Dracunculus medinensis
Dracunculus medinensis (Guinea worm, dragon worm, fiery serpent[1]) is a nematode that causes dracunculiasis, also known as guinea worm disease.[2] The disease is caused by the female[3] which, at around 80 centimetres (31 inches) in length,[4] is among the longest nematodes infecting humans.[5] In contrast, the longest recorded male Guinea worm is only 4 cm (1+1⁄2 in).[4]
| Guinea worm | |
|---|---|
 | |
| Photomicrograph of larvae | |
| Scientific classification | |
| Domain: | Eukaryota |
| Kingdom: | Animalia |
| Phylum: | Nematoda |
| Class: | Secernentea |
| Order: | Camallanida |
| Family: | Dracunculidae |
| Genus: | Dracunculus |
| Species: | D. medinensis |
| Binomial name | |
| Dracunculus medinensis | |
| Synonyms | |
Guinea worm is on target to be the second infectious disease of humans to be eradicated, after smallpox. It was formerly endemic to a wide swath of Africa and Eurasia; as of 2023, it remains endemic in 5 countries: Chad, Mali, South Sudan, Angola and Ethiopia,[6] with most cases in Chad. Guinea worm spread to Angola c. 2018, and it is now considered endemic there. Infection of domestic dogs is a serious complication in Chad.
The common name "guinea worm" is derived from the Guinea region of Western Africa.
History
Dracunculus medinensis ("little dragon from Medina") was described in Egypt as early as the 15th century BCE and possibly was the "fiery serpent" afflicting the Israelites described in the Bible.[7]
In the mid-19th century, the nematode Camallanus lacustris, which infects freshwater fish, was discovered to develop in copepods. This led Russian naturalist Alexei Pavlovich Fedchenko to discover in 1870 that D. medinensis is similarly transmitted via copepod intermediate hosts.[8]
Life cycle
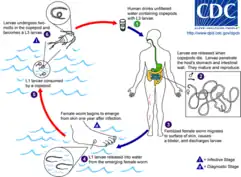
D. medinensis L1 larvae are found in fresh water, where they are ingested by copepods (small crustaceans) of the genus Cyclops. Within the copepod, the D. medinensis larvae develop to an infective L3 stage within 14 days.[9] When the infected copepod is ingested by a mammalian host drinking unfiltered water, the copepod is then dissolved by stomach acid and dies and the D. medinensis larvae are released and migrate through the wall of the mammalian intestine, and enter the abdominal cavity and retro-peritoneal space, where they mature into adults. After maturing and mating within the host, the males die and females (length 70–120 cm) migrate in subcutaneous tissue towards the skin's surface. Around a year after the infection, the female causes the formation of a blister on the skin's surface, generally on the lower extremities, though occasionally on the hand or scrotum. When the blister ruptures, the female slowly emerges over the course of several days or weeks.[9] This causes extreme pain and irritation to the host. During those few days to hours before the worm exits the skin, the person may develop a fever, pain, or swelling in that area. When the host — in an attempt to alleviate the excruciating burning pain — submerges the affected body part in water, the female releases thousands of larvae into the water. From here, the larvae infect copepods, continuing the life cycle.[9] After the worm exits the skin the wound caused by the emerging worm often develops a secondary bacterial infection. Permanent damage can occur if the infection goes untreated around a joint. Most cases occur in areas without access to health care facilities.[10]
Animal reservoirs
In 2020, Guinea worm was found in 1507 domestic dogs in Chad, 15 in Ethiopia, and eight in Mali, as well as in 61 domestic cats in Chad and three in Ethiopia. Small numbers have also been found in wildcats and baboons.[11] These findings are a potential problem for the eradication program.
Epidemiology
D. medinensis is most commonly found in the subtropic to tropical regions, especially in India, south-west Asia (Iraq, Iran, Pakistan, etc.), and rural areas of Africa, where temperatures between 25 and 30 °C are best for larval development.[12] The parasite relies on people accidentally consuming microcrustaceans of the genus Cyclops (copepods), that dwell in stationary bodies of water such as ponds, large, open wells (with stairs), or rain-filled cisterns.[12] The infection occurs most during times of drought or the "dry-season" in humid climates, or during or just after the rain season in the "semiarid, wet-and-dry-climates".[12] This is due to the lower surface water of the stationary bodies of water, which are prime for the growth of the infected copepods, and main source of water for many.[12]
Pathology
D. medinensis causes dracunculiasis as a result of the emergence of the female worm, nonemergence of adult worms (usually the male), and secondary bacterial infections.[13] As it emerges to the subcutaneous tissue, the female releases a toxic chemical that may result in nausea, rash at site, diarrhea, dizziness, localized edema, reddish papule, blister, and itching.[13] Arthritis or paraplegia can result from a worm that fails to reach the skin and gets calcified in or along the joint or finds its way into the central nervous tissue.[13] Aseptic abscesses and cystic swelling can also occur when worms rupture before emerging, causing an acute inflammatory response from the host's immune system.[13]
Treatment
The female guinea worm slowly starts to emerge from the host's skin after the blister ruptures. The most common method for removing the worm involves submerging the affected body part in water to help coax the worm out. The site is then cleaned thoroughly. Then, slight pressure is applied to the worm as it is slowly pulled out of the wound. To avoid breaking the worm, pulling should stop when resistance is met. Full extraction of the female guinea worm usually takes several days. After each day's worth of extraction, the exposed portion of the worm is wrapped around a piece of rolled-up gauze or small stick to maintain tension.[14] This method of wrapping the worm around a stick or gauze is speculated to be the source for the Rod of Asclepius, the symbol of medicine.[15] Once secure, topical antibiotics are applied to the affected region, to help prevent secondary infections due to bacteria, which is then wrapped in gauze to protect the wound. The same steps are repeated each day until the whole worm has been removed from the lesion.[14]
Eradication program
| Year | Reported cases | Countries |
|---|---|---|
| 1986 | estimated 3,500,000 | 21[17] |
| 1989 | 892,055 | 15[18] |
| 1992 | 374,202 | 15[18] |
| 1995 | 129,852 | 19[18] |
| 2000 | 75,223 | 16[18] |
| 2001 | 63,717 | 16[18] |
| 2002 | 54,638 | 14[18] |
| 2003 | 32,193 | 13[18] |
| 2004 | 16,026 | 13[18] |
| 2005 | 10,674 | 12[18] |
| 2006 | 25,217 [lower-alpha 1] | 10 [18] |
| 2007 | 9,585 | 9[18] |
| 2008 | 4,619 | 7[18] |
| 2009 | 3,190 | 5 |
| 2010 | 1,797 | 4[20] (6[21]) |
| 2011 | 1,060 | 4[22] |
| 2012 | 542 | 4[23] |
| 2013 | 148 | 5[24] |
| 2014 | 126 | 4[25] |
| 2015 | 22 | 4[26] |
| 2016 | 25 | 3[17] |
| 2017 | 30 | 2[27] |
| 2018 | 28 | 3[28] |
| 2019 | 54 [lower-alpha 2] | 4[29] |
| 2020 | 27 | 6[30] |
| 2021 | 15 | 4[31] |
| 2022 | 13 | 4[32] |
In the 1980s, the Carter Center initiated a program to eradicate the guinea worm.[33] The campaign began in 1980 at the U.S. Centers for Disease Control and Prevention. In 1984, the CDC was designated by the World Health Organization as the "Collaborating Center for Research, Training, and Eradication of D. medinensis". More than twenty countries were affected by Guinea worms in 1986. That year, WHO started the eradication program with the Carter Center leading the effort.[34] The program included education of people in affected areas that the disease was caused by larvae in drinking water, isolation and support for affected people, and – crucially – widespread distribution of net filters and pipe filters for drinking water, and education about the importance of using them.
As of 2015, the species has been reported to be near eradication.[33] The International Commission for the Certification of Dracunculus Eradication has certified 198 countries, territories, and other WHO represented areas. As of January 2015, eight countries were yet to be certified as Guinea worm-free: Angola, the Democratic Republic of the Congo, Kenya, Sudan, Chad, Ethiopia, Mali, and South Sudan; of these, only in Chad, Ethiopia, Mali, and South Sudan does D. medinensis remain endemic countries.[34]
See also
Explanatory notes
References
- Chaudhury, Abhijit (2022). "Dracunculiasis". Textbook of Parasitic Zoonoses. Microbial Zoonoses. pp. 427–436. doi:10.1007/978-981-16-7204-0_41. ISBN 978-981-16-7203-3.
- Knopp, Stefanie; Amegbo, Ignace K.; Hamm, David M.; Schulz-Key, Hartwig; Banla, Meba; Soboslay, Peter T. (March 2008). "Antibody and cytokine responses in Dracunculus medinensis patients at distinct states of infection". Transactions of the Royal Society of Tropical Medicine and Hygiene. 102 (3): 277–283. doi:10.1016/j.trstmh.2007.12.003. PMID 18258273.
- Bimi, Langbong (2007). "Potential vector species of Guinea worm (Dracunculus medinensis) in northern Ghana". Vector-Borne and Zoonotic Diseases. 7 (3): 324–329. doi:10.1089/vbz.2006.0622. PMID 17767406.
- Schmidt, G.D.; Roberts, L.S. (2009). Roberts, Larry S.; Janovy, John, Jr. (eds.). Foundations of Parasitology (8th ed.). McGraw-Hill. pp. 480–484. ISBN 978-0-07-128458-5.
{{cite book}}: CS1 maint: multiple names: editors list (link) - bin Saleem, Talha; Ahmed, Irfan (2006). ""Serpent" in the breast" (PDF). Journal of Ayub Medical College Abbottabad. 18 (4): 67–68. PMID 17591014.
- Control of Neglected Tropical Diseases WHO Team (2023). Criteria for the certification of dracunculiasis eradication 2023 update. World Health Organization (WHO). pp. 9, 26. ISBN 978-92-4-007334-0.



This work is licensed under the Creative Commons Attribution-ShareAlike 3.0 License. - "Dracunculiasis: Historical background". who.int. World Health Organization. Archived from the original on 18 October 2014. Retrieved 27 April 2017.
- Anderson, Roy C. (8 February 2000). Nematode Parasites of Vertebrates: Their development and transmission. CABI. p. 1. ISBN 978-0-85199-786-5 – via Google Books.
- "Dracunculiasis: About Guinea-Worm Disease". who.int. World Health Organization. Archived from the original on 1 November 2006. Retrieved 20 December 2015.
- "General information – frequently asked questions (FAQs)". Guinea Worm Disease. U.S. Centers for Disease Control and Prevention (CDC). 17 September 2020. Retrieved 24 October 2020.
- "Guinea worm cases fell 50% in 2020, Carter Center reports". cartercenter.org (Press release). The Carter Center. 26 January 2021.
- Muller, R. (1979). "Guinea worm disease: Epidemiology, control, and treatment". Bulletin of the World Health Organization. 57 (5): 683–689. PMC 2395878. PMID 161522.
- Roberts, Larry S.; Janovy, John, Jr.; Nadler, Steve (27 November 2012). Gerald D. Schmidt & Larry S. Roberts' foundations of parasitology (9th ed.). New York, NY. ISBN 9780073524191. OCLC 812614125.
{{cite book}}: CS1 maint: location missing publisher (link) CS1 maint: multiple names: authors list (link) - "Management of Guinea worm disease (GWD)". Parasites – Guinea Worm. cdc.gov. U.S. Centers for Disease Control (CDC). 16 March 2018. Retrieved 22 July 2018.
- Satin, Morton (2009). Death in the Pot: The impact of food poisoning on history. Amherst, NY: Prometheus Books. pp. 63–65. ISBN 978-1-61-592224-6 – via Google Books.
- "Guinea worm case totals". cartercenter.org. The Carter Center.
- Martin, Jeff (11 January 2017). "Carter: Guinea worm disease reported in 3 countries in 2016". Associated Press. Retrieved 11 January 2017.
-
Dracunculiasis Epidemiological Data (1989-2008) (PDF). who.int (Report). World Health Organization. Retrieved 14 September 2009. - Centers for Disease Control and Prevention (CDC) (17 August 2007). "Progress toward global eradication of Dracunculiasis, January 2005 – May 2007". Morbidity and Mortality Weekly Report. U.S. Centers for Disease Control and Prevention (CDC). 56 (32): 813–817. PMID 17703170. Retrieved 16 March 2011.
- "Guinea worm countdown: The road to eradication". cartercenter.org. The Carter Center. Archived from the original on 6 September 2011. Retrieved 22 July 2018.
- "Monthly report on dracunculiasis cases, January–December 2010" (PDF). Weekly Epidemiological Record. WHO. 86 (10): 92. 4 March 2011. Retrieved 4 March 2011.
- "Wrap-up #209" (PDF). Guinea Worm Wrap-up. WHO Collaborating Center for Research, Training and Eradication of Dracunculiasis. No. 209. World Health Organization (WHO). 9 January 2012 – via The Carter Center (cartercenter.org).
- "Wrap-up #218" (PDF). Guinea Worm Wrap-up. WHO Collaborating Center for Research, Training and Eradication of Dracunculiasis. No. 218. World Health Organization (WHO). 22 April 2013. Retrieved 4 November 2022 – via The Carter Center (cartercenter.org).
- "Wrap-up #226" (PDF). Guinea Worm Wrap-up. WHO Collaborating Center for Research, Training and Eradication of Dracunculiasis. No. 226. World Health Organization (WHO). 9 May 2014. Retrieved 4 November 2022 – via The Carter Center (cartercenter.org).
- "126 Cases of Guinea worm disease remain worldwide". cartercenter.org (Press release). The Carter Center. 11 January 2015. Retrieved 9 May 2015.
- "Wrap-up #240" (PDF). Guinea Worm Wrap-up. WHO Collaborating Center for Research, Training and Eradication of Dracunculiasis. No. 240. World Health Organization (WHO). 13 May 2016. Retrieved 4 November 2022 – via The Carter Center (cartercenter.org).
- "Announcement for 2017 Guinea worm disease case totals". cartercenter.org (Press release). The Carter Center. 19 January 2018. Archived from the original on 20 January 2018. Retrieved 22 July 2018.
- "28 Guinea worm cases reported in 2018". cartercenter.org (Press release). Guinea worm update. The Carter Center. 6 May 2019.
- "54* cases of Guinea worm reported in 2019". cartercenter.org (Press release). The Carter Center. January 2020.
- "Guinea worm cases fell 50% in 2020, Carter Center reports". cartercenter.org (Press release). The Carter Center. 2021.
- "Wrap-up #286" (PDF). Guinea Worm Wrap-up. WHO Collaborating Center for Research, Training and Eradication of Dracunculiasis. No. 286. World Health Organization (WHO). 31 March 2022. Retrieved 29 January 2023 – via The Carter Center (cartercenter.org).
- "Guinea worm disease reaches all-time low: Only 13* human cases reported in 2022". The Carter Center. 24 January 2023. Retrieved 29 January 2023.
- "This species is close to extinction, and that's a good thing". Time. World Science Festival. 23 January 2015.
- "Eradication program". Parasites – Guinea worm. U.S. Centers for Disease Control and Prevention. 2 May 2017. Retrieved 22 July 2018.
External links
- "Donors commit $240 million to fight neglected diseases". Voice of America. 2 April 2014. Archived from the original on 4 April 2014. Retrieved 4 April 2014 – via HNKC News.
- Bestall, Clifford (Spring 2014). How to Slay a Dragon (video documentary). Lifelines: The quest for global health. Al Jazeera English.
47 min.