Foster Kennedy syndrome
Foster Kennedy syndrome is a constellation of findings associated with tumors of the frontal lobe.[1]
| Foster Kennedy syndrome | |
|---|---|
| Other names | Gowers–Paton–Kennedy syndrome, Kennedy's phenomenon, Kennedy's syndrome |
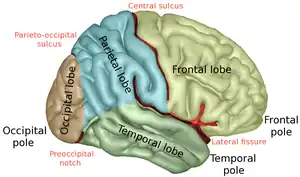 | |
| Frontal lobe (on the right) | |
| Specialty | Neurology |
Although Foster Kennedy syndrome is sometimes called "Kennedy syndrome",[2] it should not be confused with Kennedy disease, or spinal and bulbar muscular atrophy, which is named after William R. Kennedy.
Pseudo-Foster Kennedy syndrome is defined as one-sided optic atrophy with papilledema in the other eye but with the absence of a mass.[3]
Presentation
The syndrome is defined as the following changes:[4]
- optic atrophy in the ipsilateral eye
- disc edema in the contralateral eye
- central scotoma (loss of vision in the middle of the visual fields) in the ipsilateral eye
The presence of anosmia (loss of smell) ipsilateral to the eye demonstrating optic atrophy was historically associated with this syndrome, but is now understood to not strictly be associated with all cases.[4]
This syndrome is due to optic nerve compression, olfactory nerve compression, and increased intracranial pressure (ICP) secondary to a mass (such as meningioma or plasmacytoma, usually an olfactory groove meningioma).[5][6] There are other symptoms present in some cases such as nausea and vomiting, memory loss and emotional lability (i.e., frontal lobe signs).[6]
Diagnosis
Brain tumor can be visualized very well on CT scan, but MRI gives better detail and is the preferred study. Clinical localization of brain tumors may be possible by virtue of specific neurologic deficits or symptom patterns. Tumor at the base of the frontal lobe produces inappropriate behavior, optic nerve atrophy on the side of the tumor, and papilledema of the contralateral eye; anosmia on the side of the tumor may be found in certain cases of progressive disease. [4]
Treatment
The treatment, and therefore prognosis, varies depending upon the underlying tumour.[6] While awaiting surgical removal, treat any increased intracranial pressure with high-dose steroids (i.e., dexamethasone).
History
The syndrome was first extensively noted by Robert Foster Kennedy in 1911, an Irish neurologist, who spent most of his career working in the United States of America.[7] However, the first mention of the syndrome came from a William Gowers in 1893. Schultz–Zehden described the symptoms again in 1905. A later description was written by Wilhelm Uhthoff in 1915.[8]
References
- "Kennedy syndrome" at Dorland's Medical Dictionary
- "Foster Kennedy syndrome" at Dorland's Medical Dictionary
- Bansal S, Dabbs T, Long V (2008). "Pseudo-Foster–Kennedy Syndrome due to unilateral optic nerve hypoplasia: a case report". J Med Case Rep. 2: 86. doi:10.1186/1752-1947-2-86. PMC 2278154. PMID 18348732.
- Lai AT, Chiu SL, Lin IC, Sanders M (2014). "Foster Kennedy Syndrome: Now and The". Journal of Neuro-Opthanmology. 34 (1): 92–94. doi:10.1097/WNO.0000000000000072. PMID 24284554.
- Longmore, Murray; Ian Wilkinson; Tom Turmezei; Chee Kay Cheung (2007). Oxford Handbook of Clinical Medicine (7th ed.). Oxford University Press. p. 690. ISBN 978-0-19-856837-7.
- Willacy, Hayley. "Foster Kennedy syndrome". Retrieved 2008-08-13.
- Thorofare, NJ (1911). Kennedy F; Retrobulbar neuritis as an exact diagnostic sign of certain tumors and abscesses in the frontal lobe. American Journal of the Medical Sciences.
- "Kennedy's syndrome". Retrieved 2008-08-13.