Nociplastic pain
Nociplastic pain or central sensitisation is a type of pain which is mechanically different from the normal nociceptive pain caused by inflammation and tissue damage or the neuropathic pain which results from nerve damage. It may occur in combination with the other types of pain or in isolation. Its location may be generalised or multifocal and it can be more intense than would be expected from any associated physical cause.[3]
| Nociplastic pain | |
|---|---|
| Other names | Central sensitisation |
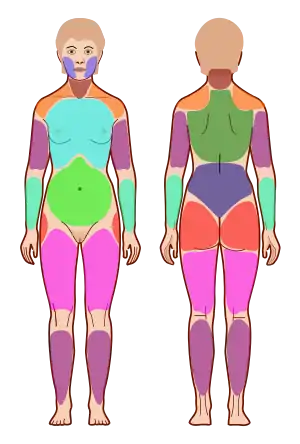 | |
| Fibromyalgia is the classic example of nociplastic pain,[1] being diagnosed when pain is felt in four different quadrants of the body using measures such as the Widespread Pain Index shown | |
| Specialty | Neurology |
| Duration | Short to long-term[2] |
| Diagnostic method | Clinical history, description of pain[3] |
| Treatment | Exercise, medication, psychological therapies, pain neuroscience education[4] |
Its causes are not fully understood but it is thought to be a dysfunction of the central nervous system whose processing of pain signals may have become distorted or sensitised.[3][5]
The concept and term was formally added to the taxonomy of the International Association for the Study of Pain following the recommendation of a task force in 2017.[6] The root terms are Latin nocēre, meaning to hurt, and Greek πλαστός, meaning development or formation in a medical context.
This type of pain typically arises in some chronic pain conditions, with the archetypal condition being fibromyalgia. It may be a factor in long COVID.[7][8] Exercise is commonly prescribed for such conditions.[9] Nociplastic pain has also been hypothesized to play a role in the persistence of medically unexplained symptoms.[5]
Definition
Nociplastic pain is a longterm complex pain, one of three mechanisms of pain, defined by the International Association for the Study of Pain as "pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing the pain".[2] The other two mechanisms are nociceptive pain and neuropathic pain.[2] Widespread pain and increased pain have been suggested as important clinical features.[2]
Central sensitization is a broader term referring to a hyperexcitability of the nervous system, usually including hyperalgesia (increased sensitivity to pain), and allodynia (painful perception of non-painful stimuli).[5]
An even broader term is that of central sensitivity syndromes, referring to syndromes characterized by the hyperexcitement of central neurons. These include fibromyalgia, irritable bowel syndrome, headaches, chronic fatigue syndrome[10] and temporomandibular disorder.[11]
Mechanism
Its causes are not fully understood but it is thought to be a dysfunction of the central nervous system whose processing of pain signals may have become distorted or sensitised.[3] Specific central nervous system locations that have been suggested are nociceptive neurons, spinal and supraspinal structures, the dorsal horn and others.[5]
Diagnosis
It is diagnosed by its clinical features and lack of response to regular painkillers.[3] Pain is experienced in several body parts, and is often widespread and intense.[3] There may be associated tiredness, and difficulties with memory, mood and sleep.[3] It can occur on its own in conditions such as tension headache or fibromyalgia, or combined with other pain categories such as in chronic back pain.[3]
Tools to measure central sensitization include sensory tests to painful stimuli, magnetic resonance imaging and measures of cytokines and neurotrophines in the blood and urine.[5] Self-report questionnaires such as the Central Sensitization Inventory[12] and the Sensory Hypersensitivity Scale[13] are also used.[5]
Treatment
Treatment generally requires both physical and psychological therapies, along with pain neuroscience education.[4]
References
- Chimenti RL, Frey-Law LA, Sluka KA (May 2018). "A Mechanism-Based Approach to Physical Therapist Management of Pain". Physical Therapy. 98 (5): 302–314. doi:10.1093/ptj/pzy030. PMC 6256939. PMID 29669091.
- Wåhlén K (2020). "Introduction: chronic pain". The pain profile in fibromyalgia: Painomic studies of pain characteristics and proteins in blood. Sweden: Linköping University. p. 9. ISBN 978-91-7929-783-1.
- Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W (May 2021). "Nociplastic pain: towards an understanding of prevalent pain conditions". Lancet. 397 (10289): 2098–2110. doi:10.1016/S0140-6736(21)00392-5. PMID 34062144. S2CID 235245552.
- Zafereo J (2020). "17. Physical therapy for pain management". In Noe CE (ed.). Pain Management for Clinicians: A Guide to Assessment and Treatment. Switzerland: Springer. pp. 445–448. ISBN 978-3-030-39982-5.
- den Boer, Carine; Dries, Linne; Terluin, Berend; van der Wouden, Johannes C.; Blankenstein, Annette H.; van Wilgen, C. Paul; Lucassen, Peter; van der Horst, Henriëtte E. (February 2019). "Central sensitization in chronic pain and medically unexplained symptom research: A systematic review of definitions, operationalizations and measurement instruments". Journal of Psychosomatic Research. 117: 32–40. doi:10.1016/j.jpsychores.2018.12.010. PMID 30665594. S2CID 58565532.
- IASP Council Adopts Task Force Recommendation for Third Mechanistic Descriptor of Pain, International Association for the Study of Pain, 14 November 2017
- Clauw DJ, Häuser W, Cohen SP, Fitzcharles MA (August 2020). "Considering the potential for an increase in chronic pain after the COVID-19 pandemic". Pain. 161 (8): 1694–1697. doi:10.1097/j.pain.0000000000001950. PMC 7302093. PMID 32701829.
- Linda Geddes (28 June 2021), "The pain that can't be seen – Sufferers of chronic pain have long been told it's all in their head. We now know that's wrong", The Guardian
- Ferro Moura Franco K, Lenoir D, Dos Santos Franco YR, Jandre Reis FJ, Nunes Cabral CM, Meeus M (January 2021). "Prescription of exercises for the treatment of chronic pain along the continuum of nociplastic pain: A systematic review with meta-analysis". European Journal of Pain. 25 (1): 51–70. doi:10.1002/ejp.1666. hdl:10067/1726510151162165141. PMID 32976664. S2CID 221937920.
- Yunus, Muhammad B. (June 2007). "Fibromyalgia and Overlapping Disorders: The Unifying Concept of Central Sensitivity Syndromes". Seminars in Arthritis and Rheumatism. 36 (6): 339–356. doi:10.1016/j.semarthrit.2006.12.009. PMID 17350675.
- Mezhov, Veronica; Guymer, Emma; Littlejohn, Geoffrey (December 2021). "Central sensitivity and fibromyalgia". Internal Medicine Journal. 51 (12): 1990–1998. doi:10.1111/imj.15430. ISSN 1444-0903. PMID 34139045. S2CID 235471910.
- Scerbo, Thomas; Colasurdo, Joseph; Dunn, Sally; Unger, Jacob; Nijs, Jo; Cook, Chad (April 2018). "Measurement Properties of the Central Sensitization Inventory: A Systematic Review". Pain Practice. 18 (4): 544–554. doi:10.1111/papr.12636. PMID 28851012. S2CID 206247498.
- Dixon, Eric A.; Benham, Grant; Sturgeon, John A.; Mackey, Sean; Johnson, Kevin A.; Younger, Jarred (June 2016). "Development of the Sensory Hypersensitivity Scale (SHS): a self-report tool for assessing sensitivity to sensory stimuli". Journal of Behavioral Medicine. 39 (3): 537–550. doi:10.1007/s10865-016-9720-3. ISSN 0160-7715. PMC 4854764. PMID 26873609.