Hemipelvectomy
Hemipelvectomy, also known as a pelvic resection, is a surgical procedure that involves the removal of part of the pelvic girdle. This procedure is most commonly performed to treat oncologic conditions of the pelvis.[1][2] Hemipelvectomy can be further classified as internal and external hemipelvectomy.[1][2] An internal hemipelvectomy is a limb-sparing procedure where the innominate bone is resected while preserving the ipsilateral limb.[1][2] An external hemipelvectomy involves the resection of the innominate bone plus amputation of the ipsilateral limb.[1][2]
| Hemipelvectomy | |
|---|---|
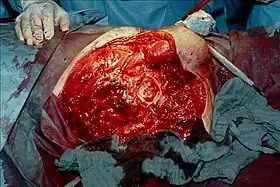 Intraoperative photograph after hemipelvectomy on the right side with view of the acetabulum. This was done for a case of gas gangrene. | |
| Other names | Hindquarter amputation, pelvic resection |
| Specialty | Orthopedic surgery |
Medical uses
Hemipelvectomy is generally reserved for the treatment of pelvic neoplasms.[1][2] Examples of malignancies that are treated with hemipelvectomy include osteosarcoma, chondrosarcoma, and Ewing's sarcoma.[1] Rarely, hemipelvectomy is performed in settings of traumatic injury and osteomyelitis.[1] Indications for external hemipelvectomy include neoplastic extension into the sciatic nerve, where loss of function of the lower extremity is anticipated.[1] Internal hemipelvectomy is preferred when complete resection of the tumor is possible without sacrificing the lower extremity.[1] If external hemipelvectomy cannot provide a greater degree of tumor resection compared to internal hemipelvectomy, internal hemipelvectomy is recommended.[1] Internal hemipelvectomy must only be considered when the surgical approach can ensure the preservation of critical neurovascular structures in the region.[1]
Complications
As with any surgical procedure, risks include infection, blood loss, damage to surrounding structures, cardiac/pulmonary complications, and adverse reactions to anesthesia.
Complications of external hemipelvectomy include:[1][2]
- Disfigurement
- Loss of ambulation
- Phantom limb pain
- Bladder dysfunction
- Sexual dysfunction
- Bowel dysfunction
Complications of internal hemipelvectomy include:[1][2]
- Leg-length discrepancy
- 'Flail hip' or 'floating hip' (referring to hypermobility of the hip joint)
- Hip instability
Technique
Prior to performing a hemipelvectomy, surgeons must possess detailed knowledge of the pelvic anatomy and its relation to the pelvic tumor.[1] Imaging studies such as conventional radiography, computed tomography, and magnetic resonance imaging help the surgeon visualize the anatomy and its relationship to the local pathology.[1] Surgical oncology techniques are utilized when resecting tumors of the pelvis.[1] Such techniques ensure that adequate resection margins are obtained at the time of surgery to minimize tumor recurrence.[1]
The Enneking and Dunham classification system was developed in 1978 to aid surgeons in characterizing pelvic resections.[1][3][4] This classification scheme breaks down pelvic resections into 3 subtypes: Type I, Type II, and Type III.[1][3][4] Type I resections involve removal of the ilium.[1][3][4] Type II resections involve removal of the peri-acetabular region.[1][3][4] Type III resections involve removal of the ischial and/or pubic region.[1][3]
Resection of pelvic bone typically requires subsequent reconstruction to ensure stability of the hip joint, particularly in internal hemipelvectomy.[1] Examples of pelvic reconstruction include the use of an allograft, autograft, or prosthesis to bridge the remaining ends of pelvic bone following resection.[1][4] Arthrodesis is a technique that can be used in internal hemipelvectomy to fix the proximal femur to a segment of pelvic bone for the purposes of stabilizing the lower extremity.[1][4]
Additional images
 An x-ray of a limb-sparing hemipelvectomy on the left side of a male pelvis taken one month after surgery.
An x-ray of a limb-sparing hemipelvectomy on the left side of a male pelvis taken one month after surgery.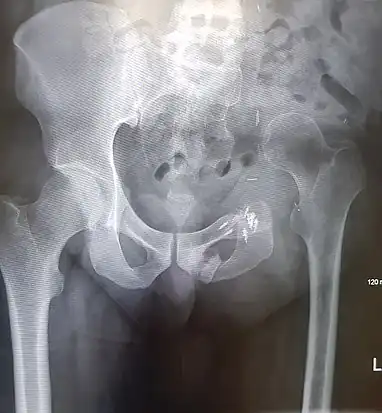 An x-ray of the same pelvis taken eighteen months after surgery highlighting the femur migration to its final resting place.
An x-ray of the same pelvis taken eighteen months after surgery highlighting the femur migration to its final resting place.
References
- Wedemeyer, Christian; Kauther, Max Daniel (2011-03-16). "Hemipelvectomy- only a salvage therapy?". Orthopedic Reviews. 3 (1): e4. doi:10.4081/or.2011.e4. ISSN 2035-8237. PMC 3144004. PMID 21808716.
- "Cedars-Sinai". www.cedars-sinai.edu. Retrieved 2020-07-16.
- "Cedars-Sinai". www.cedars-sinai.edu. Retrieved 2020-07-17.
- Ji, Tao; Guo, Wei (2019-06-19). "The evolution of pelvic endoprosthetic reconstruction after tumor resection". Annals of Joint. 4: 29. doi:10.21037/aoj.2019.06.01.