrieved 2022-07-11.
- ↑ Schaible UE, Kaufmann SH (2007). "Malnutrition and Infection: Complex Mechanisms and Global Impacts". PLOS Medicine. 4 (5): e115. doi:10.1371/journal.pmed.0040115. PMC 1858706. PMID 17472433.
- ↑ Lönnroth K, Raviglione M (2008). "Global epidemiology of tuberculosis: prospects for control". Seminars in Respiratory and Critical Care Medicine. 29 (5): 481–91. doi:10.1055/s-0028-1085700. PMID 18810682.
- ↑ Davies PD (2003). "The world-wide increase in tuberculosis: how demographic changes, HIV infection and increasing numbers in poverty are increasing tuberculosis". Annals of Medicine. 35 (4): 235–43. doi:10.1080/07853890310005713. PMID 12846265. S2CID 25007313.
- ↑ Spence DP, Hotchkiss J, Williams CS, Davies PD (1993). "Tuberculosis and poverty". BMJ (Clinical Research Ed.). 307 (6907): 759–61. doi:10.1136/bmj.307.6907.759. PMC 1696420. PMID 8219945.
- ↑ "Increased US Prison Population Has Profound Demographic Consequences, Disproportionately Affecting Black Males". Medicalnewstoday.com. Archived from the original on 2022-07-14. Retrieved 2011-10-24.
- ↑ "Tuberculosis: stopping a killer that can't be kept behind bars". ICRC. Archived from the original on 25 July 2010. Retrieved 26 July 2011.
- ↑ Larouzé B, Sánchez A, Diuana V (2008). "Tuberculosis behind bars in developing countries: a hidden shame to public health". Trans. R. Soc. Trop. Med. Hyg. 102 (9): 841–2. doi:10.1016/j.trstmh.2008.04.020. PMID 18513772.
- 1 2 3 Harries, A. D., et al. "Defining the Research Agenda to Reduce the Joint Burden of Disease from Diabetes Mellitus and Tuberculosis " Tropical medicine & international health : TM & IH (2010) Web.
- ↑ Nnoaham KE, Clarke A (2008). "Low serum vitamin D levels and tuberculosis: a systematic review and meta-analysis". Int J Epidemiol. 37 (1): 113–19. doi:10.1093/ije/dym247. PMID 18245055.
- ↑ "Core Curriculum on Tuberculosis: What the Clinician Should Know" (4th ed.). Centers for Disease Control and Prevention (CDC), Division of Tuberculosis Elimination. 2000. Archived from the original on 2022-07-14. Retrieved 2022-07-14.