Loop diuretic
Loop diuretics are diuretics that act on the Na-K-Cl cotransporter along the thick ascending limb of the loop of Henle in nephrons of the kidneys.[4] They are primarily used in medicine to treat hypertension and edema often due to congestive heart failure or chronic kidney disease. While thiazide diuretics are more effective in patients with normal kidney function, loop diuretics are more effective in patients with impaired kidney function.[5]
| Loop diuretic | |
|---|---|
| Drug class | |
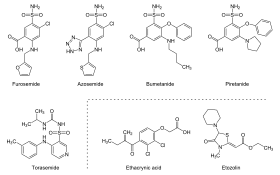 Structure of the loop diuretics Furosemide, Azosemide, Bumetanide, Piretanide, Torasemide, Ethacrynic acid and Etozolin | |
| Class identifiers | |
| Synonyms | High-ceiling diuretic[1] |
| Use | congestive heart failure, nephrotic syndrome, cirrhosis, hypertension, edema[2] |
| ATC code | C03C |
| Biological target | Na-K-Cl cotransporter[3] |
| External links | |
| MeSH | D049994 |
| Legal status | |
| In Wikidata | |
Mechanism of action
Loop diuretics are 90% bonded to proteins and are secreted into the proximal convoluted tubule through organic anion transporter 1 (OAT-1), OAT-2, and ABCC4. Loop diuretics act on the Na+-K+-2Cl− symporter (NKCC2) in the thick ascending limb of the loop of Henle to inhibit sodium, chloride and potassium reabsorption. This is achieved by competing for the Cl− binding site. Loop diuretics also inhibits NKCC2 at macula densa, reducing sodium transported into macula densa cells. This stimulates the release of renin, which through renin–angiotensin system, increases fluid retention in the body, increases the perfusion of glomerulus, thus increasing glomerular filtration rate (GFR). At the same time, loop diuretics inhibits the tubuloglomerular feedback mechanism so that increase in salts at the lumen near macula densa does not trigger a response that reduces the GFR.[6]
Loop diuretics also inhibit magnesium and calcium reabsorption in the thick ascending limb. Absorption of magnesium and calcium are dependent upon the positive voltage at the luminal side and less positive voltage at the interstitial side with transepithelial voltage gradient of 10 mV. This causes the magnesium and calcium ions to be repelled from luminal side to interstitial side, promoting their absorption. The difference in voltage in both sides are set up by potassium recycling through renal outer medullary potassium channel. By inhibiting the potassium recycling, the voltage gradient is abolished and magnesium and calcium reabsorption are inhibited.[7] By disrupting the reabsorption of these ions, loop diuretics prevent the generation of a hypertonic renal medulla. Without such a concentrated medulla, water has less of an osmotic driving force to leave the collecting duct system, ultimately resulting in increased urine production. Loop diuretics cause a decrease in the renal blood flow by this mechanism. This diuresis leaves less water to be reabsorbed into the blood, resulting in a decrease in blood volume.
A secondary effect of loop diuretics is to increase the production of prostaglandins, which results in vasodilation and increased blood supply to the kidney.[8][9]
The collective effects of decreased blood volume and vasodilation decrease blood pressure and ameliorate edema.
Pharmacokinetics
Loop diuretics are highly protein bound and therefore have a low volume of distribution. The protein bound nature of the loop diuretic molecules causes it to be secreted via several transporter molecules along luminal wall of the proximal convoluted tubules to be able to exert its function. The availability of furosemide is highly variable, ranging from 10% to 90%. The biological half-life of furosemide is limited by absorption from gastrointestinal tract into the bloodstream. The apparent half-life of its excretion is higher than the apparent half-life of absorption via oral route. Therefore, intravenous dose of furosemide is twice as potent as the oral route.[6]
However, for torsemide and bumetanide, their oral bioavailability is consistently higher than 90%. Torsemide has longer half life in heart failure patients (6 hours) when compared to furosemide (2.7 hours). Loop diuretics usually have a "ceiling" effect where there is a maximum level of dosage where further increase in dosage will not increase the clinical effect of the drug. A dose of 40 mg of furosemide is equivalent to 20 mg of torsemide and 1 mg bumetanide.[6]
Clinical use
Loop diuretics are principally used in the following indications:
- Heart failure - Giving 2.5 times of previous oral dose twice daily for those with acute decompensated heart failure is a reasonable strategy. However, daily assessment of clinical response is needed to adjust the subsequent doses.[6]
- Edema associated with liver cirrhosis, and nephrotic syndrome[10]
- Cerebral edema - intravenous furosemide can be combined with mannitol to initiate rapid diuresis. However, the optimum duration of such treatment remains unknown. Frequent fluid status monitoring is required to prevent intravascular volume depletion which leads to reduced cerebral perfusion. A bolus intravenous dose of 10 or 20 mg of furosemide can be administered and then followed by intravenous bolus of 2 or 3% hypertonic saline to increase the serum sodium level.[11]
- Pulmonary edema - Slow intravenous bolus dose of 40 to 80 mg furosemide at 4 mg per minute is indicated for patients with fluid overload and pulmonary edema. Such dose can be repeated after 20 minutes. After the bolus, a continuous intravenous infusion can be given at 5 to 10 mg per hour. For those with underlying renal impairment or severe heart failure, up to 160 to 200 mg bolus dose can be given.[12]
- Hypertension - A systematic review by the Cochrane Hypertension group assessing the anti-hypertensive effects of loop diuretics found only a modest reduction in blood pressure when compared to placebo.[13] According to Joint National Committee (JNC-8) guidelines, the first line treatment of hypertension is thiazide diuretics. The use of loop diuretics is not mentioned in this guideline. Meanwhile, according to 2013 European Society of Cardiology (ESC) guidelines, a loop diuretic can only replace thiazide-type diuretics if there is renal impairment (Creatinine of more than 1.5 mg/dL or estimated glomerular filtration rate (eGFR) of less 30 mL/min/1.73 m2 due to lack of long term cardiovascular outcome data and appropriate dosing regimen of its use.[14]
The 2012 KDIGO (Kidney Disease: Improving Global Outcomes) guidelines stated that diuretics should not be used to treat acute kidney injury, except for the management of volume overload. Diuretics has not shown any benefits of preventing or treating acute kidney injury.[15]
They are also sometimes used in the management of severe hypercalcemia in combination with adequate rehydration.[16]
Resistance
Diuretic resistance is defined as failure of diuretics to reduce fluid retention (can be measured by low urinary sodium) despite using the maximal dose of drugs. There are various causes for the resistance towards loop diuretics. After initial period of diuresis, there will be a period of "post-diuretic sodium retention" where the rate of sodium excretion does not reach as much as the initial diuresis period. Increase intake of sodium during this period will offset the amount of excreted sodium, and thus causing diuretic resistance. Prolonged usage of loop diuretics will also contributes to resistance through "braking phenomenon". This is the body physiological response to reduced extracellular fluid volume, where renin-angiotensin-aldosterone system will be activated which results in nephron remodelling. Nephron remodeling increases the number of distal convoluted cells, principle cells, and intercalated cells. These cells have sodium-chloride symporter at distal convoluted tubule, epithelial sodium channels, and chloride-bicarbonate exchanger pendrin. This will promote sodium reabsorption and fluid retention, causing diuretic resistance. Other factors includes gut edema which slows down the absorption of oral loop diuretics. Chronic kidney disease (CKD) reduces renal flow rate, reducing the delivery of diuretic molecules into the nephron, limiting sodium excretion and increasing sodium retention, causing diuretic resistance. Non-steroidal anti-inflammatory drug (NSAID) can compete with loop diuretics for organic ion transporters, thus preventing the diuretic molecules from being secreted into the proximal convoluted tubules.[6]
Those with diuretic resistance, cardiorenal syndrome, and severe right ventricular dysfunction may have better response to continuous diuretic infusion. Diuretic dosages is adjusted to produce 3 to 5 litres of urine per day. Thiazide (blockade of sodium-chloride symporter), amiloride (blockade of epithelial sodium channels) and carbonic anhydrase inhibitors (blockade of chloride-bicarbonate exchanger pendrin) has been suggested to complement the action of loop diuretics in resistance cases but limited evidence are available to support their use.[6]
Adverse effects
The most common adverse drug reactions (ADRs) are dose-related and arise from the effect of loop diuretics on diuresis and electrolyte balance.
Common ADRs include: hyponatremia, hypokalemia, hypomagnesemia, dehydration, hyperuricemia, gout, dizziness, postural hypotension, syncope.[16] The loss of magnesium as a result of loop diuretics has also been suggested as a possible cause of pseudogout (chondrocalcinosis).[17]
Infrequent ADRs include: dyslipidemia, increased serum creatinine concentration, hypocalcemia, rash. Metabolic alkalosis may also be seen with loop diuretic use.
Ototoxicity (damage to the inner ear) is a serious, but rare ADR associated with use of loop diuretics. This may be limited to tinnitus and vertigo, but may result in deafness in serious cases.
Loop diuretics may also precipitate kidney failure in patients concurrently taking an NSAID and an ACE inhibitor—the so-called "triple whammy" effect.[18]
Because furosemide, torsemide and bumetanide are technically sulfa drugs, there is a theoretical risk that patients sensitive to sulfonamides may be sensitive to these loop diuretics. This risk is stated on drug packaging inserts. However, the actual risk of crossreactivity is largely unknown and there are some sources that dispute the existence of such cross reactivity.[19][20] In one study it was found that only 10% of patients with allergy to antibiotic sulfonamides were also allergic to diuretic sulfonamides, but it is unclear if this represents true cross reactivity or the nature of being prone to allergy.[21]
Ethacrynic acid is the only medication of this class that is not a sulfonamide. It has a distinct complication of being associated with gastrointestinal toxicity.[22]
Examples
| Loop Diuretic | Relative Potency[23] |
|---|---|
| Furosemide | 40 mg |
| Bumetanide | 1 mg |
| Ethacrynic Acid | 50 mg |
| Torsemide | 20 mg |
References
- "WHOCC - ATC/DDD Index". www.whocc.no. Retrieved 9 April 2022.
- Huxel, Chris; Raja, Avais; Ollivierre-Lawrence, Michelle D. (2022). "Loop Diuretics". StatPearls. StatPearls Publishing. PMID 31536262. Retrieved 9 April 2022.
- Khan, M. Gabriel (1 January 2006). "Diuretics". Encyclopedia of Heart Diseases. pp. 313–318. doi:10.1016/b978-012406061-6/50053-9. ISBN 9780124060616. Retrieved 9 April 2022.
{{cite book}}:|website=ignored (help) - Huxel, Chris; Raja, Avais; Ollivierre-Lawrence, Michelle D. (2022). "Loop Diuretics". StatPearls. StatPearls Publishing. PMID 31536262. Retrieved 13 April 2022.
- Wile, D (Sep 2012). "Diuretics: a review". Annals of Clinical Biochemistry. 49 (Pt 5): 419–31. doi:10.1258/acb.2011.011281. PMID 22783025.
- Ingelfinger, Julie R (16 November 2017). "Diuretic Treatment in Heart Failure". The New England Journal of Medicine. 377 (20): 1964–1975. doi:10.1056/NEJMra1703100. PMC 5811193. PMID 29141174.
- Rose, BD (Feb 1991). "Diuretics". Kidney International. 39 (2): 336–52. doi:10.1038/ki.1991.43. PMID 2002648.
- Liguori, A.; A. Casini; M. Di Loreto; I. Andreini; C. Napoli (1999). "Loop diuretics enhance the secretion of prostacyclin in vitro, in healthy persons, and in patients with chronic heart failure". European Journal of Clinical Pharmacology. 55 (2): 117–124. doi:10.1007/s002280050605. ISSN 0031-6970. PMID 10335906. S2CID 39588076.
- Miyanoshita, A.; M. Terada; H. Endou (1989). "Furosemide directly stimulates prostaglandin E2 production in the thick ascending limb of Henle's loop". The Journal of Pharmacology and Experimental Therapeutics. 251 (3): 1155–1159. ISSN 0022-3565. PMID 2600809.
- O'Brien, James G; Chennubthotla, Shobha A (1 June 2005). "Treatment of Edema". American Family Physician. 71 (11): 2111–2117. PMID 15952439. Retrieved 5 March 2018.
- Ahmed, Raslan; Anish, Bhardwaj (2007). "Medical management of cerebral edema". Neurosurgical Focus. 22 (5): E12. doi:10.3171/foc.2007.22.5.13. PMID 17613230.
- Megan, Purvey; George, Allen (April 2017). "Managing acute pulmonary oedema". Australian Prescriber. 40 (2): 59–63. doi:10.18773/austprescr.2017.013. PMC 5408000. PMID 28507398.
- Musini, VM; Rezapour, P; Wright, JM; Bassett, K; Jauca, CD (2015). "Blood pressure-lowering efficacy of loop diuretics for primary hypertension". Cochrane Database of Systematic Reviews. 2015 (5): CD003825. doi:10.1002/14651858.CD003825.pub4. PMC 7156893. PMID 26000442.
- Line, Malha; Samuel, J Mann (7 March 2016). "Loop Diuretics in the Treatment of Hypertension". Current Hypertension Reports. 18 (27): 27. doi:10.1007/s11906-016-0636-7. PMID 26951244. S2CID 22999638.
- Claire, Annie; Fredette, Nadeau; Bouchard, Josée (January 2013). "Fluid Management and Use of Diuretics in Acute Kidney Injury". Advances in Chronic Kidney Disease. 20 (1): 45–55. doi:10.1053/j.ackd.2012.09.005. PMID 23265596.
- Rossi S, ed. (2004). Australian Medicines Handbook 2004 (5th ed.). Adelaide, S.A.: Australian Medicines Handbook Pty Ltd. ISBN 978-0-9578521-4-3.
- Rho, YH; Zhu, Y; Zhang, Y; Reginato, AM; Choi, HK (2012). "Risk factors for pseudogout in the general population". Rheumatology. 51 (11): 2070–2074. doi:10.1093/rheumatology/kes204. PMC 3475980. PMID 22886340.
- Thomas MC (February 2000). "Diuretics, ACE inhibitors and NSAIDs--the triple whammy". Med. J. Aust. 172 (4): 184–5. doi:10.5694/j.1326-5377.2000.tb125548.x. PMID 10772593. S2CID 37558579.
- Phipatanakul, Wanda; N. Franklin Adkinson (2000). "Cross-Reactivity Between Sulfonamides and Loop or Thiazide Diuretics: Is it a Theoretical or Actual Risk?". Allergy & Clinical Immunology International. 12 (1): 26–28. doi:10.1027/0838-1925.12.1.26. ISSN 1097-1424. PMC 3365608. PMID 22661885.
- Rachoin, Jean-Sebastien; Elizabeth A. Cerceo (2011). "Four nephrology myths debunked". Journal of Hospital Medicine. 6 (5): –1–5. doi:10.1002/jhm.703. ISSN 1553-5606. PMID 21661096.
- Strom, Brian L.; Rita Schinnar; Andrea J. Apter; David J. Margolis; Ebbing Lautenbach; Sean Hennessy; Warren B. Bilker; Dan Pettitt (2003-10-23). "Absence of cross-reactivity between sulfonamide antibiotics and sulfonamide nonantibiotics". The New England Journal of Medicine. 349 (17): 1628–1635. doi:10.1056/NEJMoa022963. ISSN 1533-4406. PMID 14573734.
- Laragh, John H.; Paul J. Cannon; William B. Stason; Henry O. Heinemann (1966). "Physiologic and Clinical Observations on Furosemide and Ethacrynic Acid*". Annals of the New York Academy of Sciences. 139 (2): 453–465. Bibcode:1966NYASA.139..453L. doi:10.1111/j.1749-6632.1966.tb41219.x. ISSN 1749-6632. PMID 5339515. S2CID 6942431.
- Goodman & Gilman's pharmacological basis of therapeutics. Goodman, Louis S. (Louis Sanford), 1906-2000., Brunton, Laurence L., Chabner, Bruce., Knollmann, Björn C. (12th ed.). New York: McGraw-Hill. 2011. ISBN 9780071624428. OCLC 498979404.
{{cite book}}: CS1 maint: others (link)
External links
- Loop Diuretic, from the Family Practice Notebook