Molluscum contagiosum
Molluscum contagiosum (MC), sometimes called water warts, is a viral infection of the skin that results in small raised pink lesions with a dimple in the center.[1] They may become itchy or sore, and occur singularly or in groups.[1] Any area of the skin may be affected, with abdomen, legs, arms, neck, genital area, and face being the most common.[1] Onset of the lesions is around seven weeks after infection.[3] They usually go away within a year without scarring.[1]
| Molluscum contagiosum | |
|---|---|
| Other names | Water warts |
 | |
| Typical flesh-colored, dome-shaped and pearly lesions | |
| Specialty | Dermatology |
| Symptoms | Small, raised, pink lesions with a dimple in the center[1] |
| Usual onset | Children 1 to 10 years of age[2] |
| Duration | Usually 6–12 months, may last up to four years[1] |
| Types | MCV-1, MCV-2, MCV-3, MCV-4[3] |
| Causes | Molluscum contagiosum virus spread by direct contact or contaminated objects[4] |
| Risk factors | Weak immune system, atopic dermatitis, crowded living conditions[2] |
| Diagnostic method | Based on appearance[3] |
| Differential diagnosis | Warts, herpes simplex, chickenpox, folliculitis[5] |
| Prevention | Hand washing, not sharing personal items[6] |
| Treatment | None, freezing, opening up the lesion and scraping the inside, laser therapy[7] |
| Medication | Cimetidine, podophyllotoxin[7] |
| Frequency | 122 million / 1.8% (2010)[8] |
The infection is caused by a poxvirus called the molluscum contagiosum virus (MCV).[1] The virus is spread either by direct contact, including sexual activity, or via contaminated objects such as towels.[4] The condition can also be spread to other areas of the body by the person themselves.[4] Risk factors include a weak immune system, atopic dermatitis, and crowded living conditions.[2] Following one infection, it is possible to get re-infected.[9] Diagnosis is typically based on the appearance of the lesions.[3]
Prevention includes hand washing and not sharing personal items.[6] While treatment is not necessary, some may wish to have the lesions removed for cosmetic reasons or to prevent spread.[7] Removal may occur with freezing, laser therapy, or opening up the lesion and scraping the inside.[7] Scraping the lesion can, however, result in scarring.[9] The oral medication cimetidine, or podophyllotoxin cream applied to the skin, may also be used for treatment.[7]
Approximately 122 million people globally were affected by molluscum contagiosum as of 2010 (1.8% of the population).[8] It is more common in children between the ages of one and ten years old.[2] The condition has become more common in the United States since 1966.[2] But having an infection is not a reason to keep a child out of school or daycare.[10]
Signs and symptoms

Molluscum contagiosum lesions are flesh-colored, dome-shaped, and pearly in appearance. They are often 1–5 mm in diameter, with a dimpled center.[11] Molluscum lesions are most commonly found on the face, arms, legs, torso, and armpits in children. Adults typically have molluscum lesions in the genital region and this is considered to be a sexually transmitted infection; because of this, if genital lesions are found on a child, sexual abuse should be suspected.[3] These lesions are generally not painful, but they may itch or become irritated. Picking or scratching the bumps may lead to a spread of the viral infection responsible for molluscum contagiosum, an additional bacterial infection, and scarring.[3][12] In some cases, eczema develops around the lesions.[13]
Individual molluscum lesions may go away on their own within two months and generally clear completely without treatment or scarring in six to twelve months.[3] Mean durations for an outbreak are variously reported from eight[14] to about 18 months,[15][16] but durations are reported as widely as six months to five years, lasting longer in immunosuppressed individuals.[16]
Transmission
As the name implies, molluscum contagiosum is extremely contagious.[3] Transmission of the molluscum contagiosum virus can occur many different ways including direct skin contact (e.g., contact sports or sexual activity), contact with an infected surface (fomite), or autoinoculation (self-infection) by scratching or picking molluscum lesions and then touching other parts of the skin not previously affected by the virus.[3] Children are particularly susceptible to autoinoculation and may have widespread clusters of lesions.[17]
The viral infection is limited to a localized area on the topmost layer of the superficial layer of the skin.[18] Once the virus-containing head of the lesion has been destroyed, the infection is gone. The central waxy core contains the virus.
Diagnosis
Diagnosis is made on the appearance; the virus cannot routinely be cultured. The diagnosis can be confirmed by excisional biopsy.
Histologically, molluscum contagiosum is characterized by molluscum bodies (also known as Henderson-Patterson bodies) in the epidermis, above the stratum basale, which consist of cells with abundant large granular eosinophilic cytoplasmic inclusion bodies (accumulated virions) and a small nucleus that has been pushed to the periphery.[19][20]
 Low magnification micrograph of a molluscum contagiosum lesion
Low magnification micrograph of a molluscum contagiosum lesion Low-magnification micrograph of molluscum contagiosum, H&E stain
Low-magnification micrograph of molluscum contagiosum, H&E stain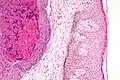 High-magnification micrograph of molluscum contagiosum, showing the characteristic molluscum bodies, H&E stain
High-magnification micrograph of molluscum contagiosum, showing the characteristic molluscum bodies, H&E stain
Management
Because molluscum contagiosum usually resolves without treatment and treatment options can cause discomfort to children, initial recommendations are often to simply wait for the lesions to resolve on their own.[21] Of the treatments available, a meta-analysis of randomized controlled trials suggested that there is no difference between treatments in short term improvement, and no single treatment is significantly better than natural resolution of the condition.[22]
Bumps located in the genital area may be treated in an effort to prevent them from spreading.[16] When treatment has resulted in the elimination of all bumps, the infection has been effectively cured and will not reappear unless the person is reinfected.[23]
Medications
For mild cases, over-the-counter wart medicines, such as salicylic acid may[24] shorten infection duration. Daily topical application of tretinoin cream may also trigger resolution.[25]
Studies have found cantharidin to be an effective and safe treatment for removing molluscum contagiosum.[26] This medication is usually well tolerated though mild side effects such as pain or blistering are common.[26] There is no high-quality evidence for cimetidine.[27] However, oral cimetidine has been used as an alternative treatment for the pediatric population as it is generally well tolerated and less invasive.[28]
Imiquimod
Imiquimod is a form of immunotherapy initially proposed as a treatment for molluscum based on promising results in small case series and clinical trials.[29] However, two large randomized controlled trials, specifically requested by the U.S. Food and Drug Administration under the Best Pharmaceuticals for Children Act both demonstrated that imiquimod cream applied three times per week was no more effective than placebo cream for treating molluscum after 18 weeks of treatment in a total of 702 children aged 2–12 years.[30] In 2007, results from those trials—which remain unpublished—were incorporated into FDA-approved prescribing information for imiquimod, which states: "Limitations of Use: Efficacy was not demonstrated for molluscum contagiosum in children aged 2–12."[30][31] In 2007, the FDA also updated imiquimod's label concerning safety issues raised in the two large trials and an FDA-requested pharmacokinetic study (the latter of which was published).[30] The updated safety label reads as follows:
- Potential adverse effects of imiquimod use: "Similar to the studies conducted in adults, the most frequently reported adverse reaction from 2 studies in children with molluscum contagiosum was application site reaction. Adverse events which occurred more frequently in Aldara-treated subjects compared with vehicle-treated subjects generally resembled those seen in studies in indications approved for adults and also included otitis media (5% Aldara vs. 3% vehicle) and conjunctivitis (3% Aldara vs. 2% vehicle). Erythema was the most frequently reported local skin reaction. Severe local skin reactions reported by Aldara-treated subjects in the pediatric studies included erythema (28%), edema (8%), scabbing/crusting (5%), flaking/scaling (5%), erosion (2%) and weeping/exudate (2%)."
- Potential systemic absorption of imiquimod, with negative effects on white blood cell counts overall, and specifically neutrophil counts: "Among the 20 subjects with evaluable laboratory assessments, the median WBC count decreased by 1.4*109/L and the median absolute neutrophil count decreased by 1.42×109 L−1."[32]
Surgery
Surgical treatments include cryosurgery, in which liquid nitrogen is used to freeze and destroy lesions, as well as scraping them off with a curette. Application of liquid nitrogen may cause burning or stinging at the treated site, which may persist for a few minutes after the treatment. With liquid nitrogen, a blister may form at the treatment site, but it will slough off in two to four weeks. Cryosurgery and curette scraping can be painful procedures and can result in residual scarring.[33]
Laser
A 2014 systematic review of case reports and case series concluded that the limited available data suggest pulsed dye laser therapy is a safe and effective treatment for molluscum contagiosum and is generally well tolerated by children.[33] Side effects seen with pulsed dye laser therapy included mild temporary pain at the site of therapy, bruising (lasting up to 2–3 weeks), and temporary discoloration of the treated skin (as long as 1–6 months).[33] No cases of permanent scarring have been reported.[33] As of 2009, however, there is no evidence for genital lesions.[34]
Prognosis
Most cases of molluscum contagiosum will clear up naturally within two years (usually within nine months). So long as the skin growths are present, there is a possibility of transmitting the infection to another person. When the growths are gone, the possibility of spreading the infection is ended.[23]
Unlike herpesviruses, which can remain inactive in the body for months or years before reappearing, molluscum contagiosum does not remain in the body when the growths are gone from the skin and will not reappear on their own.[23]
Epidemiology
As of 2010, approximately 122 million people were affected worldwide by molluscum contagiosum (1.8% of the population).[8]
See also
- Acrochordons (also called skin tags—similar in appearance and grow in similar areas)
- Basal-cell carcinoma
- Wart (caused by the human papillomavirus; also similar in appearance to molluscum)
References
- "Molluscum Contagiosum". www.cdc.gov. 11 May 2015. Archived from the original on 16 June 2017. Retrieved 10 June 2017.
- "Risk Factors | Molluscum Contagiosum". www.cdc.gov. 11 May 2015. Archived from the original on 10 June 2017. Retrieved 10 June 2017.
- Ramdass, P; Mullick, S; Farber, HF (December 2015). "Viral Skin Diseases". Primary Care (Review). 42 (4): 517–67. doi:10.1016/j.pop.2015.08.006. PMID 26612372.
- "Transmission | Molluscum Contagiosum". www.cdc.gov. 11 May 2015. Archived from the original on 10 June 2017. Retrieved 10 June 2017.
- Ferri, Fred F. (2010). Ferri's differential diagnosis : a practical guide to the differential diagnosis of symptoms, signs, and clinical disorders (2nd ed.). Philadelphia, PA: Elsevier/Mosby. p. Chapter M. ISBN 978-0323076999.
- "Prevention | Molluscum Contagiosum". www.cdc.gov. 11 May 2015. Archived from the original on 17 June 2017. Retrieved 10 June 2017.
- "Treatment Options | Molluscum Contagiosum". www.cdc.gov. 11 May 2015. Archived from the original on 17 June 2017. Retrieved 10 June 2017.
- Vos, Theo; Flaxman, D; Naghavi, A; et al. (December 2012). "Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010". Lancet. 380 (9859): 2163–96. doi:10.1016/S0140-6736(12)61729-2. PMC 6350784. PMID 23245607.
- "Long Term Effects | Molluscum Contagiosum". www.cdc.gov. 11 May 2015. Archived from the original on 17 June 2017. Retrieved 10 June 2017.
- "Day Care Centers and Schools | Molluscum Contagiosum". www.cdc.gov. 11 May 2015. Archived from the original on 17 June 2017. Retrieved 10 June 2017.
- Likness, LP (June 2011). "Common dermatologic infections in athletes and return-to-play guidelines". The Journal of the American Osteopathic Association. 111 (6): 373–379. doi:10.7556/jaoa.2011.111.6.373. PMID 21771922.
- Basta-Juzbašić, A; Čeović, R (March 2014). "Chancroid, lymphogranuloma venereum, granuloma inguinale, genital herpes simplex infection, and molluscum contagiosum". Clinics in Dermatology (Review). 32 (2): 290–8. doi:10.1016/j.clindermatol.2013.08.013. PMID 24559566.
- "Molluscum contagiosum | DermNet NZ". dermnetnz.org. Retrieved 2021-07-30.
- Weller R, O'Callaghan CJ, MacSween RM, White MI (1999). "Scarring in molluscum contagiosum: comparison of physical expression and phenol ablation". BMJ. 319 (7224): 1540. doi:10.1136/bmj.319.7224.1540. PMC 28297. PMID 10591712.
- MedlinePlus Encyclopedia: Molluscum Contagiosum
- Tyring SK (2003). "Molluscum contagiosum: the importance of early diagnosis and treatment". Am. J. Obstet. Gynecol. 189 (3 Suppl): S12–6. doi:10.1067/S0002-9378(03)00793-2. PMID 14532898.
- "Molluscum Contagiosum". The Lecturio Medical Concept Library. Retrieved 11 August 2021.
- "Pamphlets: Molluscum Contagiosum". American Academy of Dermatology. 2006. Archived from the original on 2008-12-01. Retrieved 2008-11-30.
- Chen, X; Anstey, AV; Bugert, JJ (October 2013). "Molluscum contagiosum virus infection". Lancet Infectious Diseases. 13 (10): 877–88. doi:10.1016/S1473-3099(13)70109-9. PMID 23972567.
- Rao, K; Priya, N; Umadevi, H; Smitha, T (January 2013). "Molluscum contagiosum". Journal of Oral and Maxillofacial Pathology. 17 (1): 146–7. doi:10.4103/0973-029X.110726. PMC 3687174. PMID 23798852.
- Prodigy knowledgebase (July 2003). "Molluscum Contagiosum". National Health Service. Archived from the original on 2010-10-13. Retrieved 2010-04-20.
- van der Wouden, Johannes C; van der Sande, Renske; Kruithof, Emma J; Sollie, Annet; van Suijlekom-Smit, Lisette WA; Koning, Sander (2017-05-17). "Interventions for cutaneous molluscum contagiosum". Cochrane Database of Systematic Reviews. 2017 (5): CD004767. doi:10.1002/14651858.CD004767.pub4. ISSN 1465-1858. PMC 6481355. PMID 28513067.
- "Frequently Asked Questions: For Everyone. CDC Molluscum Contagiosum". United States Centers for Disease Control and Prevention. Archived from the original on 2008-12-19. Retrieved 2008-12-08.
- Schmitt, Jochen; Diepgen, Thomas L. (2008). "Molluscum contagiosum" (PDF). In Berthold Rzany; Williams, Hywel; Bigby, Michael E.; Diepgen, Thomas L.; Herxheimer, Andrew; Luigi Naldi (eds.). Evidence-Based Dermatology. Evidence-based Medicine. London: BMJ Books. ISBN 978-1-4051-4518-3. Archived from the original (PDF) on 2009-02-19.
- Credo, BV; Dyment, PG (1996). "Molluscum Contagiosum". Adolesc Med. 7 (1): 57–62. PMID 10359957.
- Torbeck R, Pan M, DeMoll E, Levitt J (June 2014). "Cantharidin: a comprehensive review of the clinical literature". Dermatology Online Journal (Review). 20 (6). doi:10.5070/D3206022861. PMID 24945640. Archived from the original on 2016-03-04.
- Scheinfeld N (March 2003). "Cimetidine: a review of the recent developments and reports in cutaneous medicine". Dermatol. Online J. 9 (2): 4. doi:10.5070/D33S15Q645. PMID 12639457. Archived from the original on 2008-09-28.
- "Treatment Options - Molluscum Contagiosum - Pox viruses - CDC". www.cdc.gov. 2 October 2017.
- Hanna D, Hatami A, Powell J, et al. (2006). "A prospective randomized trial comparing the efficacy and adverse effects of four recognized treatments of molluscum contagiosum in children". Pediatric Dermatology. 23 (6): 574–9. doi:10.1111/j.1525-1470.2006.00313.x. PMID 17156002. S2CID 43224667.
- Katz, KA (February 2015). "Dermatologists, imiquimod, and treatment of molluscum contagiosum in children: righting wrongs". JAMA Dermatology. 151 (2): 125–6. doi:10.1001/jamadermatol.2014.3335. PMID 25587702.
- Katz, KA; Swetman, GL (July 2013). "Imiquimod, molluscum, and the need for a better "best pharmaceuticals for children" act". Pediatrics. 132 (1): 1–3. doi:10.1542/peds.2013-0116. PMID 23796740. S2CID 29556501.
- DailyMed. Aldara (imiquimod) Cream for Topical use (Prescribing information): "DailyMed". Archived from the original on 2013-07-16. Retrieved 2013-07-17.
- Griffith, RD; Yazdani Abyaneh, MA; Falto-Aizpurua, L; Nouri, K (November 2014). "Pulsed dye laser therapy for molluscum contagiosum: a systematic review". Journal of Drugs in Dermatology (Review). 13 (11): 1349–52. PMID 25607701.
- Brown, M; Paulson, C; Henry, SL (Oct 15, 2009). "Treatment for anogenital molluscum contagiosum". American Family Physician. 80 (8): 864. PMID 19835348.
External links
- Molluscum—Center for Disease Control
- Virus Pathogen Database and Analysis Resource (ViPR): Poxviridae