Androgen insensitivity syndrome
Androgen insensitivity syndrome (AIS) is a difference in sex development involving hormonal resistance due to androgen receptor dysfunction.[1]
| Androgen insensitivity syndrome | |
|---|---|
 | |
| AIS results when the function of the androgen receptor (AR) is impaired. The AR protein (pictured) mediates the effects of androgens in the human body. | |
| Specialty | Endocrinology |
It affects 1 in 20,000 to 64,000 XY (karyotypically male) births. The condition results in the partial or complete inability of cells to respond to androgens.[2] This unresponsiveness can impair or prevent the development of male genitals, as well as impairing or preventing the development of male secondary sexual characteristics at puberty. It does not significantly impair female genital or sexual development.[3][4] The insensitivity to androgens is therefore clinically significant only when it occurs in genetic males, (i.e. individuals with a Y-chromosome, or more specifically, an SRY gene).[5] Clinical phenotypes in these individuals range from a typical male habitus with mild spermatogenic defect or reduced secondary terminal hair, to a full female habitus, despite the presence of a Y-chromosome.[6]
AIS is divided into three categories that are differentiated by the degree of genital masculinization: complete androgen insensitivity syndrome (CAIS) is indicated when the external genitalia are those of a typical female; mild androgen insensitivity syndrome (MAIS) is indicated when the external genitalia are those of a typical male, and partial androgen insensitivity syndrome (PAIS) is indicated when the external genitalia are partially, but not fully, masculinized.[7][8] Androgen insensitivity syndrome is the largest single entity that leads to 46,XY undermasculinized genitalia.[9]
Management of AIS is currently limited to symptomatic management; no method is currently available to correct the malfunctioning androgen receptor proteins produced by AR gene mutations. Areas of management include sex assignment, genitoplasty, gonadectomy to reduce tumor risk, hormone replacement therapy, genetic counseling, and psychological counseling.
Genetics
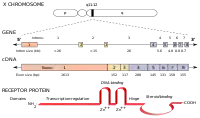
The human androgen receptor (AR) is a protein encoded by a gene located on the proximal long arm of the X chromosome (locus Xq11-Xq12).[10] The protein coding region consists of approximately 2,757 nucleotides (919 codons) spanning eight exons, designated 1-8 or A-H.[5][3] Introns vary in size between 0.7 and 26 kb.[3] Like other nuclear receptors, the AR protein consists of several functional domains: the transactivation domain (also called the transcription-regulation domain or the amino / NH2-terminal domain), the DNA-binding domain, the hinge region, and the steroid-binding domain (also called the carboxyl-terminal ligand-binding domain).[5][11][3][12] The transactivation domain is encoded by exon 1, and makes up more than half of the AR protein.[3] Exons 2 and 3 encode the DNA-binding domain, while the 5' portion of exon 4 encodes the hinge region.[3] The remainder of exons 4 through 8 encodes the ligand binding domain.[3]
Trinucleotide satellite lengths and AR transcriptional activity
The AR gene contains two polymorphic trinucleotide microsatellites in exon 1.[11] The first microsatellite (nearest the 5' end) contains 8 [13] to 60 [14][15] repetitions of the glutamine codon "CAG" and is thus known as the polyglutamine tract.[3] The second microsatellite contains 4 [16] to 31[17] repetitions of the glycine codon "GGC" and is known as the polyglycine tract.[18] The average number of repetitions varies by ethnicity, with Caucasians exhibiting an average of 21 CAG repeats, and Blacks 18.[19] In men, disease states are associated with extremes in polyglutamine tract length; prostate cancer,[20] hepatocellular carcinoma,[21] and intellectual disability[13] are associated with too few repetitions, while spinal and bulbar muscular atrophy (SBMA) is associated with a CAG repetition length of 40 or more.[22] Some studies indicate that the length of the polyglutamine tract is inversely correlated with transcriptional activity in the AR protein, and that longer polyglutamine tracts may be associated with male infertility[23][24][25] and undermasculinized genitalia in men.[26] However, other studies have indicated no such correlation exists.[27][28] A comprehensive meta-analysis of the subject published in 2007 supports the existence of the correlation, and concluded these discrepancies could be resolved when sample size and study design are taken into account.[29] Some studies suggest longer polyglycine tract lengths are also associated with genital masculinization defects in men.[30][31] Other studies find no such association.[32]
AR mutations
As of 2010, over 400 AR mutations have been reported in the AR mutation database, and the number continues to grow.[11] Inheritance is typically maternal and follows an X-linked recessive pattern;[5][33] individuals with a 46,XY karyotype always express the mutant gene since they have only one X chromosome, whereas 46,XX carriers are minimally affected. About 30% of the time, the AR mutation is a spontaneous result, and is not inherited.[34] Such de novo mutations are the result of a germ cell mutation or germ cell mosaicism in the gonads of one of the parents, or a mutation in the fertilized egg itself.[35] In one study,[36] three of eight de novo mutations occurred in the postzygotic stage, leading to the estimate that up to one-third of de novo mutations result in somatic mosaicism.[5] Not every mutation of the AR gene results in androgen insensitivity; one particular mutation occurs in 8 to 14% of genetic males,[37][38][39][40] and is thought to adversely affect only a small number of individuals when other genetic factors are present.[41]
Other causes
Some individuals with CAIS or PAIS do not have any AR mutations despite clinical, hormonal, and histological features sufficient to warrant an AIS diagnosis; up to 5% of women with CAIS do not have an AR mutation,[11] as well as between 27[42][43] and 72%[44] of individuals with PAIS.
In one patient, the underlying cause for presumptive PAIS was a mutant steroidogenic factor-1 (SF-1) protein.[45] In another patient, CAIS was the result of a deficit in the transmission of a transactivating signal from the N-terminal region of the androgen receptor to the basal transcription machinery of the cell.[46] A coactivator protein interacting with the activation function 1 (AF-1) transactivation domain of the androgen receptor may have been deficient in this patient.[46] The signal disruption could not be corrected by supplementation with any coactivators known at the time, nor was the absent coactivator protein characterized, which left some in the field unconvinced that a mutant coactivator would explain the mechanism of androgen resistance in CAIS or PAIS patients with a typical AR gene.[5]
XY karyotype
Depending on the mutation, a person with a 46,XY karyotype and AIS can have either a male (MAIS) or female (CAIS) phenotype,[47] or may have genitalia that are only partially masculinized (PAIS).[48] The gonads are testes regardless of phenotype due to the influence of the Y chromosome.[49][50] A 46,XY female, thus, does not have ovaries,[51] and can not contribute an egg towards conception. In some cases, 46, XY females do form a vestigial uterus and have been able to gestate children. Such examples are rare and have required the use of an egg donor, hormone therapy, and IVF.[52]
Several case studies of fertile 46,XY males with AIS have been published,[53][54] although this group is thought to be a minority.[12] In some cases, infertile males with MAIS have been able to conceive children after increasing their sperm count through the use of supplementary testosterone.[5][55]
A genetic male conceived by a man with AIS would not receive his father's X chromosome, thus would neither inherit nor carry the gene for the syndrome. A genetic female conceived in such a way would receive her father's X chromosome, thus would become a carrier.
XX karyotype
Genetic females (46,XX karyotype) have two X chromosomes, thus have two AR genes. A mutation in one (but not both) results in a minimally affected, fertile, female carrier. Some carriers have been noted to have slightly reduced body hair, delayed puberty, and/or tall stature, presumably due to skewed X-inactivation.[3][4] A female carrier will pass the affected AR gene to her children 50% of the time. If the affected child is a genetic female, she, too, will be a carrier. An affected 46,XY child will have AIS.
A genetic female with mutations in both AR genes could theoretically result from the union of a fertile man with AIS and a female carrier of the gene, or from de novo mutation. However, given the scarcity of fertile AIS men and low incidence of AR mutation, the chances of this occurrence are small. The phenotype of such an individual is a matter of speculation; as of 2010, no such documented case has been published.
Correlation of genotype and phenotype
Individuals with partial AIS, unlike those with the complete or mild forms, present at birth with ambiguous genitalia, and the decision to raise the child as male or female is often not obvious.[5][35][56] Unfortunately, little information regarding phenotype can be gleaned from precise knowledge of the AR mutation itself; the same AR mutation may cause significant variation in the degree of masculinization in different individuals, even among members of the same family.[57][58] Exactly what causes this variation is not entirely understood, although factors contributing to it could include the lengths of the polyglutamine and polyglycine tracts,[59] sensitivity to and variations in the intrauterine endocrine milieu,[48] the effect of coregulatory proteins active in Sertoli cells,[18][60] somatic mosaicism,[5] expression of the 5RD2 gene in genital skin fibroblasts,[57] reduced AR transcription and translation from factors other than mutations in the AR coding region,[61] an unidentified coactivator protein,[46] enzyme deficiencies such as 21-hydroxylase deficiency,[4] or other genetic variations such as a mutant steroidogenic factor-1 protein.[45] The degree of variation, however, does not appear to be constant across all AR mutations, and is much more extreme in some.[5][4][41][48] Missense mutations that result in a single amino acid substitution are known to produce the most phenotypic diversity.[11]
Pathophysiology

Androgens and the androgen receptor
The effects that androgens have on the human body (virilization, masculinization, anabolism, etc.) are not brought about by androgens themselves, but rather are the result of androgens bound to androgen receptors; the androgen receptor mediates the effects of androgens in the human body.[63] Likewise, the androgen receptor itself is generally inactive in the cell until androgen binding occurs.[3]
The following series of steps illustrates how androgens and the androgen receptor work together to produce androgenic effects:[5][11][3][12]
- Androgen enters the cell.
- Only certain organs in the body, such as the gonads and the adrenal glands, produce the androgen testosterone.
- Testosterone is converted into dihydrotestosterone, a chemically similar androgen, in cells containing the enzyme 5-alpha reductase.
- Both androgens exert their influence through binding with the androgen receptor.
- Androgen binds with the androgen receptor.
- The androgen receptor is expressed ubiquitously throughout the tissues of the human body.
- Before it binds with an androgen, the androgen receptor is bound to heat shock proteins.
- These heat shock proteins are released upon androgen binding.
- Androgen binding induces a stabilizing, conformational change in the androgen receptor.
- The two zinc fingers of the DNA-binding domain are exposed as a result of this new conformation.
- AR stability is thought to be aided by type II coregulators, which modulate protein folding and androgen binding, or facilitate NH2/carboxyl-terminal interaction.
- The hormone-activated androgen receptor is phosphorylated.
- Receptor phosphorylation can occur before androgen binding, although the presence of androgen promotes hyperphosphorylation.
- The biological ramifications of receptor phosphorylation are unknown.
- The hormone-activated androgen receptor translocates to the nucleus.
- Nucleocytoplasmic transport is in part facilitated by an amino acid sequence on the AR called the nuclear localization signal.
- The AR's nuclear localization signal is primarily encoded in the hinge region of the AR gene.
- Homodimerization occurs.
- Dimerization is mediated by the second (nearest the 3' end) zinc finger.
- DNA binding to regulatory androgen response elements occurs.
- Target genes contain (or are flanked by) transcriptional enhancer nucleotide sequences that interact with the first zinc finger.
- These areas are called androgen response elements.
- Coactivators are recruited by the AR.
- Type I coactivators (i.e., coregulators) are thought to influence AR transcriptional activity by facilitating DNA occupancy, chromatin remodeling, or the recruitment of general transcription factors associated with RNA polymerase II holocomplex.
- Target gene transcription ensues.
In this way, androgens bound to androgen receptors regulate the expression of target genes, thus produce androgenic effects.[64]
Theoretically, certain mutant androgen receptors can function without androgens; in vitro studies have demonstrated that a mutant androgen receptor protein can induce transcription in the absence of androgen if its steroid binding domain is deleted.[65][66] Conversely, the steroid-binding domain may act to repress the AR transactivation domain, perhaps due to the AR's unliganded conformation.[3]
Androgens in fetal development
Human embryos develop similarly for the first six weeks, regardless of genetic sex (46,XX or 46,XY karyotype); the only way to tell the difference between 46,XX or 46,XY embryos during this time period is to look for Barr bodies or a Y chromosome.[68] The gonads begin as bulges of tissue called the genital ridges at the back of the abdominal cavity, near the midline. By the fifth week, the genital ridges differentiate into an outer cortex and an inner medulla, and are called indifferent gonads.[68] By the sixth week, the indifferent gonads begin to differentiate according to genetic sex. If the karyotype is 46,XY, testes develop due to the influence of the Y chromosome’s SRY gene.[49][50] This process does not require the presence of androgen, nor a functional androgen receptor.[49][50]
Until around the seventh week of development, the embryo has indifferent sex accessory ducts, which consist of two pairs of ducts: the Müllerian ducts and the Wolffian ducts.[68] Sertoli cells within the testes secrete anti-Müllerian hormone around this time to suppress the development of the Müllerian ducts, and cause their degeneration.[68] Without this anti-Müllerian hormone, the Müllerian ducts develop into the female internal genitalia (uterus, cervix, fallopian tubes, and upper vaginal barrel).[68] Unlike the Müllerian ducts, the Wolffian ducts will not continue to develop by default.[69] In the presence of testosterone and functional androgen receptors, the Wolffian ducts develop into the epididymides, vasa deferentia, and seminal vesicles.[68] If the testes fail to secrete testosterone, or the androgen receptors do not function properly, the Wolffian ducts degenerate.[70]
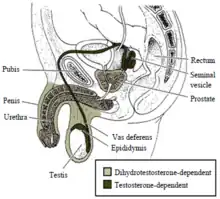
Masculinization of the male external genitalia (the penis, penile urethra, and scrotum), as well as the prostate, are dependent on the androgen dihydrotestosterone.[71][72][73][74] Testosterone is converted into dihydrotestosterone by the 5-alpha reductase enzyme.[75] If this enzyme is absent or deficient, then dihydrotestosterone is not created, and the external male genitalia do not develop properly.[71][72][73][74][75] As is the case with the internal male genitalia, a functional androgen receptor is needed for dihydrotestosterone to regulate the transcription of target genes involved in development.[63]
Pathogenesis of AIS
Mutations in the androgen receptor gene can cause problems with any of the steps involved in androgenization, from the synthesis of the androgen receptor protein itself, through the transcriptional ability of the dimerized, androgen-AR complex.[3] AIS can result if even one of these steps is significantly disrupted, as each step is required for androgens to activate the AR successfully and regulate gene expression.[3] Exactly which steps a particular mutation will impair can be predicted, to some extent, by identifying the area of the AR in which the mutation resides. This predictive ability is primarily retrospective in origin; the different functional domains of the AR gene have been elucidated by analyzing the effects of specific mutations in different regions of the AR.[3] For example, mutations in the steroid binding domain have been known to affect androgen binding affinity or retention, mutations in the hinge region have been known to affect nuclear translocation, mutations in the DNA-binding domain have been known to affect dimerization and binding to target DNA, and mutations in the transactivation domain have been known to affect target gene transcription regulation.[3][69] Unfortunately, even when the affected functional domain is known, predicting the phenotypical consequences of a particular mutation (see Correlation of genotype and phenotype) is difficult.
Some mutations can adversely impact more than one functional domain. For example, a mutation in one functional domain can have deleterious effects on another by altering the way in which the domains interact.[69] A single mutation can affect all downstream functional domains if a premature stop codon or framing error results; such a mutation can result in a completely unusable (or unsynthesizable) androgen receptor protein.[3] The steroid binding domain is particularly vulnerable to the effects of a premature stop codon or framing error, since it occurs at the end of the gene, and its information is thus more likely to be truncated or misinterpreted than other functional domains.[3]
Other, more complex relationships have been observed as a consequence of mutated AR; some mutations associated with male phenotypes have been linked to male breast cancer, prostate cancer, or in the case of spinal and bulbar muscular atrophy, disease of the central nervous system.[76][20][77][78][79] The form of breast cancer seen in some men with PAIS is caused by a mutation in the AR's DNA-binding domain.[77][79] This mutation is thought to cause a disturbance of the AR's target gene interaction that allows it to act at certain additional targets, possibly in conjunction with the estrogen receptor protein, to cause cancerous growth.[3] The pathogenesis of spinal and bulbar muscular atrophy (SBMA) demonstrates that even the mutant AR protein itself can result in pathology. The trinucleotide repeat expansion of the polyglutamine tract of the AR gene that is associated with SBMA results in the synthesis of a misfolded AR protein that the cell fails to proteolyze and disperse properly.[80] These misfolded AR proteins form aggregates in the cell cytoplasm and nucleus.[80] Over the course of 30 to 50 years, these aggregates accumulate and have a cytotoxic effect, eventually resulting in the neurodegenerative symptoms associated with SBMA.[80]
Diagnosis
The phenotypes that result from the insensitivity to androgens are not unique to AIS, thus the diagnosis of AIS requires thorough exclusion of other causes.[9][81] Clinical findings indicative of AIS include the presence of a short vagina [82] or undermasculinized genitalia,[5][58][71] partial or complete regression of Müllerian structures,[83] bilateral nondysplastic testes,[84] and impaired spermatogenesis and/or virilization.[5][85][42][76] Laboratory findings include a 46,XY karyotype[11] and typical or elevated postpubertal testosterone, luteinizing hormone, and estradiol levels.[11][9] The androgen binding activity of genital skin fibroblasts is typically diminished,[3][86] although exceptions have been reported.[87] Conversion of testosterone to dihydrotestosterone may be impaired.[3] The diagnosis of AIS is confirmed if androgen receptor gene sequencing reveals a mutation, although not all individuals with AIS (particularly PAIS) will have an AR mutation (see Other Causes).[11][42][43][44]
Each of the three types of AIS (complete, partial, and mild) has a different list of differential diagnoses to consider.[5] Depending on the form of AIS suspected, the list of differentials can include:[49][50][88][89][90]
- Chromosomal anomalies:
- Klinefelter syndrome (47,XXY karyotype)
- Turner syndrome (45,XO karyotype)
- Mixed gonadal dysgenesis (45,XO/46,XY karyotype)
- Tetragametic chimerism (46,XX/46,XY karyotype)
- Androgen biosynthetic dysfunction in 46,XY individuals:
- Luteinizing hormone (LH) receptor mutations
- Smith–Lemli–Opitz syndrome (associated with intellectual disability)
- Lipoid congenital adrenal hyperplasia
- 3β-hydroxysteroid dehydrogenase 2 deficiency
- 17α-hydroxylase deficiency
- 17,20 lyase deficiency
- 17β-hydroxysteroid dehydrogenase deficiency
- 5α-reductase deficiency
- Androgen excess in 46,XX individuals:
- 21-hydroxylase deficiency
- 3β-hydroxysteroid dehydrogenase 2 deficiency
- Cytochrome P450 oxidoreductase deficiency (disorder in mother causes 46,XX fetal virilization)
- 11β-hydroxylase deficiency
- Aromatase deficiency
- Glucocorticoid receptor mutations
- Maternal virilizing tumor (e.g. luteoma)
- Increased androgen exposure in utero, not otherwise specified (e.g. androgenic drugs)
- Developmental
- Mayer–Rokitansky–Küster–Hauser syndrome (46,XX karyotype)
- Swyer syndrome (46,XY karyotype)
- XX gonadal dysgenesis (46,XX karyotype)
- Leydig cell agenesis or hypoplasia, not otherwise specified (46,XY karyotype)
- Absent (vanishing) testes syndrome
- Ovotesticular DSD
- Testicular DSD (i.e. 46,XX sex reversal)
- Teratogenic causes (e.g. estrogens, antiestrogens)
- Other causes:
- Frasier syndrome (associated with progressive glomerulopathy)
- Denys–Drash syndrome (associated with nephropathy and Wilms tumor)
- WAGR syndrome (associated with Wilms tumor and aniridia)
- McKusick–Kaufman syndrome (associated with postaxial polydactyly)
- Robinow syndrome (associated with dwarfism)
- Aarskog–Scott syndrome (associated with facial anomalies)
- Hand-foot-genital syndrome (associated with limb malformations)
- Popliteal pterygium syndrome (associated with extensive webbing behind knees)
- Kallmann syndrome (often associated with anosmia)
- Hypospadias not otherwise specified
- Cryptorchidism not otherwise specified
- vaginal atresia not otherwise specified
Classification

AIS is broken down into three classes based on phenotype: complete androgen insensitivity syndrome (CAIS), partial androgen insensitivity syndrome (PAIS), and mild androgen insensitivity syndrome (MAIS).[5][11][85][42][91][34][29][92][12] A supplemental system of phenotypic grading that uses seven classes instead of the traditional three was proposed by pediatric endocrinologist Charmian A. Quigley et al. in 1995.[3] The first six grades of the scale, grades 1 through 6, are differentiated by the degree of genital masculinization; grade 1 is indicated when the external genitalia is fully masculinized, grade 6 is indicated when the external genitalia is fully feminized, and grades 2 through 5 quantify four degrees of decreasingly masculinized genitalia that lie in the interim.[3] Grade 7 is indistinguishable from grade 6 until puberty, and is thereafter differentiated by the presence of secondary terminal hair; grade 6 is indicated when secondary terminal hair is present, whereas grade 7 is indicated when it is absent.[3] The Quigley scale can be used in conjunction with the traditional three classes of AIS to provide additional information regarding the degree of genital masculinization, and is particularly useful when the diagnosis is PAIS.[11][93]
Complete AIS
Partial AIS
Mild AIS
Management
Management of AIS is currently limited to symptomatic management; no method is currently available to correct the malfunctioning androgen receptor proteins produced by AR gene mutations. Areas of management include sex assignment, genitoplasty, gonadectomy in relation to tumor risk, hormone replacement therapy, genetic counseling, and psychological counseling.
CAIS
PAIS
MAIS
Epidemiology
AIS represents about 15% to 20% of DSDs and affects 1 in 20,000 to 1 in 64,000 males.[94]
Estimates for the incidence of androgen insensitivity syndrome are based on a relatively small population size, thus are known to be imprecise.[5] CAIS is estimated to occur in one of every 20,400 46,XY births.[95] A nationwide survey in the Netherlands based on patients with genetic confirmation of the diagnosis estimates that the minimal incidence of CAIS is one in 99,000.[57] The incidence of PAIS is estimated to be one in 130,000.[96] Due to its subtle presentation, MAIS is not typically investigated except in the case of male infertility,[71] thus its true prevalence is unknown.[11]
Controversy
Preimplantation genetic diagnosis
Preimplantation genetic diagnosis (PGD or PIGD) refers to genetic profiling of embryos prior to implantation (as a form of embryo profiling), and sometimes even of oocytes prior to fertilization. When used to screen for a specific genetic sequence, its main advantage is that it avoids selective pregnancy termination, as the method makes it highly likely that a selected embryo will be free of the condition under consideration.[97]
In the UK, AIS appears on a list of serious genetic diseases that may be screened for via PGD.[98] Some ethicists, clinicians, and intersex advocates have argued that screening embryos to specifically exclude intersex traits is based on social and cultural norms as opposed to medical necessity.[99][100][101]
History
Recorded descriptions of the effects of AIS date back hundreds of years, although significant understanding of its underlying histopathology did not occur until the 1950s.[5] The taxonomy and nomenclature associated with androgen insensitivity went through a significant evolution that paralleled this understanding.
Timeline of major milestones
- 1950: Lawson Wilkins administers daily methyltestosterone to a karyotype 46,XY female patient, who shows no signs of virilization. His experiment is the first documented demonstration of the pathophysiology of AIS.[81][102]
- 1970: Mary F. Lyon and Susan Hawkes reported that a gene on the X chromosome caused complete insensitivity to androgens in mice.[103][104]
- 1981: Barbara Migeon et al. narrowed down the locus of the human androgen receptor gene (or a factor controlling the androgen receptor gene) to somewhere between Xq11 and Xq13.[105][106]
- 1988: The human androgen receptor gene is first cloned and partially analyzed by multiple parties.[107][108] Terry Brown et al. reported the first mutations proven to cause AIS.[11][106]
- 1989: Terry Brown et al. reported the exact locus of the AR gene (Xq11-Xq12),[10] and Dennis Lubahn et al. published its intron-exon boundaries.[109]
- 1994: The androgen receptor gene mutations database was created to provide a comprehensive listing of mutations published in medical journals and conference proceedings.[110]
Early terminology
The first descriptions of the effects of AIS appeared in the medical literature as individual case reports or as part of a comprehensive description of intersex physicalities. In 1839, Scottish obstetrician Sir James Young Simpson published one such description[111] in an exhaustive study of intersexuality that has been credited with advancing the medical community's understanding of the subject.[112] Simpson's system of taxonomy, however, was far from the first; taxonomies or descriptions for the classification of intersexuality were developed by Italian physician and physicist Fortuné Affaitati in 1549,[113][114] French surgeon Ambroise Paré in 1573,[112][115] French physician and sexology pioneer Nicolas Venette in 1687 (under the pseudonym Vénitien Salocini),[116][117] and French zoologist Isidore Geoffroy Saint-Hilaire in 1832.[118] All five of these authors used the colloquial term "hermaphrodite" as the foundation of their taxonomies, although Simpson himself questioned the propriety of the word in his publication.[111] Use of the word "hermaphrodite" in the medical literature has persisted to this day,[119][120] although its propriety is still in question. An alternative system of nomenclature has been recently suggested,[121] but the subject of exactly which word or words should be used in its place still one of much debate.[89][122][123][124][125]

Pseudohermaphroditism
"Pseudohermaphroditism" has, until very recently,[121] been the term used in the medical literature to describe the condition of an individual whose gonads and karyotype do not match the external genitalia in the gender binary sense. For example, 46,XY individuals who have a female phenotype, but also have testes instead of ovaries—a group that includes all individuals with CAIS, as well as some individuals with PAIS—are classified as having "male pseudohermaphroditism", while individuals with both an ovary and a testis (or at least one ovotestis) are classified as having "true hermaphroditism".[120][121] Use of the word in the medical literature antedates the discovery of the chromosome, thus its definition has not always taken karyotype into account when determining an individual's sex. Previous definitions of "pseudohermaphroditism" relied on perceived inconsistencies between the internal and external organs; the "true" sex of an individual was determined by the internal organs, and the external organs determined the "perceived" sex of an individual.[111][118]
German-Swiss pathologist Edwin Klebs is sometimes noted for using the word "pseudohermaphroditism" in his taxonomy of intersexuality in 1876,[127] although the word is clearly not his invention as is sometimes reported; the history of the word "pseudohermaphrodite" and the corresponding desire to separate "true" hermaphrodites from "false", "spurious", or "pseudo" hermaphrodites, dates back to at least 1709, when Dutch anatomist Frederik Ruysch used it in a publication describing a subject with testes and a mostly female phenotype.[126] "Pseudohermaphrodite" also appeared in the Acta Eruditorum later that same year, in a review of Ruysch's work.[128] Also some evidence indicates the word was already being used by the German and French medical community long before Klebs used it; German physiologist Johannes Peter Müller equated "pseudohermaphroditism" with a subclass of hermaphroditism from Saint-Hilaire's taxonomy in a publication dated 1834,[129] and by the 1840s "pseudohermaphroditism" was appearing in several French and German publications, including dictionaries.[130][131][132][133]
Testicular feminization
In 1953, American gynecologist John Morris provided the first full description of what he called "testicular feminization syndrome" based on 82 cases compiled from the medical literature, including two of his own patients.[5][3][134] The term "testicular feminization" was coined to reflect Morris' observation that the testicles in these patients produced a hormone that had a feminizing effect on the body, a phenomenon now understood to be due to the inaction of androgens, and subsequent aromatization of testosterone into estrogen.[5] A few years before Morris published his landmark paper, Lawson Wilkins had shown through experiment that unresponsiveness of the target cell to the action of androgenic hormones was a cause of "male pseudohermaphroditism".[81][102] Wilkins' work, which clearly demonstrated the lack of a therapeutic effect when 46,XY patients were treated with androgens, caused a gradual shift in nomenclature from "testicular feminization" to "androgen resistance".[71]
Other names
A distinct name has been given to many of the various presentations of AIS, such as Reifenstein syndrome (1947),[135] Goldberg-Maxwell syndrome (1948),[136] Morris' syndrome (1953),[134] Gilbert-Dreyfus syndrome (1957),[137] Lub's syndrome (1959),[138] "incomplete testicular feminization" (1963),[139] Rosewater syndrome (1965),[140] and Aiman's syndrome (1979).[141] Since it was not understood that these different presentations were all caused by the same set of mutations in the androgen receptor gene, a unique name was given to each new combination of symptoms, resulting in a complicated stratification of seemingly disparate disorders.[81][142]
Over the last 60 years, as reports of strikingly different phenotypes were reported to occur even among members of the same family, and as steady progress was made towards the understanding of the underlying molecular pathogenesis of AIS, these disorders were found to be different phenotypic expressions of one syndrome caused by molecular defects in the androgen receptor gene.[5][12][81][142]
AIS is now the accepted terminology for the syndromes resulting from unresponsiveness of the target cell to the action of androgenic hormones.[5] CAIS encompasses the phenotypes previously described by "testicular feminization", Morris' syndrome, and Goldberg-Maxwell syndrome;[5][143] PAIS includes Reifenstein syndrome, Gilbert-Dreyfus syndrome, Lub's syndrome, "incomplete testicular feminization", and Rosewater syndrome;[142][144][145] and MAIS includes Aiman's syndrome.[146]
The more virilized phenotypes of AIS have sometimes been described as "undervirilized male syndrome", "infertile male syndrome", "undervirilized fertile male syndrome", etc., before evidence was reported that these conditions were caused by mutations in the AR gene.[147] These diagnoses were used to describe a variety of mild defects in virilization; as a result, the phenotypes of some men who have been diagnosed as such are better described by PAIS (e.g. micropenis, hypospadias, and undescended testes), while others are better described by MAIS (e.g. isolated male infertility or gynecomastia).[5][147][54][145][148][149]
Society and culture
In the film Orchids, My Intersex Adventure, Phoebe Hart and her sister Bonnie Hart, both women with CAIS, documented their exploration of AIS and other intersex issues.[150]
Recording artist Dalea is a Hispanic-American Activist who is public about her CAIS. She has given interviews about her condition[151][152] and founded Girl Comet, a non-profit diversity awareness and inspiration initiative.[153]
In 2017, fashion model Hanne Gaby Odiele disclosed that they were born with the intersex trait androgen insensitivity syndrome. As a child, they underwent medical procedures relating to the condition,[154] which they said took place without their or their parents' informed consent.[155] They were told about their intersex condition weeks before beginning their modelling career.[155]
In the 1991 Japanese horror novel Ring and its sequels, by Koji Suzuki (later adapted into Japanese, Korean, and American films), the central antagonist Sadako has this syndrome, as revealed by Dr Nagao when confronted by Ryuji and Asakawa.[156] Sadako's condition is referred to by the earlier name "testicular feminisation syndrome".
In season 2, episode 13 ("Skin Deep") of the TV series House, the main patient's cancerous testicle is mistaken for an ovary due to the patient's undiscovered CAIS.[157]
In season 2 of the MTV series Faking It, a character has CAIS. The character, Lauren Cooper, played by Bailey De Young, was the first intersex series regular on American television.[158][159]
In season 8, episode 11 ("Delko for the Defense") of the TV series CSI: Miami, the primary suspect has AIS which gets him off a rape charge.
In series 8, episode 5 of Call the Midwife, a woman discovers that she has AIS. She attends a cervical smear and brings up that she has never had a period, and is concerned about having children as she is about to be married. She is then diagnosed with "testicular feminisation syndrome", the old term for AIS.[160]
People with AIS
People with Partial androgen insensitivity syndrome
- Tony Briffa[173][174]
- Favorinus of Arelate has been described as having partial androgen insensitivity syndrome.[175][176]
- Small Luk[177]
- Eliana Rubashkyn[178][179][180]
- Sean Saifa Wall[181]
- Sogto Ochirov[182]
See also
References
- Legato, Marianne J. (2017-05-15). Principles of Gender-Specific Medicine: Gender in the Genomic Era. Academic Press. p. 34. ISBN 978-0-12-803542-9.
- Hughes IA, Deeb A (December 2006). "Androgen resistance". Best Pract. Res. Clin. Endocrinol. Metab. 20 (4): 577–98. doi:10.1016/j.beem.2006.11.003. PMID 17161333. Galani A, Kitsiou-Tzeli S, Sofokleous C, Kanavakis E, Kalpini-Mavrou A (2008). "Androgen insensitivity syndrome: clinical features and molecular defects". Hormones (Athens). 7 (3): 217–29. doi:10.14310/horm.2002.1201. PMID 18694860. Quigley CA, De Bellis A, Marschke KB, el-Awady MK, Wilson EM, French FS (June 1995). "Androgen receptor defects: historical, clinical, and molecular perspectives". Endocr. Rev. 16 (3): 271–321. doi:10.1210/edrv-16-3-271. PMID 7671849.
- Quigley CA, De Bellis A, Marschke KB, el-Awady MK, Wilson EM, French FS (June 1995). "Androgen receptor defects: historical, clinical, and molecular perspectives". Endocr. Rev. 16 (3): 271–321. doi:10.1210/edrv-16-3-271. PMID 7671849.
- Giwercman YL, Nordenskjöld A, Ritzén EM, Nilsson KO, Ivarsson SA, Grandell U, Wedell A (June 2002). "An androgen receptor gene mutation (E653K) in a family with congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency as well as in partial androgen insensitivity". J. Clin. Endocrinol. Metab. 87 (6): 2623–8. doi:10.1210/jcem.87.6.8518. PMID 12050225.
- Hughes IA, Deeb A (December 2006). "Androgen resistance". Best Pract. Res. Clin. Endocrinol. Metab. 20 (4): 577–98. doi:10.1016/j.beem.2006.11.003. PMID 17161333.
-
- Hughes IA, Deeb A (December 2006). "Androgen resistance". Best Pract. Res. Clin. Endocrinol. Metab. 20 (4): 577–98. doi:10.1016/j.beem.2006.11.003. PMID 17161333.
- Zuccarello D, Ferlin A, Vinanzi C, Prana E, Garolla A, Callewaert L, Claessens F, Brinkmann AO, Foresta C (April 2008). "Detailed functional studies on androgen receptor mild mutations demonstrate their association with male infertility". Clin. Endocrinol. 68 (4): 580–8. doi:10.1111/j.1365-2265.2007.03069.x. PMID 17970778. S2CID 2783902.
- Ferlin A, Vinanzi C, Garolla A, Selice R, Zuccarello D, Cazzadore C, Foresta C (November 2006). "Male infertility and androgen receptor gene mutations: clinical features and identification of seven novel mutations". Clin. Endocrinol. 65 (5): 606–10. doi:10.1111/j.1365-2265.2006.02635.x. PMID 17054461. S2CID 33713391.
- Stouffs K, Tournaye H, Liebaers I, Lissens W (2009). "Male infertility and the involvement of the X chromosome". Hum. Reprod. Update. 15 (6): 623–37. doi:10.1093/humupd/dmp023. PMID 19515807.
- Giwercman YL, Nikoshkov A, Byström B, Pousette A, Arver S, Wedell A (June 2001). "A novel mutation (N233K) in the transactivating domain and the N756S mutation in the ligand binding domain of the androgen receptor gene are associated with male infertility". Clin. Endocrinol. 54 (6): 827–34. doi:10.1046/j.1365-2265.2001.01308.x. PMID 11422119. S2CID 23554058.
- Lund A, Juvonen V, Lähdetie J, Aittomäki K, Tapanainen JS, Savontaus ML (June 2003). "A novel sequence variation in the transactivation regulating domain of the androgen receptor in two infertile Finnish men". Fertil. Steril. 79. Suppl 3: 1647–8. doi:10.1016/s0015-0282(03)00256-5. PMID 12801573.
-
- Hughes IA, Deeb A (December 2006). "Androgen resistance". Best Pract. Res. Clin. Endocrinol. Metab. 20 (4): 577–98. doi:10.1016/j.beem.2006.11.003. PMID 17161333.
- Galani A, Kitsiou-Tzeli S, Sofokleous C, Kanavakis E, Kalpini-Mavrou A (2008). "Androgen insensitivity syndrome: clinical features and molecular defects". Hormones (Athens). 7 (3): 217–29. doi:10.14310/horm.2002.1201. PMID 18694860.
- Zuccarello D, Ferlin A, Vinanzi C, Prana E, Garolla A, Callewaert L, Claessens F, Brinkmann AO, Foresta C (April 2008). "Detailed functional studies on androgen receptor mild mutations demonstrate their association with male infertility". Clin. Endocrinol. 68 (4): 580–8. doi:10.1111/j.1365-2265.2007.03069.x. PMID 17970778. S2CID 2783902.
- Ferlin A, Vinanzi C, Garolla A, Selice R, Zuccarello D, Cazzadore C, Foresta C (November 2006). "Male infertility and androgen receptor gene mutations: clinical features and identification of seven novel mutations". Clin. Endocrinol. 65 (5): 606–10. doi:10.1111/j.1365-2265.2006.02635.x. PMID 17054461. S2CID 33713391.
-
- Stouffs K, Tournaye H, Liebaers I, Lissens W (2009). "Male infertility and the involvement of the X chromosome". Hum. Reprod. Update. 15 (6): 623–37. doi:10.1093/humupd/dmp023. PMID 19515807.
- Ozülker T, Ozpaçaci T, Ozülker F, Ozekici U, Bilgiç R, Mert M (January 2010). "Incidental detection of Sertoli-Leydig cell tumor by FDG PET/CT imaging in a patient with androgen insensitivity syndrome". Ann Nucl Med. 24 (1): 35–9. doi:10.1007/s12149-009-0321-x. PMID 19957213. S2CID 10450803.
- Davis-Dao CA, Tuazon ED, Sokol RZ, Cortessis VK (November 2007). "Male infertility and variation in CAG repeat length in the androgen receptor gene: a meta-analysis". J. Clin. Endocrinol. Metab. 92 (11): 4319–26. doi:10.1210/jc.2007-1110. PMID 17684052.
- Kawate H, Wu Y, Ohnaka K, Tao RH, Nakamura K, Okabe T, Yanase T, Nawata H, Takayanagi R (November 2005). "Impaired nuclear translocation, nuclear matrix targeting, and intranuclear mobility of mutant androgen receptors carrying amino acid substitutions in the deoxyribonucleic acid-binding domain derived from androgen insensitivity syndrome patients". J. Clin. Endocrinol. Metab. 90 (11): 6162–9. doi:10.1210/jc.2005-0179. PMID 16118342.
- Gottlieb B, Lombroso R, Beitel LK, Trifiro MA (January 2005). "Molecular pathology of the androgen receptor in male (in)fertility". Reprod. Biomed. Online. 10 (1): 42–8. doi:10.1016/S1472-6483(10)60802-4. PMID 15705293.
- Ahmed SF, Cheng A, Hughes IA (April 1999). "Assessment of the gonadotrophin-gonadal axis in androgen insensitivity syndrome". Arch. Dis. Child. 80 (4): 324–9. doi:10.1136/adc.80.4.324. PMC 1717906. PMID 10086936.
- Brown CJ, Goss SJ, Lubahn DB, Joseph DR, Wilson EM, French FS, Willard HF (February 1989). "Androgen receptor locus on the human X chromosome: regional localization to Xq11-12 and description of a DNA polymorphism". American Journal of Human Genetics. 44 (2): 264–9. PMC 1715398. PMID 2563196.
- Galani A, Kitsiou-Tzeli S, Sofokleous C, Kanavakis E, Kalpini-Mavrou A (2008). "Androgen insensitivity syndrome: clinical features and molecular defects". Hormones (Athens). 7 (3): 217–29. doi:10.14310/horm.2002.1201. PMID 18694860.
- Gottlieb B, Lombroso R, Beitel LK, Trifiro MA (January 2005). "Molecular pathology of the androgen receptor in male (in)fertility". Reprod. Biomed. Online. 10 (1): 42–8. doi:10.1016/S1472-6483(10)60802-4. PMID 15705293.
- Kooy RF, Reyniers E, Storm K, Vits L, van Velzen D, de Ruiter PE, Brinkmann AO, de Paepe A, Willems PJ (July 1999). "CAG repeat contraction in the androgen receptor gene in three brothers with mental retardation". American Journal of Medical Genetics. 85 (3): 209–13. doi:10.1002/(SICI)1096-8628(19990730)85:3<209::AID-AJMG4>3.0.CO;2-2. PMID 10398229.
- Dejager S, Bry-Gauillard H, Bruckert E, Eymard B, Salachas F, LeGuern E, Tardieu S, Chadarevian R, Giral P, Turpin G (August 2002). "A comprehensive endocrine description of Kennedy's disease revealing androgen insensitivity linked to CAG repeat length". J. Clin. Endocrinol. Metab. 87 (8): 3893–901. doi:10.1210/jcem.87.8.8780. PMID 12161529.
- Choong CS, Wilson EM (December 1998). "Trinucleotide repeats in the human androgen receptor: a molecular basis for disease". J. Mol. Endocrinol. 21 (3): 235–57. doi:10.1677/jme.0.0210235. PMID 9845666.
- Audi L, Fernández-Cancio M, Carrascosa A, et al. (April 2010). "Novel (60%) and recurrent (40%) androgen receptor gene mutations in a series of 59 patients with a 46,XY disorder of sex development". J. Clin. Endocrinol. Metab. 95 (4): 1876–88. doi:10.1210/jc.2009-2146. PMID 20150575.
- Lumbroso R, Beitel LK, Vasiliou DM, Trifiro MA, Pinsky L (November 1997). "Codon-usage variants in the polymorphic (GGN)n trinucleotide repeat of the human androgen receptor gene". Hum. Genet. 101 (1): 43–6. doi:10.1007/s004390050583. PMID 9385367. S2CID 24753862.
- Gottlieb B, Pinsky L, Beitel LK, Trifiro M (December 1999). "Androgen insensitivity". American Journal of Medical Genetics. 89 (4): 210–7. doi:10.1002/(SICI)1096-8628(19991229)89:4<210::AID-AJMG5>3.0.CO;2-P. PMID 10727996.
- Edwards A, Hammond HA, Jin L, Caskey CT, Chakraborty R (February 1992). "Genetic variation at five trimeric and tetrameric tandem repeat loci in four human population groups". Genomics. 12 (2): 241–53. doi:10.1016/0888-7543(92)90371-X. PMID 1740333.
- Casella R, Maduro MR, Lipshultz LI, Lamb DJ (November 2001). "Significance of the polyglutamine tract polymorphism in the androgen receptor". Urology. 58 (5): 651–6. doi:10.1016/S0090-4295(01)01401-7. PMID 11711330.
- Yeh SH, Chiu CM, Chen CL, Lu SF, Hsu HC, Chen DS, Chen PJ (April 2007). "Somatic mutations at the trinucleotide repeats of androgen receptor gene in male hepatocellular carcinoma". Int. J. Cancer. 120 (8): 1610–7. doi:10.1002/ijc.22479. PMID 17230529. S2CID 22184439.
- La Spada AR, Wilson EM, Lubahn DB, Harding AE, Fischbeck KH (July 1991). "Androgen receptor gene mutations in X-linked spinal and bulbar muscular atrophy". Nature. 352 (6330): 77–9. Bibcode:1991Natur.352...77S. doi:10.1038/352077a0. PMID 2062380. S2CID 1678351.
- Casella R, Maduro MR, Misfud A, Lipshultz LI, Yong EL, Lamb DJ (January 2003). "Androgen receptor gene polyglutamine length is associated with testicular histology in infertile patients". J. Urol. 169 (1): 224–7. doi:10.1016/s0022-5347(05)64073-6. PMID 12478141.
- Dowsing AT, Yong EL, Clark M, McLachlan RI, de Kretser DM, Trounson AO (August 1999). "Linkage between male infertility and trinucleotide repeat expansion in the androgen-receptor gene". Lancet. 354 (9179): 640–3. doi:10.1016/S0140-6736(98)08413-X. PMID 10466666. S2CID 1868372.
- Tut TG, Ghadessy FJ, Trifiro MA, Pinsky L, Yong EL (November 1997). "Long polyglutamine tracts in the androgen receptor are associated with reduced trans-activation, impaired sperm production, and male infertility". J. Clin. Endocrinol. Metab. 82 (11): 3777–82. doi:10.1210/jcem.82.11.4385. PMID 9360540.
- Lim HN, Chen H, McBride S, Dunning AM, Nixon RM, Hughes IA, Hawkins JR (March 2000). "Longer polyglutamine tracts in the androgen receptor are associated with moderate to severe undermasculinized genitalia in XY males". Hum. Mol. Genet. 9 (5): 829–34. doi:10.1093/hmg/9.5.829. PMID 10749991.
- Hiort O, Holterhus PM, Horter T, Schulze W, Kremke B, Bals-Pratsch M, Sinnecker GH, Kruse K (August 2000). "Significance of mutations in the androgen receptor gene in males with idiopathic infertility". J. Clin. Endocrinol. Metab. 85 (8): 2810–5. doi:10.1210/jcem.85.8.6713. PMID 10946887. S2CID 2071030.
- Kukuvitis A, Georgiou I, Bouba I, Tsirka A, Giannouli CH, Yapijakis C, Tarlatzis B, Bontis J, Lolis D, Sofikitis N, Papadimas J (June 2002). "Association of oestrogen receptor alpha polymorphisms and androgen receptor CAG trinucleotide repeats with male infertility: a study in 109 Greek infertile men". Int. J. Androl. 25 (3): 149–52. doi:10.1046/j.1365-2605.2002.00339.x. PMID 12031042.
- Davis-Dao CA, Tuazon ED, Sokol RZ, Cortessis VK (November 2007). "Male infertility and variation in CAG repeat length in the androgen receptor gene: a meta-analysis". J. Clin. Endocrinol. Metab. 92 (11): 4319–26. doi:10.1210/jc.2007-1110. PMID 17684052.
- Radpour R, Rezaee M, Tavasoly A, Solati S, Saleki A (2007). "Association of long polyglycine tracts (GGN repeats) in exon 1 of the androgen receptor gene with cryptorchidism and penile hypospadias in Iranian patients". J. Androl. 28 (1): 164–9. doi:10.2164/jandrol.106.000927. PMID 16957138.
- Aschim EL, Nordenskjöld A, Giwercman A, Lundin KB, Ruhayel Y, Haugen TB, Grotmol T, Giwercman YL (October 2004). "Linkage between cryptorchidism, hypospadias, and GGN repeat length in the androgen receptor gene". J. Clin. Endocrinol. Metab. 89 (10): 5105–9. doi:10.1210/jc.2004-0293. PMID 15472213.
- Rajender S, Rajani V, Gupta NJ, Chakravarty B, Singh L, Thangaraj K (2006). "No association of androgen receptor GGN repeat length polymorphism with infertility in Indian men". J. Androl. 27 (6): 785–9. doi:10.2164/jandrol.106.000166. PMID 16809273.
- Gottlieb B, Beitel LK, Trifiro MA (May 2001). "Variable expressivity and mutation databases: The androgen receptor gene mutations database". Hum. Mutat. 17 (5): 382–8. doi:10.1002/humu.1113. PMID 11317353. S2CID 2933566.
- Ozülker T, Ozpaçaci T, Ozülker F, Ozekici U, Bilgiç R, Mert M (January 2010). "Incidental detection of Sertoli-Leydig cell tumor by FDG PET/CT imaging in a patient with androgen insensitivity syndrome". Ann Nucl Med. 24 (1): 35–9. doi:10.1007/s12149-009-0321-x. PMID 19957213. S2CID 10450803.
- Köhler B, Lumbroso S, Leger J, Audran F, Grau ES, Kurtz F, Pinto G, Salerno M, Semitcheva T, Czernichow P, Sultan C (January 2005). "Androgen insensitivity syndrome: somatic mosaicism of the androgen receptor in seven families and consequences for sex assignment and genetic counseling". J. Clin. Endocrinol. Metab. 90 (1): 106–11. doi:10.1210/jc.2004-0462. PMID 15522944.
- Hiort O, Sinnecker GH, Holterhus PM, Nitsche EM, Kruse K (June 1998). "Inherited and de novo androgen receptor gene mutations: investigation of single-case families". J. Pediatr. 132 (6): 939–43. doi:10.1016/S0022-3476(98)70387-7. PMID 9627582.
- Batch JA, Williams DM, Davies HR, Brown BD, Evans BA, Hughes IA, Patterson MN (October 1992). "Androgen receptor gene mutations identified by SSCP in fourteen subjects with androgen insensitivity syndrome". Hum. Mol. Genet. 1 (7): 497–503. doi:10.1093/hmg/1.7.497. PMID 1307250.
- Hiort O, Klauber G, Cendron M, Sinnecker GH, Keim L, Schwinger E, Wolfe HJ, Yandell DW (May 1994). "Molecular characterization of the androgen receptor gene in boys with hypospadias". Eur. J. Pediatr. 153 (5): 317–21. doi:10.1007/BF01956409. PMID 8033918. S2CID 12862106.
- Lu J, Danielsen M (June 1996). "A Stu I polymorphism in the human androgen receptor gene (AR)". Clin. Genet. 49 (6): 323–4. doi:10.1111/j.1399-0004.1996.tb03800.x. PMID 8884086. S2CID 33645516.
- Macke JP, Hu N, Hu S, Bailey M, King VL, Brown T, Hamer D, Nathans J (October 1993). "Sequence variation in the androgen receptor gene is not a common determinant of male sexual orientation". American Journal of Human Genetics. 53 (4): 844–52. PMC 1682384. PMID 8213813.
- Gottlieb B, Vasiliou DM, Lumbroso R, Beitel LK, Pinsky L, Trifiro MA (1999). "Analysis of exon 1 mutations in the androgen receptor gene". Hum. Mutat. 14 (6): 527–39. doi:10.1002/(SICI)1098-1004(199912)14:6<527::AID-HUMU12>3.0.CO;2-X. PMID 10571951. S2CID 39155225.
- Ferlin A, Vinanzi C, Garolla A, Selice R, Zuccarello D, Cazzadore C, Foresta C (November 2006). "Male infertility and androgen receptor gene mutations: clinical features and identification of seven novel mutations". Clin. Endocrinol. 65 (5): 606–10. doi:10.1111/j.1365-2265.2006.02635.x. PMID 17054461. S2CID 33713391.
- Melo KF, Mendonca BB, Billerbeck AE, Costa EM, Inácio M, Silva FA, Leal AM, Latronico AC, Arnhold IJ (July 2003). "Clinical, hormonal, behavioral, and genetic characteristics of androgen insensitivity syndrome in a Brazilian cohort: five novel mutations in the androgen receptor gene". J. Clin. Endocrinol. Metab. 88 (7): 3241–50. doi:10.1210/jc.2002-021658. PMID 12843171.
- Ahmed SF, Cheng A, Dovey L, Hawkins JR, Martin H, Rowland J, Shimura N, Tait AD, Hughes IA (February 2000). "Phenotypic features, androgen receptor binding, and mutational analysis in 278 clinical cases reported as androgen insensitivity syndrome". J. Clin. Endocrinol. Metab. 85 (2): 658–65. doi:10.1210/jcem.85.2.6337. PMID 10690872.
- Coutant R, Mallet D, Lahlou N, Bouhours-Nouet N, Guichet A, Coupris L, Croué A, Morel Y (August 2007). "Heterozygous mutation of steroidogenic factor-1 in 46,XY subjects may mimic partial androgen insensitivity syndrome". J. Clin. Endocrinol. Metab. 92 (8): 2868–73. doi:10.1210/jc.2007-0024. PMID 17488792.
- Adachi M, Takayanagi R, Tomura A, Imasaki K, Kato S, Goto K, Yanase T, Ikuyama S, Nawata H (September 2000). "Androgen-insensitivity syndrome as a possible coactivator disease". N. Engl. J. Med. 343 (12): 856–62. doi:10.1056/NEJM200009213431205. PMID 10995865.
- Ghadessy FJ, Lim J, Abdullah AA, Panet-Raymond V, Choo CK, Lumbroso R, Tut TG, Gottlieb B, Pinsky L, Trifiro MA, Yong EL (June 1999). "Oligospermic infertility associated with an androgen receptor mutation that disrupts interdomain and coactivator (TIF2) interactions". J. Clin. Invest. 103 (11): 1517–25. doi:10.1172/JCI4289. PMC 408364. PMID 10359561.
- Giwercman YL, Ivarsson SA, Richthoff J, Lundin KB, Giwercman A (2004). "A novel mutation in the D-box of the androgen receptor gene (S597R) in two unrelated individuals Is associated with both normal phenotype and severe PAIS". Horm. Res. 61 (2): 58–62. doi:10.1159/000075240. PMID 14646391. S2CID 39208502.
- Achermann JC, Jameson JL (2006). "Disorders of sexual differentiation". In Hauser SL, Kasper DL, Fauci AS, Braunwald E, Longo DL (eds.). Harrison's endocrinology. New York: McGraw-Hill Medical Pub. Division. p. 161172. ISBN 978-0-07-145744-6.
- Simpson JL, Rebar RW (2002). Hung, Wellington, Becker, Kenneth L., Bilezikian, John P., William J Bremner (eds.). Principles and Practice of Endocrinology and Metabolism. Hagerstwon, MD: Lippincott Williams & Wilkins. pp. 852–85. ISBN 978-0-7817-4245-0.
- Brinkmann A, Jenster G, Ris-Stalpers C, van der Korput H, Brüggenwirth H, Boehmer A, Trapman J (April 1996). "Molecular basis of androgen insensitivity". Steroids. 61 (4): 172–5. doi:10.1016/0039-128X(96)00008-6. hdl:2066/22511. PMID 8732995. S2CID 34941122.
- Stone, Jon (January 31, 2015). "Woman born with no womb gives birth to twins after treatment breakthrough". The Independent. Retrieved July 7, 2022.
- Pinsky L, Kaufman M, Killinger DW (January 1989). "Impaired spermatogenesis is not an obligate expression of receptor-defective androgen resistance". American Journal of Medical Genetics. 32 (1): 100–4. doi:10.1002/ajmg.1320320121. PMID 2705470.
- Giwercman A, Kledal T, Schwartz M, Giwercman YL, Leffers H, Zazzi H, Wedell A, Skakkebaek NE (June 2000). "Preserved male fertility despite decreased androgen sensitivity caused by a mutation in the ligand-binding domain of the androgen receptor gene". J. Clin. Endocrinol. Metab. 85 (6): 2253–9. doi:10.1210/jcem.85.6.6626. PMID 10852459.
- Yong EL, Ng SC, Roy AC, Yun G, Ratnam SS (September 1994). "Pregnancy after hormonal correction of severe spermatogenic defect due to mutation in androgen receptor gene". Lancet. 344 (8925): 826–7. doi:10.1016/S0140-6736(94)92385-X. PMID 7993455. S2CID 34571405.
- Bouvattier C, Mignot B, Lefèvre H, Morel Y, Bougnères P (September 2006). "Impaired sexual activity in male adults with partial androgen insensitivity". J. Clin. Endocrinol. Metab. 91 (9): 3310–5. doi:10.1210/jc.2006-0218. PMID 16757528.
- Boehmer AL, Brinkmann O, Brüggenwirth H, van Assendelft C, Otten BJ, Verleun-Mooijman MC, Niermeijer MF, Brunner HG, Rouwé CW, Waelkens JJ, Oostdijk W, Kleijer WJ, van der Kwast TH, de Vroede MA, Drop SL (September 2001). "Genotype versus phenotype in families with androgen insensitivity syndrome". J. Clin. Endocrinol. Metab. 86 (9): 4151–60. doi:10.1210/jcem.86.9.7825. PMID 11549642.
- Evans BA, Hughes IA, Bevan CL, Patterson MN, Gregory JW (June 1997). "Phenotypic diversity in siblings with partial androgen insensitivity syndrome". Arch. Dis. Child. 76 (6): 529–31. doi:10.1136/adc.76.6.529. PMC 1717223. PMID 9245853.
- Werner R, Holterhus PM, Binder G, Schwarz HP, Morlot M, Struve D, Marschke C, Hiort O (September 2006). "The A645D mutation in the hinge region of the human androgen receptor (AR) gene modulates AR activity, depending on the context of the polymorphic glutamine and glycine repeats". J. Clin. Endocrinol. Metab. 91 (9): 3515–20. doi:10.1210/jc.2006-0372. PMID 16804045.
- Zenteno JC, Chávez B, Vilchis F, Kofman-Alfaro S (2002). "Phenotypic heterogeneity associated with identical mutations in residue 870 of the androgen receptor". Horm. Res. 57 (3–4): 90–3. doi:10.1159/000057958. PMID 12006704. S2CID 23484493.
- Holterhus PM, Werner R, Hoppe U, Bassler J, Korsch E, Ranke MB, Dörr HG, Hiort O (2005). "Molecular features and clinical phenotypes in androgen insensitivity syndrome in the absence and presence of androgen receptor gene mutations". J Mol Med. 83 (12): 1005–1113. doi:10.1007/s00109-005-0704-y. PMID 16283146. S2CID 7725163.
- Meehan KL, Sadar MD (May 2003). "Androgens and androgen receptor in prostate and ovarian malignancies". Front. Biosci. 8 (1–3): d780–800. doi:10.2741/1063. PMID 12700055.
- Wang Q, Ghadessy FJ, Trounson A, de Kretser D, McLachlan R, Ng SC, Yong EL (December 1998). "Azoospermia associated with a mutation in the ligand-binding domain of an androgen receptor displaying normal ligand binding, but defective trans-activation". J. Clin. Endocrinol. Metab. 83 (12): 4303–9. doi:10.1210/jcem.83.12.5358. PMID 9851768.
- Jin, Hong-Jian; Kim, Jung; Yu, Jindan (September 2013). "Androgen receptor genomic regulation". Translational Andrology and Urology. 2 (3): 15877–15177. doi:10.3978/j.issn.2223-4683.2013.09.01. ISSN 2223-4691. PMC 4165347. PMID 25237629.
- Jenster G, van der Korput HA, van Vroonhoven C, van der Kwast TH, Trapman J, Brinkmann AO (October 1991). "Domains of the human androgen receptor involved in steroid binding, transcriptional activation, and subcellular localization". Mol. Endocrinol. 5 (10): 1396–404. doi:10.1210/mend-5-10-1396. PMID 1775129.
- Simental JA, Sar M, Lane MV, French FS, Wilson EM (January 1991). "Transcriptional activation and nuclear targeting signals of the human androgen receptor". J. Biol. Chem. 266 (1): 510–8. doi:10.1016/S0021-9258(18)52466-2. PMID 1985913.
- Gilbert SF (2000). Developmental biology. Sunderland, Mass: Sinauer Associates. ISBN 978-0-87893-243-6.
- Jones RE, Lopez KH (2006). "Chapter 5: Sexual differentiation". Human reproductive biology. Amsterdam: Elsevier Academic Press. pp. 127–48. ISBN 978-0-12-088465-0.
- Yong EL, Loy CJ, Sim KS (2003). "Androgen receptor gene and male infertility". Hum. Reprod. Update. 9 (1): 1–7. doi:10.1093/humupd/dmg003. PMID 12638777.
- Hannema SE, Scott IS, Hodapp J, Martin H, Coleman N, Schwabe JW, Hughes IA (November 2004). "Residual activity of mutant androgen receptors explains wolffian duct development in the complete androgen insensitivity syndrome". J. Clin. Endocrinol. Metab. 89 (11): 5815–22. doi:10.1210/jc.2004-0709. PMID 15531547.
- Oakes MB, Eyvazzadeh AD, Quint E, Smith YR (December 2008). "Complete androgen insensitivity syndrome--a review". J Pediatr Adolesc Gynecol. 21 (6): 305–10. doi:10.1016/j.jpag.2007.09.006. PMID 19064222.
- Roy AK, Lavrovsky Y, Song CS, Chen S, Jung MH, Velu NK, Bi BY, Chatterjee B (1999). Regulation of androgen action. pp. 309–52. doi:10.1016/S0083-6729(08)60938-3. ISBN 978-0-12-709855-5. PMID 9949684.
{{cite book}}:|journal=ignored (help) - Kokontis JM, Liao S (1999). Molecular action of androgen in the normal and neoplastic prostate. pp. 219–307. doi:10.1016/s0083-6729(08)60937-1. ISBN 978-0127098555. PMID 9949683.
{{cite book}}:|journal=ignored (help) - Rajender S, Gupta NJ, Chakrabarty B, Singh L, Thangaraj K (March 2009). "Ala 586 Asp mutation in androgen receptor disrupts transactivation function without affecting androgen binding". Fertil. Steril. 91 (3): 933.e23–8. doi:10.1016/j.fertnstert.2008.10.041. PMID 19062009.
- Sobel V, Schwartz B, Zhu YS, Cordero JJ, Imperato-McGinley J (August 2006). "Bone mineral density in the complete androgen insensitivity and 5alpha-reductase-2 deficiency syndromes". J. Clin. Endocrinol. Metab. 91 (8): 3017–23. doi:10.1210/jc.2005-2809. PMID 16735493.
- Lund A, Juvonen V, Lähdetie J, Aittomäki K, Tapanainen JS, Savontaus ML (June 2003). "A novel sequence variation in the transactivation regulating domain of the androgen receptor in two infertile Finnish men". Fertil. Steril. 79. Suppl 3: 1647–8. doi:10.1016/s0015-0282(03)00256-5. PMID 12801573.
- Wooster R, Mangion J, Eeles R, Smith S, Dowsett M, Averill D, Barrett-Lee P, Easton DF, Ponder BA, Stratton MR (October 1992). "A germline mutation in the androgen receptor gene in two brothers with breast cancer and Reifenstein syndrome". Nat. Genet. 2 (2): 132–4. doi:10.1038/ng1092-132. PMID 1303262. S2CID 19780651.
- Evans BA, Harper ME, Daniells CE, Watts CE, Matenhelia S, Green J, Griffiths K (March 1996). "Low incidence of androgen receptor gene mutations in human prostatic tumors using single strand conformation polymorphism analysis". Prostate. 28 (3): 162–71. doi:10.1002/(SICI)1097-0045(199603)28:3<162::AID-PROS3>3.0.CO;2-H. PMID 8628719. S2CID 26338350.
- Lobaccaro JM, Lumbroso S, Belon C, Galtier-Dereure F, Bringer J, Lesimple T, Namer M, Cutuli BF, Pujol H, Sultan C (November 1993). "Androgen receptor gene mutation in male breast cancer". Hum. Mol. Genet. 2 (11): 1799–802. doi:10.1093/hmg/2.11.1799. PMID 8281139.
- Stenoien DL, Cummings CJ, Adams HP, Mancini MG, Patel K, DeMartino GN, Marcelli M, Weigel NL, Mancini MA (May 1999). "Polyglutamine-expanded androgen receptors form aggregates that sequester heat shock proteins, proteasome components and SRC-1, and are suppressed by the HDJ-2 chaperone". Hum. Mol. Genet. 8 (5): 731–41. doi:10.1093/hmg/8.5.731. PMID 10196362.
- Pérez-Palacios G, Chávez B, Méndez JP, McGinley JI, Ulloa-Aguirre A (1987). "The syndromes of androgen resistance revisited". J. Steroid Biochem. 27 (4–6): 1101–8. doi:10.1016/0022-4731(87)90196-8. PMID 3320547.
- Ismail-Pratt IS, Bikoo M, Liao LM, Conway GS, Creighton SM (July 2007). "Normalization of the vagina by dilator treatment alone in Complete Androgen Insensitivity Syndrome and Mayer-Rokitansky-Kuster-Hauser Syndrome". Hum. Reprod. 22 (7): 2020–4. doi:10.1093/humrep/dem074. PMID 17449508.
- Nichols JL, Bieber EJ, Gell JS (March 2009). "Case of sisters with complete androgen insensitivity syndrome and discordant Müllerian remnants". Fertility and Sterility. 91 (3): 932.e15–8. doi:10.1016/j.fertnstert.2008.09.027. PMID 18930210.
- Hannema SE, Scott IS, Rajpert-De Meyts E, Skakkebaek NE, Coleman N, Hughes IA (March 2006). "Testicular development in the complete androgen insensitivity syndrome". J. Pathol. 208 (4): 518–27. doi:10.1002/path.1890. PMID 16400621. S2CID 20730666.
- Zuccarello D, Ferlin A, Vinanzi C, Prana E, Garolla A, Callewaert L, Claessens F, Brinkmann AO, Foresta C (April 2008). "Detailed functional studies on androgen receptor mild mutations demonstrate their association with male infertility". Clin. Endocrinol. 68 (4): 580–8. doi:10.1111/j.1365-2265.2007.03069.x. PMID 17970778. S2CID 2783902.
- Weidemann W, Linck B, Haupt H, Mentrup B, Romalo G, Stockklauser K, Brinkmann AO, Schweikert HU, Spindler KD (December 1996). "Clinical and biochemical investigations and molecular analysis of subjects with mutations in the androgen receptor gene". Clin. Endocrinol. 45 (6): 733–9. doi:10.1046/j.1365-2265.1996.8600869.x. PMID 9039340. S2CID 28176593.
- Deeb A, Jääskeläinen J, Dattani M, Whitaker HC, Costigan C, Hughes IA (October 2008). "A novel mutation in the human androgen receptor suggests a regulatory role for the hinge region in amino-terminal and carboxy-terminal interactions". J. Clin. Endocrinol. Metab. 93 (10): 3691–6. doi:10.1210/jc.2008-0737. PMID 18697867.
- Quint EH, McCarthy JD, Smith YR (March 2010). "Vaginal surgery for congenital anomalies". Clin Obstet Gynecol. 53 (1): 115–24. doi:10.1097/GRF.0b013e3181cd4128. PMID 20142648. S2CID 41259739.
- Hughes IA (February 2008). "Disorders of sex development: a new definition and classification". Best Pract. Res. Clin. Endocrinol. Metab. 22 (1): 119–34. doi:10.1016/j.beem.2007.11.001. PMID 18279784.
- Kim KR, Kwon Y, Joung JY, Kim KS, Ayala AG, Ro JY (October 2002). "True hermaphroditism and mixed gonadal dysgenesis in young children: a clinicopathologic study of 10 cases". Mod. Pathol. 15 (10): 1013–9. doi:10.1097/01.MP.0000027623.23885.0D. PMID 12379746.
- Stouffs K, Tournaye H, Liebaers I, Lissens W (2009). "Male infertility and the involvement of the X chromosome". Hum. Reprod. Update. 15 (6): 623–37. doi:10.1093/humupd/dmp023. PMID 19515807.
- Kawate H, Wu Y, Ohnaka K, Tao RH, Nakamura K, Okabe T, Yanase T, Nawata H, Takayanagi R (November 2005). "Impaired nuclear translocation, nuclear matrix targeting, and intranuclear mobility of mutant androgen receptors carrying amino acid substitutions in the deoxyribonucleic acid-binding domain derived from androgen insensitivity syndrome patients". J. Clin. Endocrinol. Metab. 90 (11): 6162–9. doi:10.1210/jc.2005-0179. PMID 16118342.
- Sultan C, Paris F, Terouanne B, Balaguer P, Georget V, Poujol N, Jeandel C, Lumbroso S, Nicolas JC (2001). "Disorders linked to insufficient androgen action in male children". Hum. Reprod. Update. 7 (3): 314–22. doi:10.1093/humupd/7.3.314. PMID 11392378.
- Nistal, Manuel; González-Peramato, Pilar; Serrano, Álvaro (2017-03-07). Clues in the Diagnosis of Non-tumoral Testicular Pathology. Springer. p. 41. ISBN 978-3-319-49364-0.
- Bangsbøll S, Qvist I, Lebech PE, Lewinsky M (January 1992). "Testicular feminization syndrome and associated gonadal tumors in Denmark". Acta Obstet Gynecol Scand. 71 (1): 63–6. doi:10.3109/00016349209007950. PMID 1315102. S2CID 39727062.
- Mazen I, El-Ruby M, Kamal R, El-Nekhely I, El-Ghandour M, Tantawy S, El-Gammal M (2010). "Screening of genital anomalies in newborns and infants in two egyptian governorates". Horm Res Paediatr. 73 (6): 438–42. doi:10.1159/000313588. PMID 20407231. S2CID 22171345.
- "Diagnóstico Genético Preimplantacional: DGP". 25 April 2017.
- PGD conditions licensed by the HFEA Archived October 6, 2014, at the Wayback Machine, Human Fertilization and Embryology Authority, 1 October 2014. Retrieved on October 1, 2014.
- Sparrow R (2013). "Gender eugenics? The ethics of PGD for intersex conditions". Am J Bioeth. 13 (10): 29–38. doi:10.1080/15265161.2013.828115. PMID 24024804. S2CID 41857961.
- Behrmann J, Ravitsky V (2013). "Queer liberation, not elimination: why selecting against intersex is not "straight" forward". Am J Bioeth. 13 (10): 39–41. doi:10.1080/15265161.2013.828131. PMID 24024805. S2CID 27065247.
- Nisker J (2013). "Informed choice and PGD to prevent "intersex conditions"". Am J Bioeth. 13 (10): 47–9. doi:10.1080/15265161.2013.828125. PMID 24024809. S2CID 6085229.
- Wilkins L. (1950). "Heterosexual development". In: The diagnosis and treatment of endocrine disorders in childhood and adolescence. Springfield, IL: Charles C Thomas, pp. 256–79.
- Lyon MF, Hawkes SG (September 1970). "X-linked gene for testicular feminization in the mouse". Nature. 227 (5264): 1217–9. Bibcode:1970Natur.227.1217L. doi:10.1038/2271217a0. PMID 5452809. S2CID 4285996.
- Ohno S, Lyon MF (July 1970). "X-Linked testicular feminization in the mouse as a non-inducible regulatory mutation of the Jacob-Monod type". Clinical Genetics. 1 (3–4): 121–7. doi:10.1111/j.1399-0004.1970.tb01627.x. S2CID 85180199.
- Migeon BR, Brown TR, Axelman J, Migeon CJ (October 1981). "Studies of the locus for androgen receptor: localization on the human X chromosome and evidence for homology with the Tfm locus in the mouse". Proceedings of the National Academy of Sciences of the United States of America. 78 (10): 6339–43. Bibcode:1981PNAS...78.6339M. doi:10.1073/pnas.78.10.6339. PMC 349034. PMID 6947233.
- Brown TR, Lubahn DB, Wilson EM, Joseph DR, French FS, Migeon CJ (November 1988). "Deletion of the steroid-binding domain of the human androgen receptor gene in one family with complete androgen insensitivity syndrome: evidence for further genetic heterogeneity in this syndrome". Proceedings of the National Academy of Sciences of the United States of America. 85 (21): 8151–5. Bibcode:1988PNAS...85.8151B. doi:10.1073/pnas.85.21.8151. PMC 282385. PMID 3186717.
- Lubahn DB, Joseph DR, Sullivan PM, Willard HF, French FS, Wilson EM (April 1988). "Cloning of human androgen receptor complementary DNA and localization to the X chromosome". Science. 240 (4850): 327–30. Bibcode:1988Sci...240..327L. doi:10.1126/science.3353727. PMID 3353727.
- Chang CS, Kokontis J, Liao ST (April 1988). "Molecular cloning of human and rat complementary DNA encoding androgen receptors". Science. 240 (4850): 324–6. Bibcode:1988Sci...240..324C. doi:10.1126/science.3353726. PMID 3353726.
- Lubahn DB, Brown TR, Simental JA, Higgs HN, Migeon CJ, Wilson EM, French FS (December 1989). "Sequence of the intron/exon junctions of the coding region of the human androgen receptor gene and identification of a point mutation in a family with complete androgen insensitivity". Proceedings of the National Academy of Sciences of the United States of America. 86 (23): 9534–8. Bibcode:1989PNAS...86.9534L. doi:10.1073/pnas.86.23.9534. PMC 298531. PMID 2594783.
- Patterson MN, Hughes IA, Gottlieb B, Pinsky L (September 1994). "The androgen receptor gene mutations database". Nucleic Acids Res. 22 (17): 3560–2. PMC 308319. PMID 7937057.
- Simpson JY. (1839). "Hermaphroditism". In: Todd RB, ed. Cyclopaedia of Anatomy and Physiology, Vol II. London: Longman, Brown, Green, Longmans, & Roberts; 2: 684–738.
- King H (2007). Midwifery, obstetrics and the rise of gynaecology: the uses of a sixteenth-century compendium. Aldershot, Hants, England: Ashgate Pub. ISBN 978-0-7546-5396-7.
- Affaitati F [Affaitat]. De hermaphroditis. Venet. 1549.
- Panckoucke CL, ed. (1820). Dictionnaire des sciences médicales – biographie médicale. Vol. 1 (1st ed.). Paris: Panckoucke. p. 59.
- Paré A (1573). Des monstres et prodiges. Paris: Dupuys.
- Venette N [Vénitien Salocini]. Tableau de l'amour humain considéré dans l'état du mariage. A Parme: Chez Franc d'Amour 1687.
- Jacob G. Tractatus de hermaphroditis. London: E. Curll 1718.
- Saint Hilaire IG (1832–1836). Histoire générale et particulière des anomalies de l'organisation. Paris: J.-B. Baillière.
- Dorsey FY, Hsieh MH, Roth DR (March 2009). "46,XX SRY-negative true hermaphrodite siblings". Urology. 73 (3): 529–31. doi:10.1016/j.urology.2008.09.050. PMID 19038427.
- Verkauskas G, Jaubert F, Lortat-Jacob S, Malan V, Thibaud E, Nihoul-Fékété C (February 2007). "The long-term followup of 33 cases of true hermaphroditism: a 40-year experience with conservative gonadal surgery". J. Urol. 177 (2): 726–31, discussion 731. doi:10.1016/j.juro.2006.10.003. PMID 17222668.
- Hughes IA, Houk C, Ahmed SF, Lee PA (July 2006). "Consensus statement on management of intersex disorders". Arch. Dis. Child. 91 (7): 554–63. doi:10.1136/adc.2006.098319. PMC 2082839. PMID 16624884.
- Simmonds M (January 2007). "Was "variations of reproductive development" considered?". Arch. Dis. Child. 92 (1): 89. doi:10.1136/adc.2006.107797. PMC 2083124. PMID 17185456.
- Zannoni GF, Vellone VG, Cordisco EL, Sangiorgi E, Grimaldi ME, Neri C, Nanni L, Neri G (January 2010). "Morphology and immunophenotyping of a monolateral ovotestis in a 46,XderY/45,X mosaic individual with ambiguous genitalia". Int. J. Gynecol. Pathol. 29 (1): 33–8. doi:10.1097/PGP.0b013e3181b52e75. PMID 19952940.
- Feder EK, Karkazis K (2008). "What's in a name? The controversy over "disorders of sex development"". Hastings Cent Rep. 38 (5): 33–6. doi:10.1353/hcr.0.0062. PMID 18947138. S2CID 39697912.
- Reis E (2007). "Divergence or disorder?: the politics of naming intersex". Perspect. Biol. Med. 50 (4): 535–43. doi:10.1353/pbm.2007.0054. PMID 17951887. S2CID 17398380.
- Ruysch F (1709). Thesaurus anatomicus octavus. Amsterdam: Joannem Wolters. pp. 33, Plate II.
- Klebs E. Handbuch der pathologischen anatomie. Berlin: A. Hirschwald 1876; 1:718.
- Mencke JB, ed. Acta eruditorum anno mdccix. Leipzig: Joh. Grossii Haeredes, Joh. Frid. Gleditsch, & Frid. Groschuf. 1709; 28: 272–4.
- Müller JP, ed. Archiv für Anatomie, Physiologie und wissenschaftliche Medicin. Berlin: G. Eichler 1834, p. 171.
- Académie française. Complément du Dictionnaire de l'Académie française. Paris: Chez Firmin Didot Fréres 1843, p. 997.
- Ritter von Raiman JN, Edlen von Rosas A, Fischer SC, Wisgrill J, eds. Medicinische Jahrbücher des kaiserlich-königlichen österreichischen Staates (volume 22). Vienna: Carl Gerold 1840; 22: 380–4.
- Bertuch FJ, Schütz CG, eds. Allgemeine Literatur-Zeitung Issues 1–97. Leipzig 1815, pp. 257–60.
- Peschier A, Mozin DJ, eds. Supplément au dictionnaire complet des langues française et allemande de l'abbe Mozin. Paris: Stuttgart et Augsbourg 1859, p. 333.
- Morris JM (June 1953). "The syndrome of testicular feminization in male pseudohermaphrodites". Am. J. Obstet. Gynecol. 65 (6): 1192–1211. doi:10.1016/0002-9378(53)90359-7. PMID 13057950.
- Reifenstein EC Jr. (1947). "Hereditary familial hypogonadism". Proc Am Fed Clin Res. 3: 86. PMID 18909356.
- Goldberg MB, Maxwell A (May 1948). "Male pseudohermaphroditism proved by surgical exploration and microscopic examination; a case report with speculations concerning pathogenesis". J. Clin. Endocrinol. Metab. 8 (5): 367–79. doi:10.1210/jcem-8-5-367. PMID 18863968.
- Gilbert-Dreyfus S, Sabaoun CI, Belausch J (1957). "Etude d'un cas familial d'androgynoidisme avec hypospadias grave, gynecomastie et hyperoestrogenie". Ann. Endocrinol. 18: 93–101.
- Lubs HA Jr, Vilar O, Bergenstal DM (September 1959). "Familial male pseudohermaphrodism with labial testes and partial feminization: endocrine studies and genetic aspects". J. Clin. Endocrinol. Metab. 19 (9): 1110–20. doi:10.1210/jcem-19-9-1110. PMID 14418653.
- Morris JM, Mahesh VB (November 1963). "Further observations on the syndrome, "testicular feminization."". Am. J. Obstet. Gynecol. 87: 731–48. PMID 14085776.
- Rosewater S, Gwinup G, Hamwi JG (September 1965). "Familial gynecomastia". Annals of Internal Medicine. 63 (3): 377–85. doi:10.7326/0003-4819-63-3-377. PMID 14327504.
- Aiman J, Griffin JE, Gazak JM, Wilson JD, MacDonald PC (February 1979). "Androgen insensitivity as a cause of infertility in otherwise normal men". N. Engl. J. Med. 300 (5): 223–7. doi:10.1056/NEJM197902013000503. PMID 759869.
- Simpson JL (2008). "Male Pseudohermaphroditism Due to Androgen Insensitivity or 5α-Reductase Deficiency". Glob. Libr. Women's Med. doi:10.3843/GLOWM.10349.
{{cite book}}:|journal=ignored (help) - Hester JD (2004). "Intersex(e) und alternative Heilungsstrategien – Medizin, soziale Imperative und identitatsstiftende Gegengemeinschaften". Ethik Med. 16: 48–67. doi:10.1007/s00481-004-0284-3. S2CID 5933432.
- McPhaul MJ (1999). "Molecular defects of the androgen receptor". J. Steroid Biochem. Mol. Biol. 69 (1–6): 315–22. doi:10.1016/S0960-0760(99)00050-3. PMID 10419008. S2CID 1485903.
- Hoff TA, Fuqua SA (2000). "Steroid and nuclear receptor polymorphism variants in hormone resistance and hormone independence". In Miller MS, Cronin MT (eds.). Genetic polymorphisms and susceptibility to disease. Washington, DC: Taylor & Francis. p. 111. ISBN 978-0-7484-0822-1.
- Sultan C, Lumbroso S, Paris F, Jeandel C, Terouanne B, Belon C, Audran F, Poujol N, Georget V, Gobinet J, Jalaguier S, Auzou G, Nicolas JC (August 2002). "Disorders of androgen action". Semin. Reprod. Med. 20 (3): 217–28. doi:10.1055/s-2002-35386. PMID 12428202. S2CID 41205149.
- Tsukada T, Inoue M, Tachibana S, Nakai Y, Takebe H (October 1994). "An androgen receptor mutation causing androgen resistance in undervirilized male syndrome". J. Clin. Endocrinol. Metab. 79 (4): 1202–7. doi:10.1210/jcem.79.4.7962294. PMID 7962294.
- Chu J, Zhang R, Zhao Z, Zou W, Han Y, Qi Q, Zhang H, Wang JC, Tao S, Liu X, Luo Z (January 2002). "Male fertility is compatible with an Arg(840)Cys substitution in the AR in a large Chinese family affected with divergent phenotypes of AR insensitivity syndrome". J. Clin. Endocrinol. Metab. 87 (1): 347–51. doi:10.1210/jcem.87.1.8167. PMID 11788673.
- Meschede D, Horst J (May 1997). "The molecular genetics of male infertility". Mol. Hum. Reprod. 3 (5): 419–30. doi:10.1093/molehr/3.5.419. PMID 9239727.
- Hart P. "Orchids: My Intersex Adventure". hartflicker Moving Pictures. Archived from the original on 2017-12-11.
- Carter S (31 May 2014). "Challenging Perspectives: Interview Dalea". Vada Magazine. Retrieved 23 January 2017.
- Peikoff K (22 August 2014). "What It's Really Like to be Intersex". Cosmopolitan. Retrieved 23 January 2017.
- "All about 'Girl Comet'". Dalea Music. Archived from the original on 2016-12-25. Retrieved 2017-01-24.
- "International Fashion Model Hanne Gaby Odiele Reveals She is Intersex; Announces Partnership with interACT Advocates for Intersex Youth to Raise Awareness About the Importance of Human Rights Protections for Intersex People Worldwide" (PDF). interACT. January 23, 2017.
- Faye S, Balzary C, Wyman E, Jawara, Sobol S, Shelley N (2017). "Hanne Gaby Odiele". Dazed. No. 250. Archived from the original on 2018-09-07. Retrieved 2017-05-30.
- Suzuki, Koji (2015-10-06). "Chapter 11-12". Ring. Translated by Rohmer, Robert B.; Walley, Glynne. HarperCollins. ISBN 9780007331574.
- "I AM A GIRL! House M.D." YouTube. 2020-01-15. Retrieved 2022-07-01.
- "'Faking It' canceled; Carter Covington interview – Hollywood Reporter". The Hollywood Reporter. 2016-05-16. Archived from the original on 2016-05-16. Retrieved 2019-02-11.
What the show will really be known for is Lauren's coming out as intersex and being the first series regular who is intersex on television
- Kay A (16 September 2014). "'Faking It' Will Make LGBT History in Season 2". Bustle. Retrieved 2019-02-11.
- "Call the Midwife: What is Testicular Feminisation Syndrome?". Radio Times. Retrieved 2019-02-11.
- "Kitty Anderson – Reykjavík, Iceland". Interface Project. October 2017. Retrieved 2018-11-22.
- Amnesty International (October 25, 2016). "Understanding the 'i' in LGBTI". Retrieved 2018-11-22.
- "Eden Atwood". Montana Kids. Montana Office of Tourism. Retrieved 2021-10-23.
- Cole, Cheryl L. (2000). "One Chromosome Too Many?". In Kay Schaffer (ed.). The Olympics at the Millennium: Power, Politics, and the Games. Sidonie Smith. Rutgers UP. pp. 128–146. ISBN 9780813528205. Retrieved 2 March 2015.
- Miller, Susan (23 January 2017). "Model Hanne Gaby Odiele Reveals She Is Intersex". USA Today.
- "Model Hanne Gaby Odiele reveals she is intersex to 'break taboo'". BBC News. 24 January 2017.
- "#FairTreatment for Shanthi Soundarajan". Thappad. 2016.
- Joshi, Sonam. "Why We Should Join The Campaign Seeking Justice For Runner Shanthi Soundarajan". Huffingtonpost.in. Archived from the original on 2017-03-17. Retrieved 2017-03-02.
- Punt, Anne (August 28, 2014). "Duizenden Nederlanders passen niet in het biologische hokje man of vrouw". Vice. Retrieved 2017-01-12.
- Fogle, Asher (October 21, 2016). "Falling In Between: Inside the lives of intersex women". Good Housekeeping. Retrieved 2017-08-05.
- "Georgiann Davis". The Interface Project. November 7, 2012.
- Morrison, Sarah (30 November 2013). "Special report: Intersex women speak out to protect the next generation". The Independent. Archived from the original on 2022-05-07. Retrieved 19 November 2015.
- "About Tony". Briffa.org. 2012. Archived from the original on 2014-04-06. Retrieved 2020-12-28.
- Senate of Australia; Community Affairs References Committee (28 March 2013), Involuntary or coerced sterilisation of people with disabilities in Australia: Thursday 28 March 2013, Canberra
{{citation}}: CS1 maint: location missing publisher (link) - Retief, F P; Cilliers, J F G (2003). "Congenital eunuchism and Favorinus". South African Medical Journal. 93 (1): 73–76. PMID 12564336.
- Mason, H.J., Favorinus’ Disorder: Reifenstein’s Syndrome in Antiquity?, in Janus 66 (1978) 1–13.
- "We talk to intersex individual Dr Small Luk about her gender struggles". Time Out Hong Kong. Archived from the original on 2016-05-29. Retrieved 2020-12-28.
- "專訪:前跨性別難民Eliana(國際特赦組織香港分會人權雜誌春季號)Interview: Former Transgender Refugee Eliana (Amnesty International Hong Kong) Human Rights Magazine Spring Issue)". 28 April 2016.
- "Gender refugee hopes for NZ citizenship". 3 Degrees - TV3 New Zealand. 26 July 2015. Archived from the original on 25 December 2015. Retrieved 23 December 2015.
- Vesga, Alejandro (11 July 2015). "El purgatorio de una transgénero víctima de un pasaporte con sexo masculino".
- Wall, Sean Saifa (November 8, 2016). "Love, complexity and inter-sectionality". Intersex Day. Retrieved 2017-01-19.
- один, Номер. "Бурятский лучник полжизни провел в чужом теле". gazeta-n1.ru (in Russian). Retrieved 2022-05-30.