Necrotizing enterocolitis
Necrotizing enterocolitis (NEC) is a devastating intestinal disease that affects premature or very low birth weight infants.[4][1] Symptoms may include poor feeding, bloating, decreased activity, blood in the stool, vomiting of bile, bowel death, multiorgan failure, and even death.[1][2]
| Necrotizing enterocolitis | |
|---|---|
| Specialty | Pediatrics, gastroenterology, neonatology |
| Symptoms | Poor feeding, bloating, decreased activity, vomiting of bile[1] |
| Complications | Short-gut syndrome, intestinal strictures, developmental delay[2] |
| Causes | Unclear[1] |
| Risk factors | Preterm birth, congenital heart disease, birth asphyxia, exchange transfusion, prolonged rupture of membranes[1] |
| Differential diagnosis | Sepsis, anal fissure, infectious enterocolitis, Hirschsprung disease[2][3] |
| Prevention | Breast milk, probiotics.[2] |
| Treatment | Bowel rest, nasogastric tube, antibiotics, surgery[2] |
| Prognosis | Risk of death 25%[1] |
The exact cause is unclear.[1] However, several risk factors have been identified. Consistently described risk factors include formula feeding, intestinal dysbiosis, low birth weight, and prematurity.[5] Maternal factors such as chorioamnionitis, cocaine abuse, in utero growth restriction, intrahepatic cholestasis during pregnancy, increased body mass index, lack of prenatal steroids, mode of delivery, placental abruption, preeclampsia, and smoking have not been consistently implicated with the development of NEC.[6][7][8][9][10] Other risk factors potentially implicated include congenital heart disease, birth asphyxia, exchange transfusion, and prelabor rupture of membranes.[1] The underlying mechanism is believed to involve a combination of poor blood flow and infection of the intestines.[2] Diagnosis is based on symptoms and confirmed with medical imaging.[1]
Prevention includes the use of breast milk and probiotics.[2] Treatment includes bowel rest, orogastric tube, intravenous fluids, and intravenous antibiotics.[2] Surgery is required in those who have free air in the abdomen.[2] A number of other supportive measures may also be required.[2] Complications may include short-gut syndrome, intestinal strictures, or developmental delay.[2]
About 7% of those who are born prematurely develop NEC; however the odds of an infant developing this illness is directly related to the intensive care unit they are placed in.[11][12][13][4][2] Onset is typically in the first four weeks of life.[2] Among those affected, about 25% die.[1] The sexes are affected with equal frequency.[14] The condition was first described between 1888 and 1891.[14]
Signs and symptoms
The condition is typically seen in premature infants, and the timing of its onset is generally inversely proportional to the gestational age of the baby at birth (i.e., the earlier a baby is born, the later signs of NEC are typically seen).[15]
Initial symptoms include feeding intolerance and failure to thrive, increased gastric residuals, abdominal distension, and bloody stools. Symptoms may progress rapidly to abdominal discoloration with intestinal perforation and peritonitis and systemic hypotension requiring intensive medical support.[16]
Cause
The exact cause is unclear.[1] Several risk factors have been implicated:[17]
Maternal factors
- Acid-suppressing medications
- Chorioamnionitis
- Cocaine abuse
- In utero growth restriction
- Increased body mass index
- Intrahepatic cholestasis during pregnancy
- Lack of prenatal steroids
- Mode of delivery
- Placental abruption
- Pre-eclampsia
- Smoking
Main risk factors
- Low birth weight
- Prematurity
- Formula feeding (bovine based)
- Intestinal dysbiosis
Other risk factors
- Acute hypoxia
- Antibiotic exposure
- Blood transfusions
- Cardiac anomalies
- Neonatal anemia
- Poor intestinal perfusion
- Prolonged use of indomethacin for patent ductus arteriosus closure
Diagnosis

Diagnosis is usually suspected clinically, but often requires the aid of diagnostic imaging, most commonly radiography, which can show the intestines and may show areas with death tissue or a bowel perforation.[18] Specific radiographic signs of NEC are associated with specific Bell's stages of the disease:[19]
- Bell's stage 1 (suspected disease):
- Mild systemic disease (apnea, lethargy,[20] slowed heart rate, temperature instability)
- Mild intestinal signs (abdominal distention, increased gastric residuals, bloody stools)
- Nonspecific or normal radiological signs
- Bell's stage 2 (definite disease):
- Mild to moderate systemic signs
- Additional intestinal signs (absent bowel sounds, abdominal tenderness)
- Specific radiologic signs (pneumatosis intestinalis or portal venous gas)
- Laboratory changes (metabolic acidosis, too few platelets in the bloodstream)
- Bell's stage 3 (advanced disease):
- Severe systemic illness (low blood pressure)
- Additional intestinal signs (striking abdominal distention, peritonitis)
- Severe radiologic signs (pneumoperitoneum)
- Additional laboratory changes (metabolic and respiratory acidosis, disseminated intravascular coagulation)
Ultrasonography has proven to be useful, as it may detect signs and complications of NEC before they are evident on radiographs, specifically in cases that involve a paucity of bowel gas, a gasless abdomen, or a sentinel loop.[21] Diagnosis is ultimately made in 5–10% of very-low-birth-weight infants (<1,500g).[22]
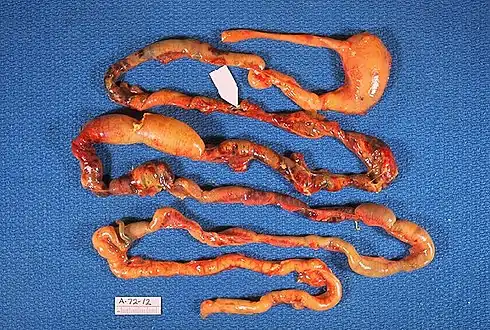 Alimentary tract of infant showing intestinal necrosis, pneumatosis intestinalis, and perforation site (arrow) (autopsy)
Alimentary tract of infant showing intestinal necrosis, pneumatosis intestinalis, and perforation site (arrow) (autopsy) Close-up of intestine of infant showing necrosis and pneumatosis intestinalis (autopsy)
Close-up of intestine of infant showing necrosis and pneumatosis intestinalis (autopsy)
Diagnosis of NEC is more challenging in premature infants, due to inexplicit symptoms and radiographic signs. The most preterm infant is at highest risk of developing NEC.[23]
Prevention
Prevention includes the use of breast milk and probiotics.[2] A 2012 policy by the American Academy of Pediatrics recommended feeding preterm infants human milk, finding "significant short- and long-term beneficial effects," including reducing the rate of NEC by a factor of one-half to three-quarters.[24]
Small amounts of oral feeds of human milk starting as soon as possible, while the infant is being primarily fed intravenously, primes the immature gut to mature and become ready to receive greater intake by mouth.[25] Human milk from a milk bank or donor can be used if mother's milk is unavailable. The gut mucosal cells do not get enough nourishment from arterial blood supply to stay healthy, especially in very premature infants, where the blood supply is limited due to immature development of the capillaries, so nutrients from the lumen of the gut are needed.
Towards understanding intervention with human milk, experts have noted cow's and human milk differ in their immunoglobular and glycan compositions.[26][27] Due to their relative ease of production, human milk oligosaccharides (HMO) are a subject of particular interest in supplementation and intervention.[28]
A Cochrane review in 2020 (updated in 2023) found low- to moderate-quality evidence that supplementation of probiotics enterally "prevents severe NEC, as well as all-cause mortality in preterm infants" but cautioned that the evidence was not sufficient to inform policy and practice and that further high-quality trials are needed.[29]
Advancing enteral feed volumes at lower rates does not appear to reduce the risk of NEC or death in very preterm infants and seems to increase the risk of invasive infection.[30] Not beginning feeding an infant by mouth for more than 4 days does not appear to have protective benefits.[31]
Treatment
If a baby is diagnosed with NEC, treatment should begin immediately.[18] Treatment consists primarily of supportive care, including providing bowel rest by stopping enteral feeds, gastric decompression with intermittent suction, fluid repletion to correct electrolyte abnormalities and third-space losses, support for blood pressure, parenteral nutrition,[32] and prompt antibiotic therapy.
Monitoring is clinical, although serial supine and left lateral decubitus abdominal X-rays should be performed every six hours.[33]
As an infant recovers from NEC, feeds are gradually introduced. "Trophic feeds" or low-volume feeds (<20 ml/kg/day) are usually initiated first. How and what to feed are determined by the extent of bowel involved, the need for surgical intervention, and the infant's clinical appearance.[34]
Where the disease is not halted through medical treatment alone, or when the bowel perforates, immediate emergency surgery to resect the dead bowel is generally required, although abdominal drains may be placed in very unstable infants as a temporizing measure. Surgery may require a colostomy, which may be able to be reversed at a later time. Some children may develop short bowel syndrome if extensive portions of the bowel must be removed.
In the case of an infant whose bowel is left in discontinuity, the surgical creation of a mucous fistula or connection to the distal bowel may be helpful, as this allows for refeeding of ostomy output to the distal bowel. This refeeding process is believed to improve bowel adaptation and aid in advancement of feeds.[34]
Prognosis
Typical recovery from NEC if medical, nonsurgical treatment succeeds, includes 10–14 days or more without oral intake, and then demonstrated ability to resume feedings and gain weight. Recovery from NEC alone may be compromised by co-morbid conditions that frequently accompany prematurity. Long-term complications of medical NEC include bowel obstruction and anemia.
In the United States, NEC caused 355 deaths per 100,000 live births in 2013, down from 484 per 100,000 live births in 2009. Rates of death were almost three times higher for the black population than for the white population.[35]
When NEC is diagnosed and treated immediately, the prognosis for babies is generally very good. Most babies recover fully without any additional health problems.[18] Overall, about 70-80% of infants who develop NEC survive.[36] Medical management of NEC shows an increased chance of survival compared to surgical management.[36] Despite a significant mortality risk, long-term prognosis for infants undergoing NEC surgery is improving, with survival rates of 70–80%. However, "Surgical NEC" survivors are still at risk for possible long-term complications, such as narrowing of the intestines[18] or short bowel syndrome and neurodevelopmental disability.
References
- "Necrotizing Enterocolitis – Pediatrics – Merck Manuals Professional Edition". Merck Manuals Professional Edition. February 2017. Retrieved 12 December 2017.
- Rich BS, Dolgin SE (December 2017). "Necrotizing Enterocolitis". Pediatrics in Review. 38 (12): 552–559. doi:10.1542/pir.2017-0002. PMID 29196510. S2CID 39251333.
- Crocetti M, Barone MA, Oski FA (2004). Oski's Essential Pediatrics. Lippincott Williams & Wilkins. p. 59. ISBN 9780781737708.
- Gephart S.M., Quinn M. A call to action to fight for equity and end necrotizing enterocolitis disparities. Adv. Neonatal Care. 2021;21(5):333-335. doi:10.1097/ANC.0000000000000940
- Rose AT, Patel RM (December 2018). "A critical analysis of risk factors for necrotizing enterocolitis". Seminars in Fetal & Neonatal Medicine. 23 (6): 374–379. doi:10.1016/j.siny.2018.07.005. PMC 6269219. PMID 30115546.
- Travers CP, Clark RH, Spitzer AR, Das A, Garite TJ, Carlo WA (March 2017). "Exposure to any antenatal corticosteroids and outcomes in preterm infants by gestational age: prospective cohort study". BMJ. 356: j1039. doi:10.1136/bmj.j1039. PMC 5373674. PMID 28351838.
- Been JV, Lievense S, Zimmermann LJ, Kramer BW, Wolfs TG (February 2013). "Chorioamnionitis as a risk factor for necrotizing enterocolitis: a systematic review and meta-analysis". The Journal of Pediatrics. 162 (2): 236–42.e2. doi:10.1016/j.jpeds.2012.07.012. PMID 22920508.
- Lu Q, Cheng S, Zhou M, Yu J (April 2017). "Risk Factors for Necrotizing Enterocolitis in Neonates: A Retrospective Case-Control Study". Pediatrics and Neonatology. 58 (2): 165–170. doi:10.1016/j.pedneo.2016.04.002. PMID 27543379.
- Czyrko C, Del Pin CA, O'Neill JA, Peckham GJ, Ross AJ (April 1991). "Maternal cocaine abuse and necrotizing enterocolitis: outcome and survival". Journal of Pediatric Surgery. 26 (4): 414–8, discussion 419–21. doi:10.1016/0022-3468(91)90988-6. PMID 2056401.
- Downard CD, Grant SN, Maki AC, Krupski MC, Matheson PJ, Bendon RW, et al. (July 2012). "Maternal cigarette smoking and the development of necrotizing enterocolitis". Pediatrics. 130 (1): 78–82. doi:10.1542/peds.2011-3808. PMID 22689867. S2CID 17281723.
- Gephart SM, Spitzer AR, Effken JA, Dodd E, Halpern M, McGrath JM. Discrimination of GutCheckNEC: a clinical risk index for necrotizing enterocolitis. J Perinatol. 2014;34(6):468-475.
- Horbar JD, Edwards EM, Greenberg LT, et al. Variation in performance of neona-tal intensive care units in the United States. JAMA Pediatr. 2017;171(3):e164396.
- Uauy RD, Fanaroff AA, Korones SB, Phillips EA, Phillips JB, Wright LL. Necrotizing enterocolitis in very low birth weight infants: biodemographic and clinical corre-lates. National Institute of Child Health and Human Development Neonatal Research Network. J Pediatr. 1991;119(4):630-638.
- Panigrahi P (2006). "Necrotizing enterocolitis: a practical guide to its prevention and management". Paediatric Drugs. 8 (3): 151–165. doi:10.2165/00148581-200608030-00002. PMID 16774295. S2CID 29437889.
- Yee WH, Soraisham AS, Shah VS, Aziz K, Yoon W, Lee SK (February 2012). "Incidence and timing of presentation of necrotizing enterocolitis in preterm infants". Pediatrics. 129 (2): e298–e304. doi:10.1542/peds.2011-2022. PMID 22271701. S2CID 26079047.
- "Necrotizing Enterocolitis". The Lecturio Medical Concept Library. Retrieved 11 August 2021.
- Alganabi M, Lee C, Bindi E, Li B, Pierro A (2019). "Recent advances in understanding necrotizing enterocolitis". F1000Research. 8: 107. doi:10.12688/f1000research.17228.1. PMC 6348433. PMID 30740215.
- Cline M (2021-07-14). "Necrotizing Enterocolitis: A Guide for Preemie Parents". Birth Injury Guide. Retrieved 2021-08-19.
- Lin PW, Stoll BJ (October 2006). "Necrotising enterocolitis". Lancet. 368 (9543): 1271–83. doi:10.1016/S0140-6736(06)69525-1. PMID 17027734. S2CID 37235496.
- Schanler RJ, Abrams SA, Kim MS (2016). "Clinical features and diagnosis of necrotizing enterocolitis in newborns". UpToDate.
- Muchantef K, Epelman M, Darge K, Kirpalani H, Laje P, Anupindi SA. Sonographic and radiographic imaging features of the neonate with necrotizing enterocolitis: correlating findings with outcomes. Pediatr Radiol. 2013 Jun 15.
- Marino BS, Fine KS (1 December 2008). Blueprints Pediatrics. Lippincott Williams & Wilkins. ISBN 978-0-7817-8251-7.
- Palleri E, Aghamn I, Bexelius TS, Bartocci M, Wester T (September 2018). "The effect of gestational age on clinical and radiological presentation of necrotizing enterocolitis". Journal of Pediatric Surgery. 53 (9): 1660–1664. doi:10.1016/j.jpedsurg.2017.09.018. PMID 29079313. S2CID 38176277.
- American Academy of Pediatrics, Section on Breastfeeding (March 2012). "Breastfeeding and the use of human milk". Pediatrics. 129 (3): e827–e841. doi:10.1542/peds.2011-3552. PMID 22371471.
Meta-analyses of four randomized clinical trials performed over the period 1983 to 2005 support the conclusion that feeding preterm infants human milk is associated with a significant reduction (58%) in the incidence of NEC. A more recent study of preterm infants fed an exclusive human milk diet compared with those fed human milk supplemented with cow's milk-based infant formula products noted a 77% reduction in NEC.
- Ziegler EE, Carlson SJ (March 2009). "Early nutrition of very low birth weight infants". The Journal of Maternal-Fetal & Neonatal Medicine. 22 (3): 191–197. doi:10.1080/14767050802630169. PMID 19330702. S2CID 36737314.
- Bode L (September 2012). "Human milk oligosaccharides: every baby needs a sugar mama". Glycobiology. 22 (9): 1147–1162. doi:10.1093/glycob/cws074. PMC 3406618. PMID 22513036.
- Boix-Amorós A, Collado MC, Van't Land B, Calvert A, Le Doare K, Garssen J, et al. (May 2019). "Reviewing the evidence on breast milk composition and immunological outcomes". Nutrition Reviews. 77 (8): 541–556. doi:10.1093/nutrit/nuz019. PMID 31111150.
- Bode L, Contractor N, Barile D, Pohl N, Prudden AR, Boons GJ, et al. (October 2016). "Overcoming the limited availability of human milk oligosaccharides: challenges and opportunities for research and application". Nutrition Reviews. 74 (10): 635–644. doi:10.1093/nutrit/nuw025. PMC 6281035. PMID 27634978.
- Sharif S, Meader N, Oddie SJ, Rojas-Reyes MX, McGuire W (July 2023). "Probiotics to prevent necrotising enterocolitis in very preterm or very low birth weight infants". The Cochrane Database of Systematic Reviews. 2023 (7): CD005496. doi:10.1002/14651858.CD005496.pub6. PMC 10370900. PMID 37493095.
- Oddie SJ, Young L, McGuire W (August 2021). "Slow advancement of enteral feed volumes to prevent necrotising enterocolitis in very low birth weight infants". The Cochrane Database of Systematic Reviews. 2021 (8): CD001241. doi:10.1002/14651858.CD001241.pub8. PMC 8407506. PMID 34427330.
- Young L, Oddie SJ, McGuire W (January 2022). "Delayed introduction of progressive enteral feeds to prevent necrotising enterocolitis in very low birth weight infants". The Cochrane Database of Systematic Reviews. 1 (1): CD001970. doi:10.1002/14651858.CD001970.pub6. PMC 8771918. PMID 35049036.
- Heird WC, Gomez MR (June 1994). "Total parenteral nutrition in necrotizing enterocolitis". Clinics in Perinatology. 21 (2): 389–409. doi:10.1016/s0095-5108(18)30352-x. PMID 8070233.
- Neu J, Walker WA (January 2011). "Necrotizing enterocolitis". The New England Journal of Medicine. 364 (3): 255–264. doi:10.1056/NEJMra1005408. PMC 3628622. PMID 21247316.
- Christian VJ, Polzin E, Welak S (August 2018). "Nutrition Management of Necrotizing Enterocolitis". Nutrition in Clinical Practice. 33 (4): 476–482. doi:10.1002/ncp.10115. PMID 29940075. S2CID 49419886.
- Xu J, Murphy SL, Kochanek KD, Bastian BA (February 2016). "Deaths: Final Data for 2013" (PDF). National Vital Statistics Reports. 64 (2): 1–119. PMID 26905861.
- Schanler RJ, Abrams SA, Kim MS. Management of necrotizing enterocolitis in newborns. UpToDate (Report).