Electromagnetic radiation and health
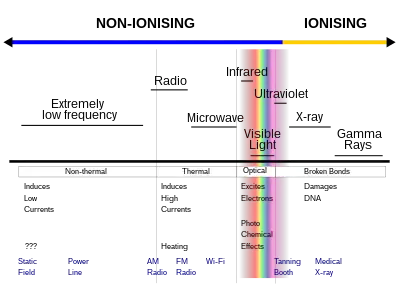
Electromagnetic radiation can be classified into two types: ionizing radiation and non-ionizing radiation, based on the capability of a single photon with more than 10 eV energy to ionize atoms or break chemical bonds.[1] Extreme ultraviolet and higher frequencies, such as X-rays or gamma rays are ionizing, and these pose their own special hazards: see radiation poisoning.
| Part of a series on |
| Pollution |
|---|
 |
The most common health hazard of radiation is sunburn, which causes between approximately 100,000 and 1 million new skin cancers annually in the United States.[2][3]
In 2011, the World Health Organization (WHO) and the International Agency for Research on Cancer (IARC) have classified radiofrequency electromagnetic fields as possibly carcinogenic to humans (Group 2B).[4]
Hazards
Dielectric heating from electromagnetic fields can create a biological hazard. For example, touching or standing around an antenna while a high-power transmitter is in operation can cause burns (the mechanism is the same as that used in a microwave oven).[5]
The heating effect varies with the power and the frequency of the electromagnetic energy, as well as the inverse square of distance to the source. The eyes and testes are particularly susceptible to radio frequency heating due to the paucity of blood flow in these areas that could otherwise dissipate the heat buildup.[6]
Radio frequency (RF) energy at power density levels of 1–10 mW/cm2 or higher can cause measurable heating of tissues. Typical RF energy levels encountered by the general public are well below the level needed to cause significant heating, but certain workplace environments near high power RF sources may exceed safe exposure limits.[6] A measure of the heating effect is the specific absorption rate or SAR, which has units of watts per kilogram (W/kg). The IEEE[7] and many national governments have established safety limits for exposure to various frequencies of electromagnetic energy based on SAR, mainly based on ICNIRP Guidelines,[8] which guard against thermal damage.
Low-level exposure
The World Health Organization (WHO) began a research effort in 1996 to study the health effects from the ever-increasing exposure of people to a diverse range of EMR sources. In 2011, the WHO/International Agency for Research on Cancer (IARC) has classified radiofrequency electromagnetic fields as possibly carcinogenic to humans (Group 2B), based on an increased risk for glioma, a malignant type of brain cancer, associated with wireless phone use.
Epidemiological studies look for statistical correlations between EM exposure in the field and specific health effects. As of 2019, much of the current work is focused on the study of EM fields in relation to cancer.[9] There are publications which support the existence of complex biological and neurological effects of weaker non-thermal electromagnetic fields (see Bioelectromagnetics), including weak ELF electromagnetic fields[10][11] and modulated RF and microwave fields.[12][13]
Effects by frequency
_(2).jpg.webp)
While the most acute exposures to harmful levels of electromagnetic radiation are immediately realized as burns, the health effects due to chronic or occupational exposure may not manifest effects for months or years.[14][15][3][16]
Extremely low frequency
Extremely low frequency EM waves can span from 0 Hz to 3 kHz, though definitions vary across disciplines. The maximum recommended exposure for the general public is 5 kV/m.[17]
ELF waves around 50 Hz to 60 Hz are emitted by power generators, transmission lines and distribution lines, power cables, and electric appliances. Typical household exposure to ELF waves ranges in intensity from 5 V/m for a light bulb to 180 V/m for a stereo, measured at 30 centimetres (12 in) and using 240V power.[17] (120V power systems would be unable to reach this intensity unless an appliance has an internal voltage transformer.) Overhead power lines range from 1kV for local distribution to 1,150 kV for ultra high voltage lines. These can produce electric fields up to 10kV/m on the ground directly underneath, but 50 m to 100 m away these levels return to approximately ambient.[17] Metal equipment must be maintained at a safe distance from energized high-voltage lines.[18]
Exposure to ELF waves can induce an electric current. Because the human body is conductive, electric currents and resulting voltages differences typically accumulate on the skin but do not reach interior tissues.[19] People can start to perceive high-voltage charges as tingling when hair or clothing in contact with the skin stands up or vibrates.[19] In scientific tests, only about 10% of people could detect a field intensity in the range of 2-5 kV/m.[19] Such voltage differences can also create electric sparks, similar to a discharge of static electricity when nearly touching a grounded object. When receiving such a shock at 5 kV/m, it was reported as painful by only 7% of test participants and by 50% of participants at 10 kV/m.[19]
The International Agency for Research on Cancer (IARC) finds "inadequate evidence" for human carcinogenicity.[20]
Shortwave
Shortwave (1.6 to 30 MHz) diathermy (where EM waves are used to produce heat) can be used as a therapeutic technique for its analgesic effect and deep muscle relaxation, but has largely been replaced by ultrasound. Temperatures in muscles can increase by 4–6 °C, and subcutaneous fat by 15 °C. The FCC has restricted the frequencies allowed for medical treatment, and most machines in the US use 27.12 MHz.[21] Shortwave diathermy can be applied in either continuous or pulsed mode. The latter came to prominence because the continuous mode produced too much heating too rapidly, making patients uncomfortable. The technique only heats tissues that are good electrical conductors, such as blood vessels and muscle. Adipose tissue (fat) receives little heating by induction fields because an electrical current is not actually going through the tissues.[22]
Studies have been performed on the use of shortwave radiation for cancer therapy and promoting wound healing, with some success. However, at a sufficiently high energy level, shortwave energy can be harmful to human health, potentially causing damage to biological tissues, for example by overheating or inducing electrical currents.[23] The FCC limits for maximum permissible workplace exposure to shortwave radio frequency energy in the range of 3–30 MHz has a plane-wave equivalent power density of (900/f2) mW/cm2 where f is the frequency in MHz, and 100 mW/cm2 from 0.3 to 3.0 MHz. For uncontrolled exposure to the general public, the limit is 180/f2 between 1.34 and 30 MHz.[6]
Radio and microwave frequencies
The designation of mobile phone signals as "possibly carcinogenic to humans" by the World Health Organization (WHO) (e.g. its IARC, see below) has often been misinterpreted as indicating that some measure of risk has been observed – however the designation indicates only that the possibility could not be conclusively ruled out using the available data.[24]
In 2011, International Agency for Research on Cancer (IARC) classified mobile phone radiation as Group 2B "possibly carcinogenic" (rather than Group 2A "probably carcinogenic" nor the "is carcinogenic" Group 1). That means that there "could be some risk" of carcinogenicity, so additional research into the long-term, heavy use of mobile phones needs to be conducted.[25] The WHO concluded in 2014 that "A large number of studies have been performed over the last two decades to assess whether mobile phones pose a potential health risk. To date, no adverse health effects have been established as being caused by mobile phone use."[26][27]
Since 1962, the microwave auditory effect or tinnitus has been shown from radio frequency exposure at levels below significant heating.[28] Studies during the 1960s in Europe and Russia claimed to show effects on humans, especially the nervous system, from low energy RF radiation; the studies were disputed at the time.[29][30]
In 2019, reporters from the Chicago Tribune tested the level of radiation from smartphones and found that certain models emitted more than reported by the manufacturers and in some cases more than the U.S. Federal Communications Commission exposure limit. It is unclear if this resulted in any harm to consumers. Some problems apparently involved the phone's ability to detect proximity to a human body and lower the radio power. In response, the FCC began testing some phones itself rather than relying solely on manufacturer certifications.[31]
Microwave and other radio frequencies cause heating, and this can cause burns or eye damage if delivered in high intensity,[32] or hyperthermia as with any powerful heat source. Microwave ovens use this form of radiation, and have shielding to prevent it from leaking out and unintentionally heating nearby objects or people.
Millimeter waves
In 2009, the US TSA introduced full-body scanners as a primary screening modality in airport security, first as backscatter X-ray scanners, which use ionizing radiation and which the European Union banned in 2011 due to health and safety concerns. These were followed by non-ionizing millimeter wave scanners.[33] Likewise WiGig for personal area networks have opened the 60 GHz and above microwave band to SAR exposure regulations. Previously, microwave applications in these bands were for point-to-point satellite communication with minimal human exposure.[34]
Infrared
Infrared wavelengths longer than 750 nm can produce changes in the lens of the eye. Glassblower's cataract is an example of a heat injury that damages the anterior lens capsule among unprotected glass and iron workers. Cataract-like changes can occur in workers who observe glowing masses of glass or iron without protective eyewear for prolonged periods over many years.[14]
Exposing skin to infrared radiation near visible light (IR-A) leads to increased production of free radicals.[35] Short-term exposure can be beneficial (activating protective responses), while prolonged exposure can lead to photoaging.[36]
Another important factor is the distance between the worker and the source of radiation. In the case of arc welding, infrared radiation decreases rapidly as a function of distance, so that farther than three feet away from where welding takes place, it does not pose an ocular hazard anymore but, ultraviolet radiation still does. This is why welders wear tinted glasses and surrounding workers only have to wear clear ones that filter UV.
Visible light
Photic retinopathy is damage to the macular area of the eye's retina that results from prolonged exposure to sunlight, particularly with dilated pupils. This can happen, for example, while observing a solar eclipse without suitable eye protection. The Sun's radiation creates a photochemical reaction that can result in visual dazzling and a scotoma. The initial lesions and edema will disappear after several weeks, but may leave behind a permanent reduction in visual acuity.[37]
Moderate and high-power lasers are potentially hazardous because they can burn the retina of the eye, or even the skin. To control the risk of injury, various specifications – for example ANSI Z136 in the US, EN 60825-1/A2 in Europe, and IEC 60825 internationally – define "classes" of lasers depending on their power and wavelength.[38][39] Regulations prescribe required safety measures, such as labeling lasers with specific warnings, and wearing laser safety goggles during operation (see laser safety).
As with its infrared and ultraviolet radiation dangers, welding creates an intense brightness in the visible light spectrum, which may cause temporary flash blindness. Some sources state that there is no minimum safe distance for exposure to these radiation emissions without adequate eye protection.[40]
Ultraviolet
Sunlight includes sufficient ultraviolet power to cause sunburn within hours of exposure, and the burn severity increases with the duration of exposure. This effect is a response of the skin called erythema, which is caused by a sufficient strong dose of UV-B. The Sun's UV output is divided into UV-A and UV-B: solar UV-A flux is 100 times that of UV-B, but the erythema response is 1,000 times higher for UV-B. This exposure can increase at higher altitudes and when reflected by snow, ice, or sand. The UV-B flux is 2–4 times greater during the middle 4–6 hours of the day, and is not significantly absorbed by cloud cover or up to a meter of water.[41]
Ultraviolet light, specifically UV-B, has been shown to cause cataracts and there is some evidence that sunglasses worn at an early age can slow its development in later life.[15] Most UV light from the sun is filtered out by the atmosphere and consequently airline pilots often have high rates of cataracts because of the increased levels of UV radiation in the upper atmosphere.[42] It is hypothesized that depletion of the ozone layer and a consequent increase in levels of UV light on the ground may increase future rates of cataracts.[43] Note that the lens filters UV light, so if it is removed via surgery, one may be able to see UV light.[44][45]
Prolonged exposure to ultraviolet radiation from the sun can lead to melanoma and other skin malignancies.[3] Clear evidence establishes ultraviolet radiation, especially the non-ionizing medium wave UVB, as the cause of most non-melanoma skin cancers, which are the most common forms of cancer in the world.[3] UV rays can also cause wrinkles, liver spots, moles, and freckles. In addition to sunlight, other sources include tanning beds, and bright desk lights. Damage is cumulative over one's lifetime, so that permanent effects may not be evident for some time after exposure.[16]
Ultraviolet radiation of wavelengths shorter than 300 nm (actinic rays) can damage the corneal epithelium. This is most commonly the result of exposure to the sun at high altitude, and in areas where shorter wavelengths are readily reflected from bright surfaces, such as snow, water, and sand. UV generated by a welding arc can similarly cause damage to the cornea, known as "arc eye" or welding flash burn, a form of photokeratitis.[46]

Fluorescent light bulbs and tubes internally produce ultraviolet light. Normally this is converted to visible light by the phosphor film inside a protective coating. When the film is cracked by mishandling or faulty manufacturing then UV may escape at levels that could cause sunburn or even skin cancer.[47][48]
Regulation
In the United States, nonionizing radiation is regulated in the Radiation Control for Health and Safety Act of 1968 and the Occupational Safety and Health Act of 1970.[49]
See also
- Background radiation
- Bioinitiative Report
- Biological effects of radiation on the epigenome
- Central nervous system effects from radiation exposure during spaceflight
- Cosmic ray
- COSMOS cohort study
- Electromagnetic hypersensitivity
- Electromagnetism
- EMF measurement
- Health threat from cosmic rays
- Light ergonomics
- Magnetobiology
- Microwave
- Wireless device radiation and health
- Personal RF safety monitor
- Specific absorption rate
References
- Cleveland Jr RF, Ulcek JL (August 1999). Questions and Answers about Biological Effects and Potential Hazards of Radiofrequency Electromagnetic Fields (PDF) (4th ed.). Washington, D.C.: OET (Office of Engineering and Technology) Federal Communications Commission. Archived (PDF) from the original on 30 June 2019. Retrieved 29 January 2019.
- Siegel RL, Miller KD, Jemal A (January 2020). "Cancer statistics, 2020". CA: A Cancer Journal for Clinicians. 70 (1): 7–30. doi:10.3322/caac.21590. PMID 31912902.
- Cleaver JE, Mitchell DL (2000). "15. Ultraviolet Radiation Carcinogenesis". In Bast RC, Kufe DW, Pollock RE, et al. (eds.). Holland-Frei Cancer Medicine (5th ed.). Hamilton, Ontario: B.C. Decker. ISBN 1-55009-113-1. Archived from the original on 4 September 2015. Retrieved 31 January 2011.
- Gaudin, Ph.D., Nicolas (31 May 2011). "IARC Classifies Radiofrequency Electromagnetic Fields As Possibly Carcinogenic to Humans" (PDF). International Agency for Research on Cancer. Archived (PDF) from the original on 4 April 2012. Retrieved 20 November 2021.
- Barnes FS, Greenebaum B, eds. (2018). Biological and Medical Aspects of Electromagnetic Fields (3 ed.). CRC Press. p. 378. ISBN 978-1420009460. Archived from the original on 4 January 2021. Retrieved 29 January 2019.
- Cleveland Jr RF, Ulcek JL (August 1999). "Questions and Answers about Biological Effects and Potential Hazards of Radiofrequency Electromagnetic Fields" (PDF). OET Bulletin 56 (Fourth ed.). Office of Engineering and Technology, Federal Communications Commission. p. 7. Archived (PDF) from the original on 30 June 2019. Retrieved 2 February 2019.
- "Standard for Safety Level with Respect to Human Exposure to Radio Frequency Electromagnetic Fields, 3KHz to 300GHz". IEEE STD. IEEE. C95.1-2005. October 2005. Archived from the original on 7 May 2015. Retrieved 23 May 2015.
- International Commission on Non-Ionizing Radiation Protection (April 1998). "Guidelines for limiting exposure to time-varying electric, magnetic, and electromagnetic fields (up to 300 GHz). International Commission on Non-Ionizing Radiation Protection" (PDF). Health Physics. 74 (4): 494–522. PMID 9525427. Archived from the original (PDF) on 13 November 2008.
- "What are electromagnetic fields? – Summary of health effects". World Health Organization. Archived from the original on 16 October 2019. Retrieved 7 February 2019.
- Delgado JM, Leal J, Monteagudo JL, Gracia MG (May 1982). "Embryological changes induced by weak, extremely low frequency electromagnetic fields". Journal of Anatomy. 134 (Pt 3): 533–551. PMC 1167891. PMID 7107514.
- Harland JD, Liburdy RP (1997). "Environmental magnetic fields inhibit the antiproliferative action of tamoxifen and melatonin in a human breast cancer cell line". Bioelectromagnetics. 18 (8): 555–562. doi:10.1002/(SICI)1521-186X(1997)18:8<555::AID-BEM4>3.0.CO;2-1. PMID 9383244. Archived from the original on 16 December 2019. Retrieved 29 June 2019.
- Aalto S, Haarala C, Brück A, Sipilä H, Hämäläinen H, Rinne JO (July 2006). "Mobile phone affects cerebral blood flow in humans". Journal of Cerebral Blood Flow and Metabolism. 26 (7): 885–890. doi:10.1038/sj.jcbfm.9600279. PMID 16495939.
- Pall ML (September 2016). "Microwave frequency electromagnetic fields (EMFs) produce widespread neuropsychiatric effects including depression". Journal of Chemical Neuroanatomy. 75 (Pt B): 43–51. doi:10.1016/j.jchemneu.2015.08.001. PMID 26300312.
- Fry LL, Garg A, Guitérrez-Camona F, Pandey SK, Tabin G, eds. (2004). Clinical Practice in Small Incision Cataract Surgery. CRC Press. p. 79. ISBN 0203311825. Archived from the original on 15 December 2019. Retrieved 31 January 2019.
- Sliney DH (1994). "UV radiation ocular exposure dosimetry". Documenta Ophthalmologica. Advances in Ophthalmology. 88 (3–4): 243–254. doi:10.1007/bf01203678. PMID 7634993. S2CID 8242055.
- "UV Exposure & Your Health". UV Awareness. Archived from the original on 2 May 2019. Retrieved 10 March 2014.
- World Health Organization (4 August 2016). "Radiation: Electromagnetic fields - Q&A". Archived from the original on 18 January 2022. Retrieved 21 January 2022.
- Ubong Edet (6 December 2017). "How to identify powerline voltage level and safe clearance level". Archived from the original on 12 May 2021. Retrieved 21 January 2022.
- Extremely Low Frequency Fields Environmental Health Criteria Monograph No.238, chapter 5, page 121, WHO
- "Power Lines, Electrical Devices, and Extremely Low Frequency Radiation". Archived from the original on 11 April 2020. Retrieved 22 April 2020.
- Fishman S, Ballantyne J, Rathmell JP, eds. (2010). Bonica's Management of Pain. Lippincott Williams & Wilkins. p. 1589. ISBN 978-0781768276. Archived from the original on 18 August 2021. Retrieved 1 February 2019.
- Knight KL, Draper DO (2008). Therapeutic Modalities: The Art and the Science. Lippincott Williams & Wilkins. p. 288. ISBN 978-0781757447. Archived from the original on 15 December 2019. Retrieved 1 February 2019.
- Yu C, Peng RY (2017). "Biological effects and mechanisms of shortwave radiation: a review". Military Medical Research. 4: 24. doi:10.1186/s40779-017-0133-6. PMC 5518414. PMID 28729909.
- Boice JD, Tarone RE (August 2011). "Cell phones, cancer, and children". Journal of the National Cancer Institute. 103 (16): 1211–1213. doi:10.1093/jnci/djr285. PMID 21795667.
- "IARC classifies radiofrequency electromagnetic fields as possibly carcinogenic to humans" (PDF). press release N° 208 (Press release). International Agency for Research on Cancer. 31 May 2011. Archived (PDF) from the original on 1 June 2011. Retrieved 2 June 2011.
- "Electromagnetic fields and public health: mobile phones – Fact sheet N°193". World Health Organization. October 2014. Archived from the original on 6 August 2016. Retrieved 2 August 2016.
- Limits of Human Exposure to Radiofrequency Electromagnetic Fields in the Frequency Range from 3 kHz to 300 GHz Archived 29 October 2013 at the Wayback Machine, Canada Safety Code 6, p. 63
- Frey AH (July 1962). "Human auditory system response to modulated electromagnetic energy". Journal of Applied Physiology. 17 (4): 689–692. doi:10.1152/jappl.1962.17.4.689. PMID 13895081. S2CID 12359057.
- Bergman W (1965), The Effect of Microwaves on the Central Nervous System (trans. from German) (PDF), Ford Motor Company, pp. 1–77, archived from the original (PDF) on 29 March 2018, retrieved 19 December 2018
- Michaelson SM (1975). "Radio-Frequency and Microwave Energies, Magnetic and Electric Fields" (Volume II Book 2 of Foundations of Space Biology and Medicine). In Calvin M, Gazenko OG (eds.). Ecological and Physiological Bases of Space Biology and Medicine. Washington, D.C.: NASA Scientific and Technical Information Office. pp. 409–452 [427–430]. Archived (PDF) from the original on 7 March 2017. Retrieved 19 December 2018.
- Sam Roe (21 August 2019). "We tested popular cellphones for radiofrequency radiation. Now the FCC is investigating". Chicago Tribune.
- "Microwaves, Radio Waves, and Other Types of Radiofrequency Radiation." American Cancer Society, http://www.cancer.org/cancer/cancer-causes/radiation-exposure/radiofrequency-radiation.html Archived 2 May 2020 at the Wayback Machine
- Khan FN (18 December 2017). "Is That Airport Security Scanner Really Safe?". Scientific American. Archived from the original on 17 December 2019. Retrieved 28 March 2020.
- "Characterization of 60GHz Millimeter-Wave Focusing Beam for Living-Body Exposure Experiments, Tokyo Institute of Technology, Masaki KOUZAI et al., 2009" (PDF). Archived (PDF) from the original on 1 February 2014. Retrieved 18 January 2014.
- Schieke SM, Schroeder P, Krutmann J (October 2003). "Cutaneous effects of infrared radiation: from clinical observations to molecular response mechanisms". Photodermatology, Photoimmunology & Photomedicine. 19 (5): 228–234. doi:10.1034/j.1600-0781.2003.00054.x. PMID 14535893.
- Tsai SR, Hamblin MR (May 2017). "Biological effects and medical applications of infrared radiation". Journal of Photochemistry and Photobiology B: Biology. 170: 197–207. doi:10.1016/j.jphotobiol.2017.04.014. PMC 5505738. PMID 28441605.
- Sullivan JB, Krieger GR, eds. (2001). Clinical Environmental Health and Toxic Exposures. Lippincott Williams & Wilkins. p. 275. ISBN 978-0683080278.
- "Laser Standards and Classifications". Rockwell Laser Industries. Archived from the original on 8 April 2017. Retrieved 10 February 2019.
- "An Overview of the LED and Laser Classification System in EN 60825-1 and IEC 60825-1". Lasermet. Archived from the original on 12 February 2019. Retrieved 10 February 2019.
- "What is the minimum safe distance from the welding arc above which there is no risk of eye damage?". The Welding Institute (TWI Global). Archived from the original on 10 March 2014. Retrieved 10 March 2014.
- James WD, Elston D, Berger T (2011). SPEC – Andrews' Diseases of the Skin (11 ed.). Elsevier Health Sciences. pp. 23–24. ISBN 978-1437736199.
- Rafnsson V, Olafsdottir E, Hrafnkelsson J, Sasaki H, Arnarsson A, Jonasson F (August 2005). "Cosmic radiation increases the risk of nuclear cataract in airline pilots: a population-based case-control study". Archives of Ophthalmology. 123 (8): 1102–1105. doi:10.1001/archopht.123.8.1102. PMID 16087845.
- Dobson R (2005). "Ozone depletion will bring big rise in number of cataracts". BMJ. 331 (7528): 1292–1295. doi:10.1136/bmj.331.7528.1292-d. PMC 1298891.
- Komarnitsky. "Case study of ultraviolet vision after IOL removal for Cataract Surgery". Archived from the original on 9 February 2014. Retrieved 17 January 2014.
- Griswold MS, Stark WS (September 1992). "Scotopic spectral sensitivity of phakic and aphakic observers extending into the near ultraviolet". Vision Research. 32 (9): 1739–1743. doi:10.1016/0042-6989(92)90166-G. PMID 1455745. S2CID 45178405.
- "Ultraviolet keratitis". Medscape. Archived from the original on 1 November 2015. Retrieved 31 May 2017.
- Mironava T, Hadjiargyrou M, Simon M, Rafailovich MH (20 July 2012). "The effects of UV emission from compact fluorescent light exposure on human dermal fibroblasts and keratinocytes in vitro". Photochemistry and Photobiology. 88 (6): 1497–1506. doi:10.1111/j.1751-1097.2012.01192.x. PMID 22724459. S2CID 2626216.
- Nicole W (October 2012). "Ultraviolet Leaks from CFLs". Environmental Health Perspectives. 120 (10): a387. doi:10.1289/ehp.120-a387. PMC 3491932. PMID 23026199.
- Michaelson S, ed. (2012). Fundamental and Applied Aspects of Nonionizing Radiation. Springer Science & Business Media. p. xv. ISBN 978-1468407600. Archived from the original on 14 December 2019. Retrieved 30 January 2019.
Further reading
- U.S. Congress, Office of Technology Assessment (May 1989). Biological Effects of Power Frequency Electric & Magnetic Fields—Background Paper, OTA-BP-E-53 (PDF). Washington, DC: U.S. Government Printing Office. Archived (PDF) from the original on 1 August 2014. Retrieved 2 May 2010. (over 100 pages)ju
External links
- Information page on electromagnetic fields at the World Health Organization web site
- CDC – Electric and Magnetic Fields – NIOSH Workplace Safety and Health Topic
- Dunning, Brian (30 October 2007). "Skeptoid #72: Electromagnetic Hypersensitivity: Real or Imagined?". Skeptoid.