Broad-spectrum antibiotic
A broad-spectrum antibiotic is an antibiotic that acts on the two major bacterial groups, Gram-positive and Gram-negative,[1] or any antibiotic that acts against a wide range of disease-causing bacteria.[2] These medications are used when a bacterial infection is suspected but the group of bacteria is unknown (also called empiric therapy) or when infection with multiple groups of bacteria is suspected. This is in contrast to a narrow-spectrum antibiotic, which is effective against only a specific group of bacteria.[3] Although powerful, broad-spectrum antibiotics pose specific risks, particularly the disruption of native, normal bacteria and the development of antimicrobial resistance. An example of a commonly used broad-spectrum antibiotic is ampicillin.[3]

Bacterial targets
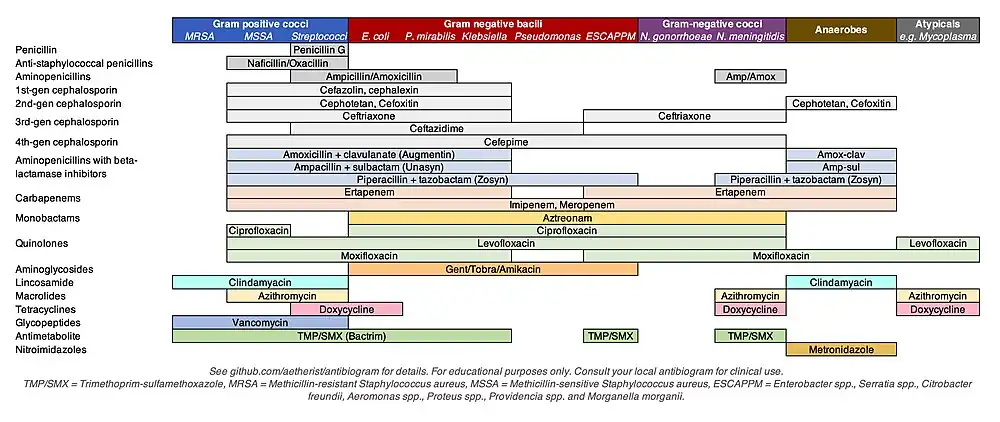
Antibiotics are often grouped by their ability to act on different bacterial groups. Although bacteria are biologically classified using taxonomy, disease-causing bacteria have historically been classified by their microscopic appearance and chemical function. The morphology of the organism may be classified as cocci, diplococci, bacilli (also known as "rods"), spiral-shaped or pleomorphic. Additional classification occurs through the organism's ability to take up the Gram stain and counter-stain; bacteria that take up the crystal violet dye stain are referred to as "gram-positive," those that take up the counterstain only are "gram-negative," and those that remain unstained are referred to as "atypical." Further classification includes their requirement for oxygen (i.e., aerobic or anaerobic), patterns of hemolysis, or other chemical properties. The most commonly encountered groupings of bacteria include gram-positive cocci, gram-negative bacilli, atypical bacteria, and anaerobic bacteria.[4] Antibiotics are often grouped by their ability to act on different bacterial groups. For example, 1st-generation cephalosporins are primarily effective against gram-positive bacteria, while 4th-generation cephalosporin s are generally effective against gram-negative bacteria.
Empiric antibiotic therapy
Empiric antibiotic therapy refers to the use of antibiotics to treat a suspected bacterial infection despite lack of a specific bacterial diagnosis. Definitive diagnosis of the species of bacteria often occurs through culture of blood, sputum, or urine, and can be delayed by 24 to 72 hours.[5] Antibiotics are generally given after the culture specimen has been taken from the patient in order to preserve the bacteria in the specimen and ensure accurate diagnosis.[4] Alternatively, some species may be identified through a urine or stool test.[4]
Risks
Disruption of normal microbiome
There are an estimated 38 trillion microorganisms that colonize the human body.[6] As a side-effect of therapy, antibiotics can change the body's normal microbial content by attacking indiscriminately both the pathological and naturally occurring, beneficial or harmless bacteria found in the intestines, lungs and bladder.[7] The destruction of the body's normal bacterial flora is thought to disrupt immunity, nutrition, and lead to a relative overgrowth in some bacteria or fungi.[8] An overgrowth of drug-resistant microorganisms can lead to a secondary infection such as Clostridioides difficile ("C. diff") or candidiasis ("thrush").[3] This side-effect is more likely with the use of broad-spectrum antibiotics, given their greater potential to disrupt a larger variety of normal human flora.[7] The use of doxycycline in acne vulgaris has been associated with increased risk of Crohn's disease.[9] Likewise, the use of minocycline in acne vulgaris has been associated with skin and gut dysbiosis.[10]
Examples of broad-spectrum antibiotics
In humans:
- Doxycycline
- Minocycline
- Aminoglycosides (except for streptomycin)
- Ampicillin
- Amoxicillin/clavulanic acid (Augmentin)[11]
- Azithromycin[12]
- Carbapenems (e.g. imipenem)
- Piperacillin/tazobactam
- Quinolones (e.g. ciprofloxacin)
- Tetracycline-class drugs (except sarecycline)
- Chloramphenicol
- Ticarcillin
Trimethoprim/sulfamethoxazole (Bactrim)
In veterinary medicine, co-amoxiclav, (in small animals); penicillin & streptomycin and oxytetracycline (in farm animals); penicillin and potentiated sulfonamides (in horses).
References
- Ory EM, Yow EM (July 1963). "The use and abuse of the broad spectrum antibiotics". JAMA. 185 (4): 273–9. doi:10.1001/jama.1963.03060040057022. PMID 13940450.
- Clayton L. Thomas, ed. (1993). Taber's Cyclopedic Medical Dictionary (17th ed.). F. A. Davis Co. ISBN 978-0-8036-8313-6.
- Hopkins SJ (1997). Drugs and Pharmacology for Nurses (12th ed.). Churchill Livingstone. ISBN 978-0-443-05249-1.
- Kasper DL, Larry Jameson J, Hauser SL, Loscalzo J, Fauci AS, Longo DL (2015-04-08). Harrison's principles of internal medicine (19th ed.). New York. ISBN 9780071802154. OCLC 893557976.
{{cite book}}: CS1 maint: location missing publisher (link) - Leekha S, Terrell CL, Edson RS (February 2011). "General principles of antimicrobial therapy". Mayo Clinic Proceedings. 86 (2): 156–67. doi:10.4065/mcp.2010.0639. PMC 3031442. PMID 21282489.
- Sender R, Fuchs S, Milo R (2016). "Revised Estimates for the Number of Human and Bacteria Cells in the Body". PLOS Biology. 14 (8): e1002533. doi:10.1371/journal.pbio.1002533. PMC 4991899. PMID 27541692.
- Martin EA (2003). Oxford Concise Medical Dictionary (6th ed.). Oxford University Press. ISBN 978-0-19-860753-3.
- Rafii F, Sutherland JB, Cerniglia CE (December 2008). "Effects of treatment with antimicrobial agents on the human colonic microflora". Therapeutics and Clinical Risk Management. 4 (6): 1343–58. doi:10.2147/tcrm.s4328. PMC 2643114. PMID 19337440.
- Margolis, David J.; Fanelli, Matthew; Hoffstad, Ole; Lewis, James D. (2010). "Potential association between the oral tetracycline class of antimicrobials used to treat acne and inflammatory bowel disease". The American Journal of Gastroenterology. 105 (12): 2610–2616. doi:10.1038/ajg.2010.303. ISSN 1572-0241. PMID 20700115. S2CID 20085592.
- Thompson, Katherine G.; Rainer, Barbara M.; Antonescu, Corina; Florea, Liliana; Mongodin, Emmanuel F.; Kang, Sewon; Chien, Anna L. (2020-02-01). "Minocycline and Its Impact on Microbial Dysbiosis in the Skin and Gastrointestinal Tract of Acne Patients". Annals of Dermatology. 32 (1): 21–30. doi:10.5021/ad.2020.32.1.21. ISSN 1013-9087. PMC 7992645. PMID 33911705.
- Coon ER, Quinonez RA, Morgan DJ, Dhruva SS, Ho T, Money N, Schroeder AR (April 2019). "2018 Update on Pediatric Medical Overuse: A Review". JAMA Pediatrics. 173 (4): 379–384. doi:10.1001/jamapediatrics.2018.5550. PMID 30776069. S2CID 73495617.
- McMullan BJ, Mostaghim M (June 2015). "Prescribing azithromycin". Australian Prescriber. 38 (3): 87–9. doi:10.18773/austprescr.2015.030. PMC 4653965. PMID 26648627.