Small for gestational age
Small for gestational age (SGA) newborns are those who are smaller in size than normal for the gestational age. SGA is most commonly defined as a weight below the 10th percentile for the gestational age.[1] SGA predicts susceptibility to hypoglycemia, hypothermia, and polycythemia.[2] By definition, at least 10% of all newborns will be labeled SGA. All SGA babies should be watched for signs of failure to thrive, hypoglycemia and other health conditions.
| Small for gestational age | |
|---|---|
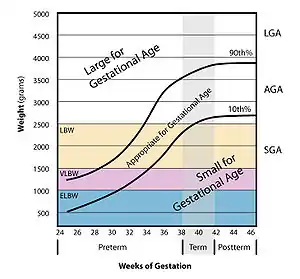 | |
| Graph showing which babies fit the definition of small. (DiseaseDB #31952) | |
| Specialty | Pediatrics |
Causes
Being small for gestational age is broadly either:[3]
- Being constitutionally small, or caused by a genetic trait of the baby
- Intrauterine growth restriction, also called "pathological SGA"
Diagnosis
The condition is defined by birth weight and/or length.
Intrauterine growth restriction is generally diagnosed by measuring the mother's uterus, with the fundal height being less than it should be for that stage of the pregnancy. If it is suspected, the mother will usually be sent for an ultrasound to confirm.
Management
Ninety percent of babies born SGA catch up in growth by the time they reach 2 years old. For the 10 percent of those that are SGA without catchup growth by 2 years old, an endocrinologist should be consulted. Some cases warrant growth hormone therapy.
Hypoglycemia is common in asymmetrical SGA babies because their larger brains burn calories at a faster rate than their usually limited fat stores hold . Hypoglycemia is treated by frequent feedings and/or additions of cornstarch-based products (such as Duocal powder) to the feedings.
There are some common conditions and disorders found in many that are SGA (and especially those that are SGA without catchup growth by 2 years old).
- Gastroenterologist - for gastrointestinal issues such as reflux and/or delayed gastric emptying
- Dietitian - to address caloric deficits. Dietitians are usually brought in for cases that include failure to thrive. According to the theory of thrifty phenotype, causes of growth restriction also trigger epigenetic responses in the fetus that are otherwise activated in times of chronic food shortage, and if the offspring develops in an environment rich in food, it may be more prone to metabolic disorders such as obesity and type II diabetes.[4]
- Speech-language pathologist or occupational therapist - Occupational therapists may also treat sensory issues
- Behaviorist - for feeding issues, a behavioral approach may also be used, but usually for older children (over 2)
- Allergist - to diagnose or rule out food allergies (not necessarily more common in those SGA than the normal population)
- Ear, nose and throat doctor - to diagnose enlarged adenoids or tonsils (not necessarily more common in those SGA than the normal population)
For intrauterine growth restriction (during pregnancy), possible treatments include the early induction of labor, though this is only done if the condition has been diagnosed and seen as a risk to the health of the fetus.
Terminology
If small for gestational age babies have been the subject of intrauterine growth restriction, formerly known as intrauterine growth retardation,[5] the term "SGA associated with intrauterine growth restriction" is used. Intrauterine growth restriction refers to a condition in which a fetus is unable to achieve its genetically determined potential size. This functional definition seeks to identify a population of fetuses at risk for modifiable but otherwise poor outcomes. This definition intentionally excludes fetuses that are small for gestational age (SGA) but are not pathologically small.[3] Infants born SGA with severe short stature (or severe SGA) are defined as having a length less than 2.5 standard deviation scores below the mean.[6]
A related term is low birth weight, defined as an infant with a birth weight (that is, mass at the time of birth[7]) of less than 2500 g (5 lb 8 oz), regardless of gestational age at the time of birth. Other related terms include "very low birth weight", which is less than 1500 g, and "extremely low birth weight", which is less than 1000 g.[8] Normal Weight at term delivery is 2500 g - 4200 g.
SGA is not a synonym of low birth weight, very low birth weight, or extremely low birth weight. Example: 35-week gestational age delivery, 2250 g weight is appropriate for gestational age but is still low birth weight. One third of low-birth-weight neonates - infants weighing less than 2500 g - are small for gestational age.
There is an 8.1% incidence of low birth weight in developed countries, and 6–30% in developing countries. Much of this can be attributed to the health of the mother during pregnancy. One third of babies born with a low birth weight are also small for gestational age. Infants that are born at low birth weights are at risk of developing neonatal infection.
Both low and high maternal serum Vitamin D (25-OH) are associated with higher incidence SGA in white women, although the correlation does not seem to hold for African American women.[9]
| Gestational Age at birth (weeks) | Mean weight (grams) | SD | 10th% |
|---|---|---|---|
| 22 | 467 | 92 | 354 |
| 23 | 553 | 109 | 416 |
| 24 | 626 | 129 | 473 |
| 25 | 714 | 156 | 529 |
| 26 | 819 | 186 | 597 |
| 27 | 935 | 215 | 677 |
| 28 | 1073 | 242 | 770 |
| 29 | 1211 | 269 | 882 |
| 30 | 1396 | 309 | 1018 |
| 31 | 1588 | 336 | 1166 |
| 32 | 1800 | 371 | 1335 |
| 33 | 2033 | 405 | 1538 |
| 34 | 2296 | 428 | 1772 |
| 35 | 2560 | 440 | 2021 |
| 36 | 2799 | 441 | 2261 |
| 37 | 3028 | 456 | 2477 |
| 38 | 3209 | 432 | 2665 |
| 39 | 3333 | 419 | 2810 |
| 40 | 3417 | 416 | 2904 |
| 41 | 3486 | 422 | 2958 |
| 42 | 3512 | 429 | 2985 |
| 43 | 3550 | 444 | 2981 |
| 44 | 3505 | 503 | 2952 |
References
- Small for gestational age (SGA) at MedlinePlus. Update Date: 8/4/2009. Updated by: Linda J. Vorvick. Also reviewed by David Zieve.
- Cunningham, F. Gary; Leveno, Kenneth J.; Bloom, Steven L.; Spong, Catherine Y.; Dashe, Jodi S.; Hoffman, Barbara L.; Casey, Brian M.; Sheffield, Jeanne S. (2013). Williams Obstetrics (24 ed.). New York, NY: McGraw-Hill Education.
- Ross, Michael G. "eMedicine - Fetal Growth Restriction". Retrieved 2010-02-25.
- Barker, D. J. P., ed. (1992). Fetal and infant origins of adult disease. London: British Medical Journal. ISBN 0-7279-0743-3.
- Dogra, Vikram S. "eMedicine - Intrauterine Growth Retardation". Retrieved 2007-11-28.
- Clayton, PE; Cianfarani, S; Czernichow, P; Johannsson, G; Rapaport, R; Rogol, A (March 2007). "Management of the child born small for gestational age through to adulthood: a consensus statement of the International Societies of Pediatric Endocrinology and the Growth Hormone Research Society". The Journal of Clinical Endocrinology and Metabolism. 92 (3): 804–10. doi:10.1210/jc.2006-2017. hdl:2108/45969. PMID 17200164.
- Definitions Archived 2012-04-02 at the Wayback Machine from Georgia Department of Public Health. Date: 12/04/2008. Original citation: "Birthweight: Infant's weight recorded at the time of birth"
- Subramanian, KN Siva. "eMedicine - Extremely Low Birth Weight Infant". Retrieved 2007-11-28.
- Bodnar, LM; Catov, JM; Zmuda, JM; Cooper, ME; Parrott, MS; Roberts, JM; Marazita, ML; Simhan, HN (May 2010). "Maternal serum 25-hydroxyvitamin D concentrations are associated with small-for-gestational age births in white women". Journal of Nutrition. 140 (5): 999–1006. doi:10.3945/jn.109.119636. PMC 2855265. PMID 20200114.
- Talge, Nicole M.; Mudd, Lanay M.; Sikorskii, Alla; Basso, Olga (2014-05-01). "United States Birth Weight Reference Corrected For Implausible Gestational Age Estimates". Pediatrics. 133 (5): 844–853. doi:10.1542/peds.2013-3285. ISSN 0031-4005. PMID 24777216. S2CID 5895957.