Ear pain
| Ear pain | |
|---|---|
| Other names: Otalgia, earache | |
 | |
| Examination of the ear canal and eardrum | |
| Specialty | Ear, nose and throat |
Ear pain, also known as earache or otalgia, is pain in the ear.[1] It may feel sharp or dull, and be present in one or both ears.[2]
Ear pain may be due to a problem in the ear or away from the ear.[1] Most causes of ear pain are not serious.[3][4] Primary ear pain is more common than secondary ear pain,[5] and it is often due to infection or injury.[3] The conditions that cause secondary (referred) ear pain are broad and range from temporomandibular joint syndrome to inflammation of the throat.[3]
In general, the reason for ear pain can be discovered by taking a thorough history of all symptoms and performing a physical examination, without need for imaging tools like a CT scan.[3] However, further testing may be needed if red flags are present like hearing loss, dizziness, ringing in the ear or unexpected weight loss.[6]
Management of ear pain depends on the cause. If there is a bacterial infection, antibiotics are sometimes recommended and over the counter pain medications can help control discomfort.[7] Some causes of ear pain require a procedure or surgery.[7][8][9]
83 percent of children have at least one episode of a middle ear infection by three years of age.[10]
Signs and symptoms
Ear pain can present in one or both ears. It may or may not be accompanied by other symptoms such as fever, sensation of the world spinning, ear itchiness, or a sense of fullness in the ear. The pain may or may not worsen with chewing.[3] The pain may also be continuous or intermittent.[11]
Ear pain due to an infection is the most common in children and can occur in babies.[10] Adults may need further evaluation if they have hearing loss, dizziness or ringing in the ear.[6] Additional red flags include diabetes, a weakened immune system, swelling seen on the outer ear, or swelling along the jaw.[12]
Causes
Ear pain has a variety of causes, the majority of which are not life-threatening.[3][4] Ear pain can originate from a part of the ear itself, known as primary ear pain, or from an anatomic structure outside the ear that is perceived as pain within the ear, known as secondary ear pain.[3] Secondary ear pain is a type of referred pain, meaning that the source of the pain differs from the location where the pain is felt. Primary ear pain is more common in children, whereas secondary (referred) pain is more common in adults.[13]
Primary ear pain is most commonly caused by infection or injury to one of the parts of the ear.[3]
External ear
Many conditions involving the external ear will be visible to the naked eye. Because the external ear is the most exposed portion of the ear, it is vulnerable to trauma or environmental exposures.[14] Blunt trauma, such as a blow to the ear, can result in a hematoma, or collection of blood between the cartilage and perichondrium of the ear. This type of injury is particularly common in contact sports such as wrestling and boxing.[15] Environmental injuries include sunburn, frostbite, or contact dermatitis.[14]
Less common causes of external ear pain include:[14][16]
- Auricular Cellulitis: a superficial infection of the ear that may be precipitated by trauma, an insect bite, or ear piercing
- Perichondritis: infection of the perichondrium, or fascia surrounding the ear cartilage, which can develop as a complication of untreated auricular cellulitis. It is important to identify and treat perichondritis with antibiotics to avoid permanent ear deformities.
- Relapsing polychondritis: a systemic inflammatory condition involving cartilage in many parts of the body, but often including the cartilage of both ears. The severity and prognosis of the disease varies widely.[17]
Otitis externa
Otitis externa, also known as "swimmer's ear", is a cellulitis of the external ear canal. In North America, 98% of cases are caused by bacteria, and the most common causative organisms are Pseudomonas and Staph aureus.[18] Risk factors include exposure to excessive moisture (e.g. from swimming or a warm climate) and disruption of the protective cerumen barrier, which can result from aggressive ear cleaning or placing objects in the ear.[19]
Malignant otitis externa is a rare and potentially life-threatening complication of otitis externa in which the infection spreads from the ear canal into the surrounding skull base, hence becoming an osteomyelitis.[16] It occurs largely in diabetic patients.[20] It is very rare in children, though can be seen in immunocompromised children and adults.[19] Pseudomonas is the most common causative organism.[20] The pain tends to be more severe than in uncomplicated otitis externa, and laboratory studies often reveal elevated inflammatory markers (ESR and/or CRP). The infection may extend to cranial nerves, or rarely to the meninges or brain.[20] Examination of the ear canal may reveal granulation tissue in the inferior canal. It is treated with several weeks of IV and oral antibiotics, usually fluoroquinolones.[20]
Mechanical obstruction
- Earwax impaction: results in 12 million medical visits annually in the United States.[21] Cerumen impaction may cause ear pain, but it can also prevent thorough examination of the ear and identification of an alternate source of pain.
- Foreign body: commonly include insects or small objects like beads[5]
Less common
- Herpes zoster: varicella zoster virus can reactivate in an area that includes the ear. Reactivation can produce pain and visible vesicles within the ear canal and, when combined with facial paralysis due to facial nerve involvement, is called Ramsay Hunt syndrome.[22]
- Tumors: the most common ear canal tumor is squamous cell carcinoma. Symptoms can resemble those of otitis externa, and cancer should be considered if the symptoms are not improving on appropriate treatment.[16]
Middle and inner ear
Acute otitis media

Acute otitis media is an infection of the middle ear. More than 80% of children experience at least one episode of otitis media by age 3 years.[23] Acute otitis media is also most common in these first 3 years of life, though older children may also experience it.[19] The most common causative bacteria are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis.[19] Otitis media often occurs with or following cold symptoms.[14] The diagnosis is made by the combination of symptoms and examination of the tympanic membrane for redness, bulging, and/or a middle ear effusion (collection of fluid within the middle ear).[5]
Complications of otitis media include hearing loss, facial nerve paralysis, or extension of infection to surrounding anatomic structures, including:[24]
- Mastoiditis: infection of the air cells in the mastoid process, the area of the skull located right behind the ear[19]
- Petrositis: infection of the petrous portion of the temporal bone
- Labyrinthitis
- Meningitis
- Subdural abscess
- Brain abscess
- Cerebral venous sinus thrombosis
Trauma
- Barotrauma: results from changes in atmospheric pressure that occur when descending in a plane or deep diving. As atmospheric pressure increases with descent, the eustachian tube collapses due to pressure within the middle ear being less than the external pressure, which causes pain. In severe cases, middle ear hemorrhage or tympanic membrane rupture can result.[16]
- Tympanic membrane rupture: disruption of the eardrum. This can be caused by a blow to the ear, blast injury, barotrauma, or direct penetration of the tympanic membrane by an object entering the ear.[5]
Referred ear pain
A variety of conditions can cause irritation of one of the nerves that provides sensation to the ear.
Conditions causing irritation the trigeminal nerve (cranial nerve V):[3]
- Temporomandibular joint syndrome: inflammation or abnormal movements of the joint between the jaw and skull. These disorders are most common in women of childbearing age, and are uncommon in children younger than 10 years old.[25][26][14]
- Myofascial pain syndrome: pain in the muscles involved in chewing. There may be certain parts of the muscles or tendons (connective tissue connecting the muscles to bones) that are especially painful when pressed[25]
- Trigeminal neuralgia: attacks of shooting pain down the face that may be triggered by touching the face or temperature changes[27]
- Dental pain from cavities or an abscess
- Oral cavity carcinoma
Conditions causing irritation of the facial nerve (cranial nerve VII) or glossopharyngeal nerve (cranial nerve IX):[3]
- Tonsillitis: infection/inflammation of the tonsils
- Post-tonsillectomy: pain following surgical removal of the tonsils
- Pharyngitis: infection/inflammation of the throat
- Sinusitis
- Parotitis: inflammation of the parotid gland, the salivary gland right in front of the ear
- Carcinoma of the oropharynx (base of tongue, soft palate, pharyngeal wall, tonsils)
Conditions causing irritation of the vagus nerve (cranial nerve X):[3]
- GERD
- Myocardial ischemia (inadequate oxygen supply to the heart muscle)
Conditions causing irritation of cervical nerves C2-C3:[3][14]
- Cervical spine trauma, arthritis (joint inflammation), or tumor
- Temporal arteritis: an autoimmune disorder leading to inflammation of the temporal artery, a large artery in the head. This condition tends to occur in adults older than 50.[16]
Pathophysiology
Primary ear pain
The ear can be anatomically divided into the external ear, the external auditory canal, the middle ear, and the inner ear.[28] These three are indistinguishable in terms of the pain experienced.[29]
Secondary ear pain

Many different nerves provide sensation to the various parts of the ear, including cranial nerves V (trigeminal), VII (facial), IX (glossopharyngeal), and X (vagus), and the great auricular nerve (cervical nerves C2-C3).[28][31] These nerves also supply other parts of the body, from the mouth to the chest and abdomen. Irritation of these nerves in another part of the body has the potential to produce pain in the ear.[28] This is called referred pain. Irritation of the trigeminal nerve (cranial nerve V) is the most common cause of referred ear pain.[3]
Diagnostic
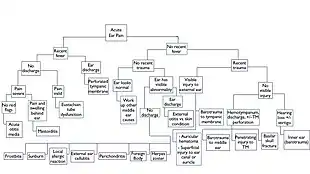

While some disorders may require specific imaging or testing, most etiologies of ear pain are diagnosed clinically. Because the differential for ear pain is so broad, there is no consensus on the best diagnostic framework to use. One approach is to differentiate by time course, as primary causes of ear pain are typically more acute in nature, while secondary causes of ear pain are more chronic.
Acute causes may be further distinguished by the presence of fever (indicating an underlying infection) or the absence of fever (suggesting a structural problem, such as such as trauma or other injury to the ear). Etiologies leading to chronic pain may be broken down by the presence or absence of worrisome clinical features, also known as red flags.
One red flag is the presence of one or multiple risk factors including smoking, heavy alcohol use (greater than 3.5 drinks per day), diabetes, coronary artery disease, and older age (greater than 50).[3] These factors increase the risk of having a serious cause of ear pain, like cancer or a serious infection. In particular, second hand smoke may increase risk of acute otitis media in children.[32] In addition, swimming is the most significant risk factor for otitis externae, though other risk factors include high humidity in the ear canal, eczema and/or ear trauma.[33]
If red flags are present it may be necessary to do additional workup such as a CT scan or biopsy to rule out a more dangerous diagnosis. Such diagnoses include malignant (or necrotizing) otitis externa, mastoiditis, temporal arteritis, and cancer. It is important to note that while the presence of a red flag does raise suspicion for one of these four disease, it does not guarantee a diagnosis as any one symptom can be seen in a variety of situations. For example, jaw claudication can be seen in temporal arteritis, but also in TMJ dysfunction.[4]
If there are no red flags, other sources of referred ear pain become more likely and are reasonable to pursue.
| Diagnosis | Features[4][8][9] | ||
|---|---|---|---|
| Acute otitis media | History of URI within 10 days | Child pulling on ear | Severe pain; feels deep inside the ear. |
| Fever | Hearing loss | Pain may disrupt sleep | |
| Perforated tympanic membrane | Discharge followed by pain improvement | ||
| Mastoiditis* | Children | History of URI >10 days | Recent history of URI or ear infection |
| Fevers/chills | May see signs of otitis media on exam | Pain is located behind the ear with postauricular (i.e. near mastoid process) swelling* | |
| Diagnose with CT | |||
| Chronic suppurative otitis media | Conductive hearing loss | Relapsing/remitting or chronic discharge | May see perforation of tympanic membrane or cholesteatoma on exam |
| Serous otitis media
(otitis media with effusion) |
No signs of infection | Prominent hearing loss | May have history of URI or acute otitis media |
| Otitis externa | Swimming | Psoriasis | Seborrheic dermatitis |
| Q-tips in the ear | Bilateral pain | Scaling | |
| Itching | Pain exacerbated when ear is pulled | May see granulation tissue in canal on exam | |
| Necrotizing/malignant
otitis externa* |
Diabetes | Immuno-compromised | Constant pain with increasing severity at night* |
| Purulent discharge* | Pain out of proportion to exam findings* | Biopsy granulation tissue for culture | |
| Chondritis vs perichondritis | Recent ear trauma (i.e. ear piercing) | External ear appears inflamed | Chondritis more likely than perichondritis if ear shape is distorted |
| Diagnosis | Features[4][8][9] | |
|---|---|---|
| GERD | Bilateral pain | |
| Neuralgia | Pain described as tingling/sharp/burning sensation; episodes can start with light touch | |
| Malignancy* | Weight loss* | |
| Arthritis of the neck | Pain exacerbated by neck movement | |
| Eagle syndrome | Swallowing exacerbates pain | |
| Infected 3rd molar | Extreme food temperatures exacerbate pain | |
| Temporal arteritis* | Patient age > 50* | Chewing exacerbates pain* |
| TMJ dysfunction | Patient grinds teeth | Bilateral pain |
| Pain + crepitus with TMJ palpation | Jaw clicking | |
*Indicates a "Can't Miss" diagnosis or a red flag.
| Diagnosis | Features[4][8][9] | ||
|---|---|---|---|
| Barotrauma | Recent ear trauma | Recent scuba diving or flying (+/- onset of pain coinciding with event) | Hearing loss |
| Eustachian tube dysfunction | Pain described as ear pressure or "plugged up" sensation in ears | Unilateral hearing loss | Crackling/gurgling sounds in ear |
| History of seasonal allergies | Poor light reflex and TM mobility | Air-fluid levels present | |
| Cerumen Impaction | Q-tips in the ear | Pain described as ear pressure or "plugged up" sensation in ears | May need to remove any ear wax present to rule this out as the underlying etiology |
Management
Management of ear pain depends on the underlying cause.
Antibiotics
While not all causes of ear pain are treated with antibiotics, those caused by bacterial infections of the ear are usually treated with antibiotics known to cover the common bacterial organisms for that type of infection. Many bacterial ear infections are treated with cleaning of the area, topical or systemic antibiotics, and oral analgesics for comfort.[7][34][9] Some types of bacterial ear infections can benefit from warm compresses included in the treatment.[7] Some of the causes of ear pain that are typically treated with either a topical or systemic antibiotic include:
- Uncomplicated acute bacterial otitis externa (AOE).[7][34] For symptoms that are not responsive to treatment within 10 days, a physician should evaluate for necrotizing external otitis.[7]
- Acute otitis media (AOM) self-resolves within 24–48 hours in 80% of cases.[34] If it does not self-resolve, AOM thought to be caused by bacteria is treated with systemic antibiotics. If symptoms do not respond to a week of treatment, a physician should evaluate for mastoiditis.[34]
- Acute folliculitis.[34]
- Auricular cellulitis.[9]
- Suppurative otitis media.[8] There is also a risk for tympanic membrane rupture.[8]
- Perichondritis. An otorhinolaryngologist should also evaluate it and if a foreign body is present in the cartilage, this foreign body should be removed.[34][8] If there is cartilage involvement, then more advance care with hospitalization is needed.[8]
- Sinusitis can cause secondary ear pain. Treating the underlying sinusitis will treat the ear pain. (See sinusitis.)[34]
Some bacterial infections may require a more advanced treatment with evaluation by otorhinolaryngology, IV antibiotics, and hospital admission.
- Necrotizing external otitis is potentially fatal and should be evaluated by an otorhinolaryngologist with admission to the hospital and IV antibiotics.[34][8](See otitis externa.)
- Acute mastoiditis is treated with admission to the hospital, otorhinolaryngology consultation and empiric IV antibiotics.[34][7][8][9] Cases with intracranial involvement are treated with a mastoidectomy with myringotomy.[34][9]
- Chondritis.[34][8]
Procedures
Some causes of ear pain require procedural management alone, by a health professional, or in addition to antibiotic therapy.
- Keratosis obturans is treated with removal of impacted desquamated keratin debris in the ear canal.[34]
- Chronic perichondritis and chondritis that continues to be symptomatic despite appropriate antibiotic management may require surgical debridement.[34] Surgical drainage could be required.[9]
- Bullous myringitis leads to the development of bullae on the tympanic membrane that can be punctured to give pain relief.[34]
- Foreign body in the ear canal can cause pain and be treated with careful removal.[8]
- Infected sebaceous cyst is treated with incision and drainage of the cysts, oral antibiotics and otorhinolaryngology assessment.[8]
Other
Given the variety of causes of ear pain, some causes require treatment other than antibiotics and procedures.
- Relapsing polychondritis is an autoimmune disease treated with immunomodulating medications (medications that help modulate the immune system).[34]
- Temporomandibular joint dysfunction can lead to secondary ear pain and can be initially treated with a soft food diet, NSAIDs, application of a heat pack, massage of local area, and a referral to a dentist.[34][16]
- Myofascial pain syndromes are initially treated with NSAIDs and physical therapy. Local anesthetic injection into the muscle trigger point can be considered in severe cases.[34]
- Glossopharyngeal neuralgia is treated with carbamazepine.[16]
Epidemiology
2/3 of people presenting with ear pain were diagnosed with some sort of primary otalgia and 1/3 were diagnosed with some sort secondary otalgia.[5]
A common cause of primary otalgia is ear infection called otitis media, meaning an infection behind the eardrum.[3] The peak age for children to get acute otitis media is ages 6–24 months. One review paper wrote that 83% of children had at least one episode of acute otitis media by 3 years of age.[10] Worldwide, there are 709 millions cases of acute otitis media every year.[35] Hearing loss globally due to ear infection is estimated to be 30 people in every 10,000.[35] Around the world there is around 21,000 to 28,000 deaths due to complications from ear infections.[35] These complications include brain abscesses and meningitis.
Otitis externae peaks at age 7–12 years of age and around 10% of people has had it at least once in their lives.[10]
Cerumen impaction occurs in 1 out of every 10 children, 1 in every 20 adults and 1 in every 3 elderly citizens.[10]
Barotrauma occurs around 1 in every 1000 people.[5]
Of people presenting with ear pain, only 3% was diagnosed with eustachian tube dysfunction.[3]
History

Not much was known about ear pain and acute otitis media before the 17th century. It was a common phenomenon with no treatment.[36] That changed when the otoscope was invented in the 1840s by Anton von Troeltsh in Germany.[36] Another shift came with the invention of antibiotics. Before antibiotics was introduced there use to be a high rate of ear infections spreading to the bone around the ear, but that is now considered a rare complication.[5]
Society and culture
There was previously a strong tradition of treating acute otitis media with amoxicillin.[5] One quote from the 1980s shows this sentiment by saying "any child with an earache has an acute amoxicillin deficiency".[5] However, people started realizing that using antibiotics too much can cause bacteria to gain resistance.[37] Increasing resistance makes antibiotics less effective. The term antibiotic stewardship is then used to describe the systematic effort to educate antibiotic prescribers to only give these medications when they are warranted. In particular to children, most ear pain resolves by itself with no complications.[35] There are guidelines Archived 2020-08-08 at the Wayback Machine in place to help determine when antibiotics for ear pain are needed in children.
The ear itself played a role in treatment via acupuncture, also known as auriculotherapy. It was believed that acupuncture of the ear could be used to correct other pain or disorders in the body. Such practices may have started as far back as the Stone Age. The first documentation of auriculotherapy in Europe was in the 1600s. One physician described stimulating the ear by burning or scarring to treat sciatic pain, while another physician applied this treatment for toothache. Paul Nogier is known as the father of ear acupuncture for his theory that parts of the ear corresponds to other areas of the body in a reliable fashion.[38]
Research
There are currently studies going on delivering antibiotics directly into the middle ear.[35]
References
- 1 2 Murr, Andrew H. (2020). "398. Approach to the patient with nose, sinus and ear disorders". In Goldman, Lee; Schafer, Andrew I. (eds.). Goldman-Cecil Medicine. Vol. 2 (26th ed.). Philadelphia: Elsevier. pp. 2554–2556. ISBN 978-0-323-53266-2. Archived from the original on 2022-05-27. Retrieved 2022-05-27.
- ↑ "Earache: MedlinePlus Medical Encyclopedia". medlineplus.gov. Archived from the original on 2017-10-03. Retrieved 2017-10-02.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Earwood JS, Rogers TS, Rathjen NA (January 2018). "Ear Pain: Diagnosing Common and Uncommon Causes". American Family Physician. 97 (1): 20–27. PMID 29365233. Archived from the original on 2022-01-08. Retrieved 2022-05-17.

- 1 2 3 4 5 6 7 8 Sullivan DJ (2012). "Chapter 17:Ear Pain". In Henderson MC, Tierney LM, Smetana GW (eds.). The Patient History: An Evidence-Based Approach to Differential Diagnosis (2 ed.). New York, NY: The McGraw-Hill Companies. Archived from the original on 2019-04-16. Retrieved 2022-05-17.
- 1 2 3 4 5 6 7 8 9 Conover K (May 2013). "Earache". Emergency Medicine Clinics of North America. 31 (2): 413–42. doi:10.1016/j.emc.2013.02.001. PMID 23601480.
- 1 2 "Position Statement: Red Flags-Warning of Ear Disease". American Academy of Otolaryngology–Head and Neck Surgery. 2014-03-20. Archived from the original on 2018-03-14. Retrieved 2018-03-13.
- 1 2 3 4 5 6 7 Coombs C (2016). "Chapter 118: Ear and Mastoid Disorders in Infants and Children". In Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM (eds.). Tintinalli's Emergency Medicine: A Comprehensive Study Guide (8 ed.). New York, NY: McGraw-Hill Education. ISBN 978-0071794763. Archived from the original on 2019-04-16. Retrieved 2022-05-17.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Stallard TC (2017). "Chapter 32: Emergency Disorders of the Ear, Nose, Sinuses, Oropharynx, & Mouth". In Stone CK, Humphries RL (eds.). CURRENT Diagnosis & Treatment: Emergency Medicine (8 ed.). New York, NY: McGraw-Hill Education. Archived from the original on 2019-04-16. Retrieved 2022-05-17.
- 1 2 3 4 5 6 7 8 9 10 11 Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J, eds. (2016). "Chapter 58: Sore Throat, Earache, and Upper Respiratory Symptoms". Harrison's Manual of Medicine (19th ed.). McGraw-Hill Education. ISBN 978-0071828529. Archived from the original on 2021-04-19. Retrieved 2022-05-17.
- 1 2 3 4 5 Rosa-Olivares J, Porro A, Rodriguez-Varela M, Riefkohl G, Niroomand-Rad I (November 2015). "Otitis Media: To Treat, To Refer, To Do Nothing: A Review for the Practitioner". Pediatrics in Review. 36 (11): 480–6, quiz 487–8. doi:10.1542/pir.36-11-480. PMID 26527627.
- ↑ Harrison E, Cronin M (July 2016). "Otalgia". Australian Family Physician. 45 (7): 493–7. PMID 27610432. Archived from the original on 2022-04-19. Retrieved 2022-05-17.
- ↑ Tucci, Debara L. (October 2016). "Earache". Ear, Nose, and Throat Disorders - Merck Manuals Professional Edition. Archived from the original on 2021-10-30. Retrieved 2022-05-17.
- ↑ Li, John (2017-09-21). "Otalgia: Background, Pathophysiology, Epidemiology". Medscape. Archived from the original on 2022-05-05. Retrieved 2022-05-17.
- 1 2 3 4 5 6 Greenes, David. "Evaluation of earache in children". www.uptodate.com. Archived from the original on 2018-03-14. Retrieved 2018-03-14.
- ↑ Leybell, Inna (2017-06-20). "Auricular Hematoma Drainage: Overview, Indications, Contraindications". Medscape. Archived from the original on 2021-01-17. Retrieved 2022-05-27.
- 1 2 3 4 5 6 7 Lustig LR, Schindler JS (2017). "Chapter 8: Ear, Nose, & Throat Disorders". In Papadakis MA, McPhee SJ, Rabow MW (eds.). Current Medical Diagnosis & Treatment 2018. New York, NY: McGraw-Hill Education. Archived from the original on 2022-05-27. Retrieved 2022-05-17.
- ↑ Compton, Nicholas. "Relapsing Polychondritis Clinical Presentation: History, Physical, Causes". emedicine.medscape.com. Archived from the original on 2018-03-14. Retrieved 2018-03-14.
- ↑ Rosenfeld RM, Schwartz SR, Cannon CR, Roland PS, Simon GR, Kumar KA, Huang WW, Haskell HW, Robertson PJ (February 2014). "Clinical practice guideline: acute otitis externa". Otolaryngology–Head and Neck Surgery. 150 (1 Suppl): S1–S24. doi:10.1177/0194599813517083. PMID 24491310. S2CID 40005605.
- 1 2 3 4 5 Yoon PJ, Scholes MA, Friedman NR (2016). "Chapter 18: Ear, Nose, & Throat". In Hay WW, Levin MJ, Deterding RR, Abzug MJ (eds.). CURRENT Diagnosis & Treatment Pediatrics (23rd ed.). New York, NY: McGraw-Hill Education. ISBN 978-0071848541. Archived from the original on 2022-05-27. Retrieved 2022-05-17.
- 1 2 3 4 Grandis, Jennifer; et al. (February 2018). "Malignant (necrotizing) otitis externa". www.uptodate.com. Archived from the original on 2018-03-14. Retrieved 2018-03-14.
- ↑ Schwartz S, et al. (January 2017). "Clinical Practice Guideline (Update): Earwax (Cerumen Impaction) Executive Summary". Otolaryngology–Head and Neck Surgery. 156 (1): 14–29. doi:10.1177/0194599816678832. PMID 28045632.
- ↑ Albrecht, Mary (August 2016). "Clinical manifestations of varicella-zoster virus infection: Herpes zoster". www.uptodate.com. Archived from the original on 2018-03-14. Retrieved 2018-03-14.
- ↑ Leung AK, Wong AH (2017). "Acute Otitis Media in Children". Recent Patents on Inflammation & Allergy Drug Discovery. 11 (1): 32–40. doi:10.2174/1874609810666170712145332. PMID 28707578.
- ↑ Klein, Jerome; et al. (September 2017). "Acute otitis media in children". www.uptodate.com. Archived from the original on 2018-03-14. Retrieved 2018-03-14.
- 1 2 Goddard, Greg (2012). "Chapter 26. Temporomandibular Disorders". In Lalwani, Anil K. (ed.). CURRENT Diagnosis & Treatment in Otolaryngology—Head & Neck Surgery (3 ed.). New York, NY: The McGraw-Hill Companies. Archived from the original on 2022-05-27. Retrieved 2022-05-17.
- ↑ Tsai, Vivian (2018-01-02). "Temporomandibular Joint Syndrome: Background, Pathophysiology, Epidemiology". Medscape. Archived from the original on 2022-02-19. Retrieved 2022-05-17.
- ↑ Singh, Manish (2017-09-26). "Trigeminal Neuralgia: Practice Essentials, Background, Anatomy". Medscape. Archived from the original on 2022-02-04. Retrieved 2022-05-17.
- 1 2 3 Morton DA, Foreman KB, Albertine KH (2011). "Chapter 19. Ear". The Big Picture: Gross Anatomy. New York, NY: The McGraw-Hill Companies. ISBN 978-0071476720.
- ↑ Gross M, Eliashar R (2008). "Chapter 6: Otolaryngological aspects of orofacial pain". In Sharav Y, Benoliel R (eds.). Orofacial Pain and Headache. Elsevier Health Sciences. p. 91. ISBN 9780723434122. Archived from the original on 2022-05-27. Retrieved 2022-05-17.
- ↑ Chen, R. C.; Khorsandi, A. S.; Shatzkes, D. R.; Holliday, R. A. (2009-11-01). "The Radiology of Referred Otalgia". American Journal of Neuroradiology. 30 (10): 1817–1823. doi:10.3174/ajnr.A1605. ISSN 0195-6108. PMC 7051282. PMID 19797791.
- ↑ Scarbrough TJ, Day TA, Williams TE, Hardin JH, Aguero EG, Thomas CR (October 2003). "Referred otalgia in head and neck cancer: a unifying schema". American Journal of Clinical Oncology. 26 (5): e157–62. doi:10.1097/01.coc.0000091357.08692.86. PMID 14528091. S2CID 35512999.
- ↑ "Ear Infections in Children". NIDCD. 2015-08-18. Archived from the original on 2018-03-14. Retrieved 2018-03-14.
- ↑ Schaefer P, Baugh RF (December 2012). "Acute otitis externa: an update". American Family Physician. 86 (11): 1055–61. PMID 23198673. Archived from the original on 2022-03-23. Retrieved 2022-05-17.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Neilan RE, Roland PS (September 2010). "Otalgia". The Medical Clinics of North America. 94 (5): 961–71. doi:10.1016/j.mcna.2010.05.004. PMID 20736106.
- 1 2 3 4 5 Qureishi A, Lee Y, Belfield K, Birchall JP, Daniel M (January 2014). "Update on otitis media - prevention and treatment". Infection and Drug Resistance. 7: 15–24. doi:10.2147/IDR.S39637. PMC 3894142. PMID 24453496.
- 1 2 Altemeier, William A (2000-10-01). "A Brief History of Otitis Media". Pediatric Annals. 29 (10): 599. doi:10.3928/0090-4481-20001001-03. ISSN 0090-4481. PMID 11056932.
- ↑ Fleming, Alexander (25 June 1945). "The Penicillin Finder Assays its Future". The New York Times: 21.
- ↑ Gori L, Firenzuoli F (September 2007). "Ear acupuncture in European traditional medicine". Evidence-Based Complementary and Alternative Medicine. 4 (Suppl 1): 13–6. doi:10.1093/ecam/nem106. PMC 2206232. PMID 18227925.
External links
| Classification | |
|---|---|
| External resources |