Multiple endocrine neoplasia type 2B
Multiple endocrine neoplasia type 2B (MEN 2B) is a genetic disease that causes multiple tumors on the mouth, eyes, and endocrine glands. It is the most severe type of multiple endocrine neoplasia,[2] differentiated by the presence of benign oral and submucosal tumors in addition to endocrine malignancies. It was first described by Wagenmann in 1922,[3] and was first recognized as a syndrome in 1965-1966 by E.D. Williams and D.J. Pollock.[4][5] It is caused by the pathogenic variant p.Met918Thr in the RET gene. This variant can cause medullary thyroid cancer and Pheochromocytoma. Presentation can include a Marfanoid body, enlarged lips, and ganglionueuromas.
| Multiple endocrine neoplasia type 2b | |
|---|---|
| Other names | MEN 2B, Mucosal neuromata with endocrine tumors, Multiple endocrine neoplasia type 3 ,Wagenmann–Froboese syndrome[1] |
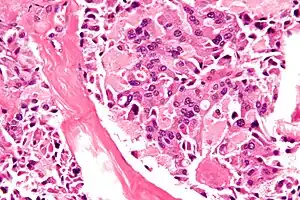 | |
| Micrograph of medullary thyroid carcinoma, as may be seen in MEN 2b. H&E stain. | |
| Specialty | Endocrinology |
MEN 2B typically manifests before a child is 10 years old. Affected individuals tend to be tall and lanky, with an elongated face and protruding, blubbery lips. Benign tumors (neoplasms) develop in the mouth, eyes, and submucosa of almost all organs in the first decade of life.[6] Medullary thyroid cancer almost always occurs, sometimes in infancy. It is often aggressive. Cancer of the adrenal glands (pheochromocytoma) occurs in 50% of cases.
A variety of eponyms have been proposed for MEN 2B, such as Williams-Pollock syndrome, Gorlin-Vickers syndrome, and Wagenmann-Froboese syndrome. However, none ever gained sufficient traction to merit continued use, and they are no longer used in the medical literature.[7]
The prevalence of MEN2B is not well established, but has been derived from other epidemiological considerations as 1 in 600,000[8] to 1 in 4,000,000.[9] The annual incidence has been estimated at 4 per 100 million per year.[10]
Signs and symptoms
The most common clinical features of MEN2B are:
- a tall, thin, "marfanoid" body build, in which long bones are disproportionately elongated;
- masses beneath mucosal surfaces in the mouth, lips, and eyes (discussed below);
- low muscle mass, sometimes with myopathy;
- gastrointestinal complaints, especially constipation;
- symptoms derived from medullary carcinoma of the thyroid;
- symptoms derived from pheochromocytoma;
- craniosynostosis;
- dry eyes or lack of tears;
- delayed puberty.

Unlike Marfan syndrome, the cardiovascular system and the lens of the eye are unaffected. Mucosal neuromas are the most consistent and distinctive feature, appearing in 100% of patients.[11] Usually there are numerous yellowish-white, sessile, painless nodules on the lips or tongue, with deeper lesions having normal coloration. There may be enough neuromas in the body of the lips to produce enlargement and a "blubbery lip" appearance. Similar nodules may be seen on the sclera and eyelids.
Histologically, neuromata contain a characteristic adventitious plaque of tissue composed of hyperplastic, interlacing bands of Schwann cells and myelinated fibers overlay the posterior columns of the spinal cord.[12] Mucosal neuromas are made up of nerve cells, often with thickened perineurium, intertwined with one another in a plexiform pattern. This tortuous pattern of nerves is seen within a background of loose endoneurium-like fibrous stroma.
Causes
Variations in the RET proto-oncogene cause MEN2B. In recent decades no case of MEN2B has been reported that lacks such a variation. The M918T variant alone is responsible for approximately 95% of cases.[13] All DNA variants that cause MEN2B are thought to enhance signaling through the RET protein, which is a receptor molecule found on cell membranes, whose ligands are part of the transforming growth factor beta signaling system.
About half of cases are inherited from a parent as an autosomal dominant trait. The other half appear to be spontaneous mutations,[2] usually arising in the paternal allele,[14] particularly from older fathers.[2] The sex ratio in de novo cases is also uneven: sons are twice as likely to develop MEN 2B as daughters.[2]
Diagnosis
Differential diagnosis
DNA testing is now the preferred method of establishing a diagnosis for MEN 2B, and is thought to be almost 100% sensitive and specific. Gordon et al. reported cases of a difference disease—the "multiple mucosal neuroma syndrome"—having the physical phenotype of MEN2B, but without variations in the RET gene and without malignancy.[15]
MEN2B should be entertained as a diagnosis whenever a person is found to have either medullary thyroid carcinoma or pheochromocytoma. Before DNA testing became available, measurement of serum calcitonin was the most important laboratory test for MEN2B. Calcitonin is produced by the "C" cells of the thyroid, which, because they are always hyperplastic or malignant in MEN2B, produce more calcitonin than normal. Calcitonin levels remain a valuable marker to detect recurrence of medullary thyroid carcinoma after thyroidectomy.
Luxol fast blue staining identifies myelin sheathing of some fibers, and lesional cells react immunohistochemically for S-100 protein, collagen type IV, vimentin, NSE, and neural filaments. More mature lesions will react also for EMA, indicating a certain amount of perineurial differentiation. Early lesions, rich in acid mucopolysaccharides, stain positively with alcian blue. When medullary thyroid cancer is present, levels of the hormone calcitonin are elevated in serum and urine.[13] Under the microscope, tumors may closely resemble traumatic neuroma, but the streaming fascicles of mucosal neuroma are usually more uniform and the intertwining nerves of the traumatic neuroma lack the thick perineurium of the mucosal neuroma.[16] Inflammatory cells are not seen in the stroma and dysplasia is not present in the neural tissues.
Treatment
Without treatment, persons with MEN2B die prematurely. Details are lacking, owing to the absence of formal studies, but it is generally assumed that death in the 30s is typical unless prophylactic thyroidectomy and surveillance for pheochromocytoma are performed (see below). The range is quite variable, however: death early in childhood can occur, and a few untreated persons have been diagnosed in their 50s.[17] Recently, a larger experience with the disease "suggests that the prognosis in an individual patient may be better than previously considered."[18]
Thyroidectomy is the mainstay of treatment, and should be performed without delay as soon as a diagnosis of MEN2B is made, even if no malignancy is detectable in the thyroid. Without thyroidectomy, almost all patients with MEN2B develop medullary thyroid cancer, in a more aggressive form than MEN 2A.[13][19] The ideal age for surgery is 4 years old or younger, since cancer may metastasize before age 10.[14]
Pheochromocytoma - a hormone secreting tumor of the adrenal glands - is also present in 50% of cases.[14] Affected individuals are encouraged to get yearly screenings for thyroid and adrenal cancer.
Because prophylactic thyroidectomy improves survival, blood relatives of a person with MEN2B should be evaluated for MEN2B, even if lacking the typical signs and symptoms of the disorder.The mucosal neuromas of this syndrome are asymptomatic and self-limiting, and present no problem requiring treatment. They may, however, be surgically removed for aesthetic purposes or if they are being constantly traumatized.
Society and culture
Abraham Lincoln hypothesis
In 2007, Dr. John Sotos proposed that President Abraham Lincoln had MEN2B.[20] This theory suggests Lincoln had all the major features of the disease: a marfan-like body habitus, large, bumpy lips, constipation, muscular hypotonia, a history compatible with cancer and a family history of the disorder - his sons Eddie, Willie, and Tad, and probably his mother. The "mole" on Lincoln's right cheek, the asymmetry of his face, his large jaw, his drooping eyelid, and "pseudo-depression" are also suggested as manifestations of MEN2B. Lincoln's longevity (dying at 56 of a gunshot wound and without any apparent suggestion of ill health otherwise) is the principal challenge to the MEN2B theory, which could be proven by DNA testing.[21][22]
See also
References
- Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. p. 858. ISBN 978-1-4160-2999-1.
- Carlson KM, Bracamontes J, Jackson CE, et al. (December 1994). "Parent-of-origin effects in multiple endocrine neoplasia type 2B". Am. J. Hum. Genet. 55 (6): 1076–82. PMC 1918453. PMID 7977365.
- Wagenmann A. (1922). "Multiple neurome des Auges und der Zunge". Ber Dtsch Ophthalmol Ges. 43: 282–5.
- Williams ED (1965). "A review of 17 cases of carnicoma of the thyroid and phaeochromocytoma". J Clin Pathol. 18 (3): 288–292. doi:10.1136/jcp.18.3.288. PMC 472926. PMID 14304238.
- Williams, E. D., Pollock, D. J. (1966). "Multiple mucosal neuromata with endocrine tumours: a syndrome allied to von Recklinghausen's disease". J. Pathol. Bacteriol. 91 (1): 71–80. doi:10.1002/path.1700910109. PMID 4957444.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - Fryns JP, Chrzanowska K (October 1988). "Mucosal neuromata syndrome (MEN type IIb (III))". J. Med. Genet. 25 (10): 703–6. doi:10.1136/jmg.25.10.703. PMC 1051565. PMID 2906373.
- Schimke RN, Hartmann WH, Prout TE, Rimoin DL (1968). "Syndrome of bilateral pheochromocytoma, medullary thyroid carcinoma and multiple neuromas. A possible regulatory defect in the differentiation of chromaffin tissue". N. Engl. J. Med. 279 (1): 1–7. doi:10.1056/NEJM196807042790101. PMID 4968712.
- Marx, Stephen J (2011). "Chapter 41: Multiple endocrine neoplasia". In Melmed, Shlomo (ed.). Williams Textbook of Endocrinology, 12th ed. pp. 1728–1767.
- Moline J, Eng C (2011). "Multiple endocrine neoplasia type 2: an overview". Genetics in Medicine. 13 (9): 755–764. doi:10.1097/GIM.0b013e318216cc6d. PMID 21552134. S2CID 22402472.
- Martino Ruggieri (2005). Neurocutaneous Disorders : The Phakomatoses. Berlin: Springer. ISBN 978-3-211-21396-4. - Chapter: Multiple Endocrine Neoplasia Type 2B by Electron Kebebew, Jessica E. Gosnell and Emily Reiff. Pages 695-701. This reference quotes a prevalence of 1 in 40,000, but this figure is inconsistent with the same reference's calculated incidence of 4 per 100 million per year for MEN2B.
- Pujol RM, Matias-Guiu X, Miralles J, Colomer A, de Moragas JM (August 1997). "Multiple idiopathic mucosal neuromas: a minor form of multiple endocrine neoplasia type 2B or a new entity?". J. Am. Acad. Dermatol. 37 (2 Pt 2): 349–52. doi:10.1016/S0190-9622(97)70025-2. PMID 9270546.
- Dyck, PJ (October 1979). "Multiple endocrine neoplasia, type 2b: phenotype recognition; neurological features and their pathological basis". Annals of Neurology. 6 (4): 302–314. doi:10.1002/ana.410060404. PMID 554522. S2CID 24328061.
- Sperling, Mark A. (2008). Pediatric Endocrinology (3 ed.). Elsevier Health Sciences. pp. 246–7. ISBN 978-1-4160-4090-3.
- Morrison PJ, Nevin NC (September 1996). "Multiple endocrine neoplasia type 2B (mucosal neuroma syndrome, Wagenmann-Froboese syndrome)". J. Med. Genet. 33 (9): 779–82. doi:10.1136/jmg.33.9.779. PMC 1050735. PMID 8880581.
- Gordon CM, Majzoub JA, Marsh DJ, Mulliken JB, Ponder BA, Robinson BG, Eng C (January 1998). "Four cases of mucosal neuroma syndrome: multiple endocrine neoplasm 2B or not 2B?". J Clin Endocrinol Metab. 83 (1): 17–20. doi:10.1210/jcem.83.1.4504. PMID 9435410.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - R. L. Miller; N. J. Burzynski; B. L. Giammara (1977). "The ultrastructure of oral neuromas in multiple mucosal neuromas, pheochromocytoma, medullary thyroid carcinoma syndrome". Journal of Oral Pathology & Medicine. 6 (5): 253–63. doi:10.1111/j.1600-0714.1977.tb01647.x. PMID 409817. Archived from the original on 13 October 2012.
- Sizemore GW, Carney JA, Gharib H, Capen CC (1992). "Multiple endocrine neoplasia type 2B: eighteen-year follow-up of a four-generation family". Henry Ford Hosp Med J. 40 (3–4): 236–244. PMID 1362413.
- Hoff, AO; Gagel, RF (2006). "Chapter 192: Multiple endocrine neoplasia type 2". In DeGroot, LJ; Jameson, JL (eds.). Endocrinology (5th ed.). Philadelphia: Elsevier-Saunders. pp. 3533–3550. ISBN 978-0721603766.
- Lester W. Burket; Martin S. Greenberg; Michaël Glick; Jonathan A. Ship (2008). Burket's oral medicine (11 ed.). PMPH-USA. p. 141. ISBN 978-1-55009-345-2.
- Sotos, JG (2008). The Physical Lincoln: Finding the Genetic Cause of Abraham Lincoln's Height, Homeliness, Pseudo-Depression, and Imminent Cancer Death. Mount Vernon, VA: Mt. Vernon Book Systems.
- Scientist Wants to Test Abraham Lincoln's Bloodstained Pillow for Cancer Discover Magazine 20 April 2009
- Lincoln's Shroud of Turin, Philadelphila Inquirer, 13 April 2009