Heavy menstrual bleeding
Heavy menstrual bleeding (HMB), previously known as menorrhagia or hypermenorrhea, is a menstrual period with excessively heavy flow. It is a type of abnormal uterine bleeding (AUB).[1][2]
| Heavy menstrual bleeding | |
|---|---|
| Other names | Hypermenorrhea, menorrhagia |
| Specialty | Gynecology |
| Symptoms | bleeding more than usual |
| Complications | Anemia, severe pain |
| Risk factors | family history, anovulation, fibroids, polyps, and adenomyosis |
| Diagnostic method | based on physical examination |
| Differential diagnosis | Irregular menstruation |
| Medication | tranexamic acid |
Abnormal uterine bleeding can be caused by structural abnormalities in the reproductive tract, anovulation, bleeding disorders, hormonal issues (such as hypothyroidism) or cancer of the reproductive tract. Initial evaluation aims at determining pregnancy status, menopausal status, and the source of bleeding. One definition is bleeding lasting more than 7 days or the loss of more than 80 mL of blood heavy flow.[3]
Treatment depends on the cause, severity, and interference with quality of life.[4] Initial treatment often involve birth control pills. Tranexamic acid, danazol, progesterone IUDs, and NSAIDs are also helpful.[5] Surgery can be an effective for those whose symptoms are not well-controlled with other treatments.[6] Approximately 53 in 1000 women are affected by AUB.[7]
Signs and symptoms
A normal menstrual cycle is 21–35 days in duration, with bleeding lasting an average of 5 days and total blood flow between 25 and 80 mL. Heavy menstrual bleeding is defined as total menstrual flow >80ml per cycle, soaking a pad/tampon at least every 2 hours, changing a pad/tampon in the middle of the night, or bleeding lasting for >7 days.[3][1][8] Deviations in terms of frequency of menses, duration of menses, or volume of menses qualifies as abnormal uterine bleeding. Bleeding in between menses, outside reproductive age, or after sex is also abnormal uterine bleeding and thus requires further evaluation.[9]
Causes
Usually, no causative abnormality can be identified and treatment is directed at the symptom, rather than a specific mechanism. However, there are known causes of abnormal uterine bleeding that need to be ruled out. Most common causes based on the nature of bleeding is listed below followed by the rare causes of bleeding (i.e. disorders of coagulation).
- Excessive menses but normal cycle:
- Painless:
- Fibroids (leiomyoma) — fibroids in the wall of the uterus cause increased menstrual loss if they protrude into the central cavity and thereby increase endometrial surface area.
- Coagulation defects (rare) — with the shedding of an endometrial lining's blood vessels, normal coagulation process must occur to limit and eventually stop the blood flow. Blood disorders of platelets (such as ITP) or coagulation (such as von Willebrand disease) or use of anticoagulant medication (such as warfarin) are therefore possible causes, although a rare minority of cases. Platelet function studies can also be used to ascertain platelet function abnormalities
- Endometrial cancer (cancer of the uterine lining) — bleeding can also be irregular, in between periods, or after the menopause (post-menopausal bleeding or PMB)
- Endometrial polyp
- Painful (i.e. associated with dysmenorrhea):
- Pelvic inflammatory disease
- Adenomyosis - extension of the endometrial tissue into the outer muscular wall of the uterus which can cause pain and abnormal bleeds when the endometrium sheds
- Pregnancy related complication (i.e. miscarriage)
- Painless:
- Short cycle (less than 21 days) but normal menses.
- Short cycle and excessive menses due to ovarian dysfunction and may be secondary to blockage of blood vessels by tumours.
- Polycystic ovary syndrome.[3]
- Systemic causes: thyroid disease, excessive emotional/physical stress.[3]
- Sexually transmitted infection.[3]
Pathophysiology
HMB is associated with increased omega-6 AA in uterine tissues.[10] The endometrium of women with HMB have higher levels of prostaglandin (E2, F2alpha and others) when compared with women with normal menses.[5] It is thought that prostaglandins are a by product of omega 6 build up.[11] Furthermore, prostaglandins have been found to trigger abnormal, painful uterine contractions, making it a source for targeted therapy.[12]
Diagnosis
The NICE guidelines states that: "Many women presenting to primary care with symptoms of HMB can be offered treatment without the need for further examination or investigation. However, investigation via a diagnostic technique might be warranted for women for whom history or examination suggests a structural or endometrial pathology or for whom the initial treatment has failed."[13]
Diagnosis is largely achieved by obtaining a complete medical history followed by physical exam and vaginal ultrasonography. If need be, laboratory tests or hysteroscopy may be used. The following are a list of diagnostic procedures that medical professionals may use to identify the cause of the abnormal uterine bleeding.
- Pelvic and rectal examination to ensure that bleeding is not from lower reproductive tract (i.e. vagina, cervix) or rectum
- Pap smear to rule out cervical neoplasia
- Pelvic ultrasound scan is the first line diagnostic tool for identifying structural abnormalities.[14]
- Endometrial biopsy in women with high risk endometrial cancer or atypical hyperplasia or malignancy.[13]
- Sonohysterography to assess for abnormalities within the uterine lining[15]
- Hysteroscopy (anaesthesia should be offered)[13]
- Thyroid-stimulating hormone and thyrotropin-releasing hormone dosage to rule out hypothyroidism [16]
Treatment
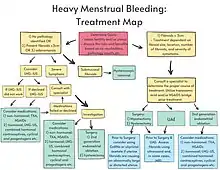
Treatment depends on identified underlying cause and varies between medication, radiation, and surgery. Heavy periods at menarche and menopause may settle spontaneously (the menarche being the start and menopause being the cessation of periods).
If the degree of bleeding is mild, all that may be sought by the woman is the reassurance that there is no sinister underlying cause. If anemia occurs due to bleeding then iron tablets may be used to help restore normal hemoglobin levels.[1]
The first line treatment option for women with HMB and no identified pathology, fibroids less than 3 cm in diameter, and/or suspected or confirmed adenomyosis is the levonorgestrel-releasing intrauterine system (LNG-IUS).[13] Clinical trial evidence suggests that the LNG-IUS may be better than other medical therapy in terms of HMB and quality of life.[18]
Usually, oral combined contraceptive or progesterone only pills may be taken for a few months, but for longer-term treatment the alternatives of injected Depo Provera or the more recent progesterone releasing IntraUterine System (IUS) may be used. In particular, an oral contraceptive containing estradiol valerate and dienogest may be more effective than tranexamic acid, NSAIDs and IUDs.[19][20] Fibroids may respond to hormonal treatment, and if they do not, then radiation or surgical removal may be required. Regarding hormonal treatment, the NICE guidelines states that: "No evidence was found on MRI-guided transcutaneous focused ultrasound for uterine fibroids nor for the progestogen-only pill, injectable progestogens, or progestogen implants."[13] Progestogen pills, independently if taken in a short or long course, are not as effective at reducing menstrual blood loss as LNG-IUS or tranexamic acid.[21]
NICE guidelines says that for individuals with HMB and no identified pathology or fibroids less than 3 cm in diameter who do not wish to have pharmacological treatment and who do not want to conserve their fertility, surgical options could be considered as a first-line treatment option. Options include a hysterectomy and second generation endometrial ablation, with hysterectomy being more effective than second generation endometrial ablation.[13]
Tranexamic acid treatments, which reduce bleeding by inhibiting the clot-dissolving enzymes, appear to be more effective than anti-inflammatory treatment like NSAIDs, but are less effective than LNG-IUS.[22] Tranexamic acid tablets may reduce loss by up to 50%.[23] This may be combined with hormonal medication previously mentioned.[24]
NSAIDs are also used to reduce heavy menstrual bleeding by an average of 20-46% through inhibiting the production of prostaglandins.[5] For this purpose, NSAIDs are ingested for only 5 days of the menstrual cycle, limiting their most common adverse effect of dyspepsia.[25]
A definitive treatment for heavy menstrual bleeding is to perform hysterectomy (removal of the uterus). The risks of the procedure have been reduced with measures to minimize the risk of deep vein thrombosis after surgery, and the switch from the front abdominal to vaginal approach greatly minimizing the discomfort and recuperation time for the patient; however extensive fibroids may make the womb too large for removal by the vaginal approach. Small fibroids may be dealt with by local removal (myomectomy). A further surgical technique is endometrial ablation (destruction) by the use of applied heat (thermoablation).[26] The effectiveness of endometrial ablation is probably similar to that of LNG‐IUS but the evidence is uncertain if hysterectomy is better or worse than LNG-IUS for improving HMB.[18]
Medications
These have been ranked by the UK's National Institute for Health and Clinical Excellence:[14]
- First line
- Second Line
- Tranexamic acid an antifibrinolytic agent
- Nonsteroidal anti-inflammatory drugs (NSAIDs).
- Combined oral contraceptive pills to prevent proliferation of the endometrium
- Third line
- Oral progestogen (e.g. norethisterone), to prevent proliferation of the endometrium
- Injected progestogen (e.g. Depo provera)
- Other options
Surgery
- Dilation and curettage (D&C) is not recommended for cases of simple heavy menstrual bleeding, having a reserved role if a spontaneous abortion is incomplete[27]
- Endometrial ablation is not recommended for women with active or recent genital or pelvic infection, known or suspected endometrial hyperplasia or malignancy.[28]
- Uterine artery embolization (UAE) is a common treatment with the etiology of a leiomyoma. The rate of serious complications is comparable to that of myomectomy or hysterectomy; however, UAE presents an increased risk of minor complications and requiring surgery within two to five years.[29][30]
- Hysteroscopic myomectomy is a minimally invasive surgical procedure to remove leiomyomas (otherwise known as fibroids). Though a safe and effective mode of treating for menstrual disorders but it is unclear whether or not it is beneficial for treating infertility.[31]
- Hysterectomy is a surgical procedure consisting of the full removal of the uterus, and can include the removal of fallopian tubes (otherwise known as the uterine tubes), cervix and ovaries.[32]
In the UK the use of hysterectomy for heavy menstrual bleeding has been almost halved between 1989 and 2003.[33] This has a number of causes: better medical management, endometrial ablation and particularly the introduction of IUS[34][35] which may be inserted in the community and avoid the need for specialist referral; in one study up to 64% of women cancelled surgery.[36]
Complications
Previous studies have suggested a nontrivial reduction in the quality of life in individuals with HMB; however, there is no single metric that has been shown to be specific enough to measure health-related quality of life in individuals with HMB.[37] Evidence suggests that HMB can take a significant toll on the physical, psychological, and social aspects of individuals' lives. For example, a large, cross-sectional study in the United States identified significant associations between HMB and lower employment rates, lost earnings, and a lower self-rating of overall health compared to the general population.[38] Physical and social issues, including performance of house work, life causing embarrassment, and social life, have also been identified as significant reasons why individuals with HMB seek help.[39] While the main impacts of HMB are primarily physical and social, previous studies have also identified an inverse relationship between HMB and psychological scores.[40]
Aside from the social distress of dealing with a prolonged and heavy period, over time the blood loss may prove to be greater than the body iron reserves or the rate of blood replenishment, leading to anemia.[4] Symptoms attributable to the anemia may include shortness of breath, tiredness, weakness, tingling and numbness in fingers and toes, headaches, depression, becoming cold more easily, and poor concentration.
References
- Munro MG, Critchley HO, Broder MS, Fraser IS (April 2011). "FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age". International Journal of Gynaecology and Obstetrics. 113 (1): 3–13. doi:10.1016/j.ijgo.2010.11.011. PMID 21345435. S2CID 205260568.
- Bacon JL (June 2017). "Abnormal Uterine Bleeding: Current Classification and Clinical Management". Obstetrics and Gynecology Clinics of North America. 44 (2): 179–193. doi:10.1016/j.ogc.2017.02.012. PMID 28499529.
- O'Brien SH (2018). "Evaluation and management of heavy menstrual bleeding in adolescents: the role of the hematologist". Hematology. 30 (1): 390–398. doi:10.1182/asheducation-2018.1.390. PMC 6246024. PMID 30504337.
- Committee on Practice Bulletins—Gynecology (July 2013). "Practice bulletin no. 136: management of abnormal uterine bleeding associated with ovulatory dysfunction". Obstetrics and Gynecology. 122 (1): 176–85. doi:10.1097/01.AOG.0000431815.52679.bb. PMID 23787936. S2CID 2796244.
- Bofill Rodriguez, M; Lethaby, A; Farquhar, C (19 September 2019). "Non-steroidal anti-inflammatory drugs for heavy menstrual bleeding". The Cochrane Database of Systematic Reviews. 2019 (9): CD000400. doi:10.1002/14651858.CD000400.pub4. PMC 6751587. PMID 31535715.
- Marjoribanks J, Lethaby A, Farquhar C (January 2016). "Surgery versus medical therapy for heavy menstrual bleeding". The Cochrane Database of Systematic Reviews. 2016 (1): CD003855. doi:10.1002/14651858.CD003855.pub3. PMC 7104515. PMID 26820670.
- Kjerulff KH, Erickson BA, Langenberg PW (February 1996). "Chronic gynecological conditions reported by US women: findings from the National Health Interview Survey, 1984 to 1992". American Journal of Public Health. 86 (2): 195–9. doi:10.2105/ajph.86.2.195. PMC 1380327. PMID 8633735.
- "Menorrhagia (heavy menstrual bleeding) - Symptoms and causes". Mayo Clinic. Retrieved 2022-09-10.
- "Abnormal Uterine Bleeding". www.acog.org. Retrieved 2022-09-10.
- Joseph E. Pizzorno; Michael T. Murray; Herb Joiner-Bey (2015). The Clinician's Handbook of Natural Medicine. doi:10.1016/C2010-0-67298-1. ISBN 978-0-7020-5514-0.
- Harel Z (December 2006). "Dysmenorrhea in adolescents and young adults: etiology and management". Journal of Pediatric and Adolescent Gynecology. 19 (6): 363–71. doi:10.1016/j.jpag.2006.09.001. PMID 17174824.
- Smith, Roger P. (2018). Dysmenorrhea and Menorrhagia. doi:10.1007/978-3-319-71964-1. ISBN 978-3-319-71963-4. S2CID 10078385.
- Heavy menstrual bleeding (update). National Institute for Health and Care Excellence. 2018.
- "CG44 Heavy menstrual bleeding: Understanding NICE guidance" (PDF). National Institute for Health and Clinical Excellence (UK). 24 January 2007.
- "Menorrhagia (heavy menstrual bleeding) - Diagnosis and treatment - Mayo Clinic". www.mayoclinic.org. Retrieved 2022-09-10.
- Weeks AD (March 2000). "Menorrhagia and hypothyroidism. Evidence supports association between hypothyroidism and menorrhagia". BMJ. 320 (7235): 649. doi:10.1136/bmj.320.7235.649. PMC 1117669. PMID 10698899.
- "NICE Guideline - Renal and ureteric stones: assessment and management". BJU International. 123 (2): 220–232. 2019-01-17. doi:10.1111/bju.14654. ISSN 1464-4096. PMID 30656839.
- Bofill Rodriguez, M; Lethaby, A; Jordan, V (12 June 2020). "Progestogen-releasing intrauterine systems for heavy menstrual bleeding". The Cochrane Database of Systematic Reviews. 2020 (6): CD002126. doi:10.1002/14651858.CD002126.pub4. PMC 7388184. PMID 32529637.
- Kaunitz AM, Meredith S, Inki P, Kubba A, Sanchez-Ramos L (May 2009). "Levonorgestrel-releasing intrauterine system and endometrial ablation in heavy menstrual bleeding: a systematic review and meta-analysis". Obstetrics and Gynecology. 113 (5): 1104–16. doi:10.1097/AOG.0b013e3181a1d3ce. PMID 19384127. S2CID 25599471.
- Jensen JT, Parke S, Mellinger U, Machlitt A, Fraser IS (April 2011). "Effective treatment of heavy menstrual bleeding with estradiol valerate and dienogest: a randomized controlled trial". Obstetrics and Gynecology. 117 (4): 777–87. doi:10.1097/AOG.0b013e3182118ac3. PMID 21422847. S2CID 40164050.
- Bofill Rodriguez M, Lethaby A, Low C, Cameron IT (14 August 2019). "Cyclical progestogens for heavy menstrual bleeding". Cochrane Database Syst Rev. 8 (8): CD001016. doi:10.1002/14651858.CD001016.pub3. PMC 6699663. PMID 31425626.
- Bryant-Smith AC, Lethaby A, Farquhar C, Hickey M (15 April 2018). "Antifibrinolytics for heavy menstrual bleeding". Cochrane Database Syst Rev. 2018 (6): CD000249. doi:10.1002/14651858.CD000249.pub2. PMC 6494516. PMID 29656433.
- Bonnar J, Sheppard BL (September 1996). "Treatment of menorrhagia during menstruation: randomised controlled trial of ethamsylate, mefenamic acid, and tranexamic acid". BMJ. 313 (7057): 579–82. doi:10.1136/bmj.313.7057.579. PMC 2352023. PMID 8806245.
- Lukes AS, Moore KA, Muse KN, Gersten JK, Hecht BR, Edlund M, Richter HE, Eder SE, Attia GR, Patrick DL, Rubin A, Shangold GA (October 2010). "Tranexamic acid treatment for heavy menstrual bleeding: a randomized controlled trial". Obstetrics and Gynecology. 116 (4): 865–75. doi:10.1097/AOG.0b013e3181f20177. PMID 20859150. S2CID 6977827.
- A Shaw J (2014-09-29). "Menorrhagia Treatment & Management". Medscape. Retrieved 2015-01-04.
- Bofill Rodriguez, M; Lethaby, A; Grigore, M; Brown, J; Hickey, M; Farquhar, C (22 January 2019). "Endometrial resection and ablation techniques for heavy menstrual bleeding". The Cochrane Database of Systematic Reviews. 1 (1): CD001501. doi:10.1002/14651858.CD001501.pub5. PMC 7057272. PMID 30667064.
- Duckitt K (September 2015). "Menorrhagia". BMJ Clinical Evidence. 2015. PMC 4574688. PMID 26382038.
- Louie M, Wright K, Siedhoff MT (2018). "The case against endometrial ablation for treatment of heavy menstrual bleeding". Curr Opin Obstet Gynecol. 30 (4): 287–292. doi:10.1097/GCO.0000000000000463. PMID 29708902. S2CID 13671197.
- Gupta, Janesh K.; Sinha, Anju; Lumsden, M. A.; Hickey, Martha (2014-12-26). "Uterine artery embolization for symptomatic uterine fibroids". The Cochrane Database of Systematic Reviews (12): CD005073. doi:10.1002/14651858.CD005073.pub4. ISSN 1469-493X. PMID 25541260.
- Spies, James B; Ascher, Susan A; Roth, Antoinette R; Kim, Joon; Levy, Elliot B; Gomez-Jorge, Jackeline (2001-07-01). "Uterine artery embolization for leiomyomata". Obstetrics & Gynecology. 98 (1): 29–34. doi:10.1016/S0029-7844(01)01382-5. ISSN 0029-7844. PMID 11430952.
- Stewart, Elizabeth A (January 2001). "Uterine fibroids". The Lancet. 357 (9252): 293–298. doi:10.1016/s0140-6736(00)03622-9. ISSN 0140-6736. PMID 11214143. S2CID 12675635.
- Clayton, R.D. (February 2006). "Hysterectomy". Best Practice & Research Clinical Obstetrics & Gynaecology. 20 (1): 73–87. doi:10.1016/j.bpobgyn.2005.09.007. ISSN 1521-6934. PMID 16275095.
- Reid PC, Mukri F (April 2005). "Trends in number of hysterectomies performed in England for menorrhagia: examination of health episode statistics, 1989 to 2002-3". BMJ. 330 (7497): 938–9. doi:10.1136/bmj.38376.505382.AE. PMC 556338. PMID 15695496.
- Hurskainen R, Teperi J, Rissanen P, Aalto AM, Grenman S, Kivelä A, Kujansuu E, Vuorma S, Yliskoski M, Paavonen J (March 2004). "Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: randomized trial 5-year follow-up". JAMA. 291 (12): 1456–63. doi:10.1001/jama.291.12.1456. PMID 15039412.
- Istre O, Trolle B (August 2001). "Treatment of menorrhagia with the levonorgestrel intrauterine system versus endometrial resection". Fertility and Sterility. 76 (2): 304–9. doi:10.1016/S0015-0282(01)01909-4. PMID 11476777.
- Stewart A, Cummins C, Gold L, Jordan R, Phillips W (January 2001). "The effectiveness of the levonorgestrel-releasing intrauterine system in menorrhagia: a systematic review". BJOG. 108 (1): 74–86. doi:10.1016/S0306-5456(00)00020-6. PMID 11213008.
- Clark, T. Justin; Khan, Khalid S.; Foon, Richard; Pattison, Helen; Bryan, Stirling; Gupta, Janesh K. (2002-09-10). "Quality of life instruments in studies of menorrhagia: a systematic review". European Journal of Obstetrics, Gynecology, and Reproductive Biology. 104 (2): 96–104. doi:10.1016/s0301-2115(02)00076-3. ISSN 0301-2115. PMID 12206918.
- Côté, Isabelle; Jacobs, Philip; Cumming, David (October 2002). "Work loss associated with increased menstrual loss in the United States". Obstetrics and Gynecology. 100 (4): 683–687. doi:10.1016/s0029-7844(02)02094-x. ISSN 0029-7844. PMID 12383534. S2CID 22526668.
- Shapley, M.; Jordan, K.; Croft, P. R. (January 2003). "Increased vaginal bleeding: the reasons women give for consulting primary care". Journal of Obstetrics and Gynaecology: The Journal of the Institute of Obstetrics and Gynaecology. 23 (1): 48–50. doi:10.1080/0144361021000043245. ISSN 0144-3615. PMID 12623484. S2CID 22878317.
- Hurskainen, R.; Aalto, A. M.; Teperi, J.; Grenman, S.; Kivelä, A.; Kujansuu, E.; Vuorma, S.; Yliskoski, M.; Paavonen, J. (March 2001). "Psychosocial and other characteristics of women complaining of menorrhagia, with and without actual increased menstrual blood loss". BJOG: An International Journal of Obstetrics and Gynaecology. 108 (3): 281–285. doi:10.1111/j.1471-0528.2001.00040.x. ISSN 1470-0328. PMID 11281469. S2CID 750120.