Dysmenorrhea
Dysmenorrhea, also known as period pain, painful periods or menstrual cramps, is pain during menstruation.[4][5][2] Its usual onset occurs around the time that menstruation begins.[1] Symptoms typically last less than three days.[1] The pain is usually in the pelvis or lower abdomen.[1] Other symptoms may include back pain, diarrhea or nausea.[1]
| Dysmenorrhea | |
|---|---|
| Other names | Dysmenorrhoea, period pain, painful periods, menstrual cramps |
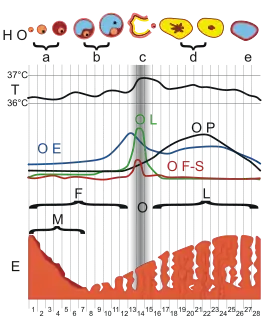 | |
| Menstrual cycle and changes in hormone production | |
| Specialty | Gynecology |
| Symptoms | Pain during first few days of menstruation, diarrhea, nausea[1][2] |
| Usual onset | Within a year of the first menstrual period[1] |
| Duration | Less than 5 days (primary dysmenorrhea)[1] |
| Causes | No underlying problem, uterine fibroids, adenomyosis, endometriosis[3] |
| Diagnostic method | Pelvic exam, ultrasound[1] |
| Differential diagnosis | Ectopic pregnancy, pelvic inflammatory disease, interstitial cystitis, chronic pelvic pain[1] |
| Treatment | Heating pad, medication[3] |
| Medication | NSAIDs such as ibuprofen, hormonal birth control, IUD with progestogen[1][3] |
| Prognosis | Often improves with age[2] |
| Frequency | 50–90% female adolescents and women of reproductive age[4] |
Dysmenorrhea can occur without an underlying problem.[3][6] Underlying issues that can cause dysmenorrhea include uterine fibroids, adenomyosis, and most commonly, endometriosis.[3] It is more common among those with heavy periods, irregular periods, those whose periods started before twelve years of age and those who have a low body weight.[1] A pelvic exam and ultrasound in individuals who are sexually active may be useful for diagnosis.[1] Conditions that should be ruled out include ectopic pregnancy, pelvic inflammatory disease, interstitial cystitis and chronic pelvic pain.[1]
Dysmenorrhea occurs less often in those who exercise regularly and those who have children early in life.[1] Treatment may include the use of a heating pad.[3] Medications that may help include NSAIDs such as ibuprofen, hormonal birth control and the IUD with progestogen.[1][3] Taking vitamin B1 or magnesium may help.[2] Evidence for yoga, acupuncture and massage is insufficient.[1] Surgery may be useful if certain underlying problems are present.[2]
Estimates of the percentage of female adolescents, and women of reproductive age affected are between 50% and 90%.[4][6] It is the most common menstrual disorder.[2] Typically, it starts within a year of the first menstrual period.[1] When there is no underlying cause, often the pain improves with age or following having a child.[2]
Signs and symptoms
The main symptom of dysmenorrhea is pain concentrated in the lower abdomen or pelvis.[1] It is also commonly felt in the right or left side of the abdomen. It may radiate to the thighs and lower back.[1]
Symptoms often co-occurring with menstrual pain include nausea and vomiting, diarrhea, headache, dizziness, disorientation, fainting and fatigue.[7] Symptoms of dysmenorrhea often begin immediately after ovulation and can last until the end of menstruation. This is because dysmenorrhea is often associated with changes in hormonal levels in the body that occur with ovulation. In particular, prostaglandins induce abdominal contractions that can cause pain and gastrointestinal symptoms.[8][9] The use of certain types of birth control pills can prevent the symptoms of dysmenorrhea because they stop ovulation from occurring.
Dysmenorrhea is associated with increased pain sensitivity and heavy menstrual bleeding.[10][11]
For many women, primary dysmenorrhea gradually subsides in late second generation. Pregnancy has also been demonstrated to lessen the severity of dysmenorrhea, when menstruation resumes. However, dysmenorrhea can continue until menopause. 5–15% of women with dysmenorrhea experience symptoms severe enough to interfere with daily activities.[12]
Causes
There are two types of dysmenorrhea, primary and secondary, based on the absence or presence of an underlying cause. Primary dysmenorrhea occurs without an associated underlying condition, while secondary dysmenorrhea has a specific underlying cause, typically a condition that affects the uterus or other reproductive organs.[5]
Painful menstrual cramps can result from an excess of prostaglandins released from the uterus. Prostaglandins cause the uterine muscles to tighten and relax causing the menstrual cramps. This type of dysmenorrhea is called primary dysmenorrhea.[5] Primary dysmenorrhea usually begins in the teens soon after the first period.[13]
Secondary dysmenorrhea is the type of dysmenorrhea caused by another condition such as endometriosis, uterine fibroids,[5] uterine adenomyosis, and polycystic ovary syndrome. Rarely, birth defects, intrauterine devices, certain cancers, and pelvic infections cause secondary dysmenorrhea.[12] If the pain occurs between menstrual periods, lasts longer than the first few days of the period, or is not adequately relieved by the use of nonsteroidal anti-inflammatory drugs (NSAIDs) or hormonal contraceptives, this could indicate another condition causing secondary dysmenorrhea.[14]
Membranous dysmenorrhea is a type of secondary dysmenorrhea in which the entire lining of the uterus is shed all at once rather than over the course of several days as is typical.[15] Signs and symptoms include spotting, bleeding, abdominal pain, and menstrual cramps. The resulting uterine tissue is called a decidual cast and must be passed through the cervix and vagina.[16] It typically takes the shape of the uterus itself. Membranous dysmenorrhea is extremely rare and there are very few reported cases. The underlying cause is unknown, though some evidence suggests it may be associated with ectopic pregnancy or the use of hormonal contraception.
When laparoscopy is used for diagnosis, the most common cause of dysmenorrhea is endometriosis, in approximately 70% of adolescents.[17]
Other causes of secondary dysmenorrhea include leiomyoma,[18] adenomyosis,[19] ovarian cysts, pelvic congestion,[20] and cavitated and accessory uterine mass.[21]
Risk factors
Genetic factors, stress and depression are risk factors for dysmenorrhea.[22] Risk factors for primary dysmenorrhea include: early age at menarche, long or heavy menstrual periods, smoking, and a family history of dysmenorrhea.[12]
Dysmenorrhea is a highly polygenic and heritable condition.[23] There is strong evidence of familial predisposition and genetic factors increasing susceptibility to dysmenorrhea. There have been multiple polymorphisms and genetic variants in both metabolic genes and genes responsible for immunity which have been associated with the disorder.[24]
Three distinct possible phenotypes have been identified for dysmenorrhea which include "multiple severe symptoms", "mild localized pain", and "severe localized pain". While there are likely differences in genotypes underlying each phenotype, the specific correlating genotypes have not yet been identified. These phenotypes are prevalent at different levels in different population demographics, suggesting different allelic frequencies across populations (in terms of race, ethnicity, and nationality).[25]
Polymorphisms in the ESR1 gene have been commonly associated with severe dysmenorrhea.[23] Variant genotypes in the metabolic genes such as CYP2D6 and GSTM1 have been similarly been correlated with an increased risk of severe menstrual pain, but not with moderate or occasional phentoypes.[26]
The occurrence and frequency of secondary dysmenorrhea (SD) has been associated with different alleles and genotypes of those with underlying pathologies, which can affect the pelvic region or other areas of the body. Individuals with disorders may have genetic mutations related to their diagnoses which produce dysmenorrhea as a symptom of their primary diagnosis. It has been found that those with fibromyalgia who have the ESR1 gene variation Xbal and possess the Xbal AA genotype are more susceptible to experiencing mild to severe menstrual pain resulting from their primary pathology.[27] Commonly, genetic mutations which are a hallmark of or associated with specific disorders can produce dysmenorrhea as a symptom which accompanies the primary disorder.
In contrast with secondary dysmenorrhea, primary dysmenorrhea (PD) has no underlying pathology.[28] Genetic mutation and variations have therefore been thought to underlie this disorder and contribute to the pathogenesis of PD.[29] There are multiple single-nucleotide polymorphisms (SNP) associated with PD. Two of the most well studied include an SNP in the promoter of MIF and an SNP in the tumor necrosis factor (TNF-α) gene. When a cytosine 173 base pairs upstream of macrophage migration inhibitory factor (MIF) promoter was replaced by a guanine there was an associated increase in the likelihood of the individual experiencing PD. While a CC/GG genotype led to an increase in likelihood of the individual experiencing severe menstrual pain, a CC/GC genotype led to a more significant likelihood of the disorder impacting the individual overall and increasing the likelihood of any of the three phenotypes.[30] A second associated SNP was located 308 base pairs upstream from the start codon of the TNF-α gene, in which guanine was substituted for adenine. A GG genotype at the loci is associated with the disorder and has been proposed as a possible genetic marker to predict PD.[30]
There has also been an association with mutations in the MEFV gene and dysmenorrhea, which are considered to be causative.[31] The phenotypes associated with these mutations in the MEFV genes have been better studied; individuals who are heterozygous for these mutations are more likely to be affected by PD which presents as a severe pain phenotype.[23]
Genes related to immunity have been identified as playing a significant role in PD as well. IL1A was found to be the gene most associated with primary dysmenorrhea in terms of its phenotypic impact.[23] This gene encodes a protein essential for the regulation of immunity and inflammation.15 While the mechanism of how it influences PD has yet to be discovered, it is assumed that possible mutations in IL1A or genes which interact with it impact the regulation of inflammation during menstruation. These mutations may therefore affect pain responses during menstruation which lead to the differing phenotypes associated with dysmenorrhea.
Two additionally well studied SNPs which are suspected to contribute to PD were found in ZM1Z1 (the mutant allele called rs76518691) and NGF (the mutant allele called rs7523831). Both ZMIZ1 and NGF are associated with autoimmune responses and diseases, as well as pain response.[23] The implication of these genes impacting Dysmenorrhea is significant as it suggests mutations which affect the immune system (specifically the inflammatory response) and pain response may also be a cause of primary dysmenorrhea.
Mechanism
The underlying mechanism of primary dysmenorrhea is the contractions of the muscles of the uterus which induce a local ischemia.[32]
During an individual's menstrual cycle, the endometrium thickens in preparation for potential pregnancy. After ovulation, if the ovum is not fertilized and there is no pregnancy, the built-up uterine tissue is not needed and thus shed.
Prostaglandins and leukotrienes are released during menstruation, due to the build up of omega-6 fatty acids.[33][34] Release of prostaglandins and other inflammatory mediators in the uterus cause the uterus to contract and can result in systemic symptoms such as nausea, vomiting, bloating and headaches or migraines.[33] Prostaglandins are thought to be a major factor in primary dysmenorrhea.[35] When the uterine muscles contract, they constrict the blood supply to the tissue of the endometrium, which, in turn, breaks down and dies. These uterine contractions continue as they squeeze the old, dead endometrial tissue through the cervix and out of the body through the vagina. These contractions, and the resulting temporary oxygen deprivation to nearby tissues, are thought to be responsible for the pain or cramps experienced during menstruation.
Compared with non-dysmnenorrhic individuals, those with primary dysmenorrhea have increased activity of the uterine muscle with increased contractility and increased frequency of contractions.[36]
Diagnosis
The diagnosis of dysmenorrhea is usually made simply on a medical history of menstrual pain that interferes with daily activities. However, there is no universally accepted standard technique for quantifying the severity of menstrual pains.[37] There are various quantification models, called menstrual symptometrics, that can be used to estimate the severity of menstrual pains as well as correlate them with pain in other parts of the body, menstrual bleeding and degree of interference with daily activities.[37]
Further work-up
Once a diagnosis of dysmenorrhea is made, further workup is required to search for any secondary underlying cause of it, in order to be able to treat it specifically and to avoid the aggravation of a perhaps serious underlying cause.
Further work-up includes a specific medical history of symptoms and menstrual cycles and a pelvic examination.[6] Based on results from these, additional exams and tests may be motivated, such as:
Management
Treatments that target the mechanism of pain include non-steroidal anti-inflammatory drugs (NSAIDs) and hormonal contraceptives. NSAIDs inhibit prostaglandin production. With long-term treatment, hormonal birth control reduces the amount of uterine fluid/tissue expelled from the uterus. Thus resulting in shorter, less painful menstruation.[38] These drugs are typically more effective than treatments that do not target the source of the pain (e.g. acetaminophen).[39] Regular physical activity may limit the severity of uterine cramps.[12][40]
NSAIDs
Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen are effective in relieving the pain of primary dysmenorrhea.[41] They can have side effects of nausea, dyspepsia, peptic ulcer, and diarrhea.[42][41]
Hormonal birth control
Use of hormonal birth control may improve symptoms of primary dysmenorrhea.[43][33] A 2009 systematic review (updated in 2023) found evidence that the low or medium doses of estrogen contained in the birth control pill reduces pain associated with dysmenorrhea.[44] In addition, no differences between different birth control pill preparations were found.[44] The review did not determine if the estrogen in birth control pills was more effective than NSAIDs.[44]
Norplant[45] and Depo-provera[46][47] are also effective, since these methods often induce amenorrhea. The intrauterine system (Mirena IUD) may be useful in reducing symptoms.[48]
Other
A review indicated the effectiveness of transdermal nitroglycerin.[49] Reviews indicated magnesium supplementation seemed to be effective.[50][2] A review indicated the usefulness of using calcium channel blockers.[32] Heat is effective compared to NSAIDs and is a preferred option by many patients, as it is easy to access and has no known side effects.[51]
Tamoxifen has been used effectively to reduce uterine contractility and pain in dysmenorrhea patients.[52]
There is some evidence that exercises performed 3 times a week for about 45 to 60 minutes, without particular intensity, reduces menstrual pain.[53]
Alternative medicine
There is insufficient evidence to recommend the use of many herbal or dietary supplements for treating dysmenorrhea, including melatonin, vitamin E, fennel, dill, chamomile, cinnamon, damask rose, rhubarb, guava, and uzara.[1][54] Further research is recommended to follow up on weak evidence of benefit for: fenugreek, ginger, valerian, zataria, zinc sulphate, fish oil, and vitamin B1. A 2016 review found that evidence of safety is insufficient for most dietary supplements.[54] There is some evidence for the use of fenugreek.[55]
One review found thiamine and vitamin E to be likely effective.[56] It found the effects of fish oil and vitamin B12 to be unknown.[56] Reviews found tentative evidence that ginger powder may be effective for primary dysmenorrhea.[57] Reviews have found promising evidence for Chinese herbal medicine for primary dysmenorrhea, but that the evidence was limited by its poor methodological quality.[58][59]
A 2016 Cochrane review of acupuncture for dysmenorrhea concluded that it is unknown if acupuncture or acupressure is effective.[60] There were also concerns of bias in study design and in publication, insufficient reporting (few looked at adverse effects), and that they were inconsistent.[60] There are conflicting reports in the literature, including one review which found that acupressure, topical heat, and behavioral interventions are likely effective.[56] It found the effect of acupuncture and magnets to be unknown.[56]
A 2007 systematic review found some scientific evidence that behavioral interventions may be effective, but that the results should be viewed with caution due to poor quality of the data.[61]
Spinal manipulation does not appear to be helpful.[56] Although claims have been made for chiropractic care, under the theory that treating subluxations in the spine may decrease symptoms,[62] a 2006 systematic review found that overall no evidence suggests that spinal manipulation is effective for treatment of primary and secondary dysmenorrhea.[63]
Valerian, Humulus lupulus and Passiflora incarnata may be safe and effective in the treatment of dysmenorrhea.[10]
TENS
A 2011 review stated that high-frequency transcutaneous electrical nerve stimulation may reduce pain compared with sham TENS, but seems to be less effective than ibuprofen.[56]
Surgery
One treatment of last resort is presacral neurectomy.[64]
Epidemiology
Dysmenorrhea is one of the most common gynecological problems, regardless of age or race. It is one of the most frequently identified causes of pelvic pain in those who menstruate. Dysmenorrhea is estimated to affect between 50% and 90% of female adolescents and women of reproductive age.[4] Another report states that estimates can vary between 16% and 91% of surveyed individuals, with severe pain observed in 2% to 29% of menstruating individuals.[51] Reports of dysmenorrhea are greatest among individuals in their late teens and 20s, with reports usually declining with age. The prevalence in adolescent females has been reported to be 67.2% by one study[65] and 90% by another.[66] It has been stated that there is no significant difference in prevalence or incidence between races,[66] although one study of Hispanic adolescent females indicated an elevated prevalence and impact in this group.[67] Another study indicated that dysmenorrhea was present in 36.4% of participants, and was significantly associated with lower age and lower parity.[68] Childbearing is said to relieve dysmenorrhea, but this does not always occur. One study indicated that in nulliparous individuals with primary dysmenorrhea, the severity of menstrual pain decreased significantly after age 40.[69]
A survey in Norway showed that 14 percent of females between the ages of 20 to 35 experience symptoms so severe that they stay home from school or work.[70] Among adolescent girls, dysmenorrhea is the leading cause of recurrent short-term school absence.[71]
References
- Osayande AS, Mehulic S (March 2014). "Diagnosis and initial management of dysmenorrhea". American Family Physician. 89 (5): 341–346. PMID 24695505.
- American College of Obstetricians and Gynecologists (Jan 2015). "FAQ046 Dynsmenorrhea: Painful Periods" (PDF). Archived (PDF) from the original on 27 June 2015. Retrieved 26 June 2015.
- "Menstruation and the menstrual cycle fact sheet". Office of Women's Health. December 23, 2014. Archived from the original on 26 June 2015. Retrieved 25 June 2015.
- McKenna KA, Fogleman CD (August 2021). "Dysmenorrhea". Am Fam Physician. 104 (2): 164–170. PMID 34383437.
- "Period Pain". MedlinePlus. National Library of Medicine. March 1, 2018. Retrieved November 7, 2018.
- "Dysmenorrhea and Endometriosis in the Adolescent". ACOG. American College of Obstetricians and Gynecologists. 20 November 2018. Retrieved 21 November 2018.
- "Dysmenorrhea". www.hopkinsmedicine.org. 13 May 2019. Retrieved 2019-10-04.
- "Period pain". nhs.uk. 2017-10-19. Retrieved 2019-10-04.
- "Using Foods Against Menstrual Pain". Physicians Committee for Responsible Medicine. Retrieved 2019-10-04.
- Gomathy N, Dhanasekar KR, Trayambak D, Amirtha R (November 2019). "Supportive therapy for dysmenorrhea: Time to look beyond mefenamic acid in primary care". Journal of Family Medicine and Primary Care. 8 (11): 3487–3491. doi:10.4103/jfmpc.jfmpc_717_19. PMC 6881953. PMID 31803641.
- Payne LA, Rapkin AJ, Seidman LC, Zeltzer LK, Tsao JC (2017). "Experimental and procedural pain responses in primary dysmenorrhea: a systematic review". Journal of Pain Research. 10: 2233–2246. doi:10.2147/JPR.S143512. PMC 5604431. PMID 29066929.
- "Dysmenorrhea - Gynecology and Obstetrics". Merck Manuals Professional Edition. Archived from the original on 10 September 2017.
- "Period problems | Office on Women's Health". www.womenshealth.gov. Retrieved 14 November 2022.
- Carlson KJ, Eisenstat SA, Ziporyn TD (2004). The New Harvard Guide to Women's Health. Harvard University Press. p. 479. doi:10.2307/j.ctv1b9f66x. ISBN 978-0-674-01282-0. JSTOR j.ctv1b9f66x.
- "How to manage a decidual cast, aka shedding your entire uterus lining in one go". 3 November 2020.
- "What is a Decidual Cast?".
- Janssen EB, Rijkers AC, Hoppenbrouwers K, Meuleman C, D'Hooghe TM (2013). "Prevalence of endometriosis diagnosed by laparoscopy in adolescents with dysmenorrhea or chronic pelvic pain: a systematic review". Human Reproduction Update. 19 (5): 570–582. doi:10.1093/humupd/dmt016. PMID 23727940.
- Hilário SG, Bozzini N, Borsari R, Baracat EC (January 2009). "Action of aromatase inhibitor for treatment of uterine leiomyoma in perimenopausal patients". Fertility and Sterility. 91 (1): 240–243. doi:10.1016/j.fertnstert.2007.11.006. PMID 18249392.
- Nabeshima H, Murakami T, Nishimoto M, Sugawara N, Sato N (2008). "Successful total laparoscopic cystic adenomyomectomy after unsuccessful open surgery using transtrocar ultrasonographic guiding". Journal of Minimally Invasive Gynecology. 15 (2): 227–230. doi:10.1016/j.jmig.2007.10.007. PMID 18312998.
- Hacker, Neville F., J. George Moore, and Joseph C. Gambone. Essentials of Obstetrics and Gynecology, 4th ed. Elsevier Saunders, 2004. ISBN 0-7216-0179-0
- Acién P, Acién M, Fernández F, José Mayol M, Aranda I (November 2010). "The cavitated accessory uterine mass: a Müllerian anomaly in women with an otherwise normal uterus". Obstetrics and Gynecology. 116 (5): 1101–1109. doi:10.1097/AOG.0b013e3181f7e735. PMID 20966695. S2CID 20532705.
- Ju H, Jones M, Mishra G (2014). "The prevalence and risk factors of dysmenorrhea". Epidemiologic Reviews. 36: 104–113. doi:10.1093/epirev/mxt009. PMID 24284871.
- Li Z, Chen J, Zhao Y, Wang Y, Xu J, Ji J, et al. (April 2017). "Common variants in ZMIZ1 and near NGF confer risk for primary dysmenorrhoea". Nature Communications. 8 (1): 14900. Bibcode:2017NatCo...814900L. doi:10.1038/ncomms14900. PMC 5414039. PMID 28447608.
- Ju H, Jones M, Mishra G (2014-01-01). "The prevalence and risk factors of dysmenorrhea". Epidemiologic Reviews. 36 (1): 104–113. doi:10.1093/epirev/mxt009. PMID 24284871.
- Chen CX, Carpenter JS, Ofner S, LaPradd M, Fortenberry JD (January 2021). "Dysmenorrhea Symptom-Based Phenotypes: A Replication and Extension Study". Nursing Research. 70 (1): 24–33. doi:10.1097/NNR.0000000000000477. PMC 7736149. PMID 32956256.
- Wu D, Wang X, Chen D, Niu T, Ni J, Liu X, Xu X (November 2000). "Metabolic gene polymorphisms and risk of dysmenorrhea". Epidemiology. 11 (6): 648–653. doi:10.1097/00001648-200011000-00006. PMID 11055624. S2CID 27774699.
- Arslan HS, Nursal AF, Inanir A, Karakus N, Yigit S (2021-08-26). "Influence of ESR1 Variants on Clinical Characteristics and Fibromyalgia Syndrome in Turkish Women". Endocrine, Metabolic & Immune Disorders Drug Targets. 21 (7): 1326–1332. doi:10.2174/1871530320666200910110915. PMID 32914729. S2CID 221623106.
- Osayande AS, Mehulic S (March 2014). "Diagnosis and initial management of dysmenorrhea". American Family Physician. 89 (5): 341–346. PMID 24695505.
- Osonuga A, Ekor M (December 2019). "Risk factors for dysmenorrhea among Ghanaian undergraduate students". African Health Sciences. 19 (4): 2993–3000. doi:10.4314/ahs.v19i4.20. PMC 7040311. PMID 32127874.
- Dogru HY, Ozsoy AZ, Karakus N, Delibas IB, Isguder CK, Yigit S (August 2016). "Association of Genetic Polymorphisms in TNF and MIF Gene with the Risk of Primary Dysmenorrhea". Biochemical Genetics. 54 (4): 457–466. doi:10.1007/s10528-016-9732-2. PMID 27105877. S2CID 86975436.
- Erten S, Altunoglu A, Keskin HL, Ceylan GG, Yazıcı A, Dalgaci AF, et al. (September 2013). "Increased frequency of MEFV gene mutations in patients with primary dysmenorrhea". Modern Rheumatology. 23 (5): 959–962. doi:10.3109/s10165-012-0779-6. PMID 23053724. S2CID 75848809.
- Fenakel K, Lurie S (December 1990). "The use of calcium channel blockers in obstetrics and gynecology; a review". European Journal of Obstetrics, Gynecology, and Reproductive Biology. 37 (3): 199–203. doi:10.1016/0028-2243(90)90025-v. PMID 2227064.
- Harel Z (December 2006). "Dysmenorrhea in adolescents and young adults: etiology and management". Journal of Pediatric and Adolescent Gynecology. 19 (6): 363–371. doi:10.1016/j.jpag.2006.09.001. PMID 17174824.
- Bofill Rodriguez M, Lethaby A, Farquhar C (September 2019). "Non-steroidal anti-inflammatory drugs for heavy menstrual bleeding". The Cochrane Database of Systematic Reviews. 2019 (9): CD000400. doi:10.1002/14651858.CD000400.pub4. PMC 6751587. PMID 31535715.
- Wright, Jason and Solange Wyatt. The Washington Manual Obstetrics and Gynecology Survival Guide. Lippincott Williams and Wilkins, 2003. ISBN 0-7817-4363-X
- Rosenwaks Z, Seegar-Jones G (October 1980). "Menstrual pain: its origin and pathogenesis". The Journal of Reproductive Medicine. 25 (4 Suppl): 207–212. PMID 7001019.
- Wyatt KM, Dimmock PW, Hayes-Gill B, Crowe J, O'Brien PM (July 2002). "Menstrual symptometrics: a simple computer-aided method to quantify menstrual cycle disorders". Fertility and Sterility. 78 (1): 96–101. doi:10.1016/s0015-0282(02)03161-8. PMID 12095497.
- Miller L, Notter KM (November 2001). "Menstrual reduction with extended use of combination oral contraceptive pills: randomized controlled trial". Obstetrics and Gynecology. LWW Journals. 98 (5 Pt 1): 771–778. doi:10.1016/s0029-7844(01)01555-1. PMID 11704167. S2CID 23668483.
- Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M (July 2015). "Nonsteroidal anti-inflammatory drugs for dysmenorrhoea". The Cochrane Database of Systematic Reviews. 2015 (7): CD001751. doi:10.1002/14651858.CD001751.pub3. PMC 6953236. PMID 26224322.
- Armour M, Ee CC, Naidoo D, Ayati Z, Chalmers KJ, Steel KA, et al. (September 2019). "Exercise for dysmenorrhoea". The Cochrane Database of Systematic Reviews. 2019 (9): CD004142. doi:10.1002/14651858.CD004142.pub4. PMC 6753056. PMID 31538328.
- Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M (July 2015). "Nonsteroidal anti-inflammatory drugs for dysmenorrhoea". The Cochrane Database of Systematic Reviews. 2015 (7): CD001751. doi:10.1002/14651858.CD001751.pub3. PMC 6953236. PMID 26224322.
- Rossi S, editor. Australian Medicines Handbook 2006. Adelaide: Australian Medicines Handbook; 2006. ISBN 0-9757919-2-3
- Archer DF (November 2006). "Menstrual-cycle-related symptoms: a review of the rationale for continuous use of oral contraceptives". Contraception. 74 (5): 359–366. doi:10.1016/j.contraception.2006.06.003. PMID 17046376.
- Schroll JB, Black AY, Farquhar C, Chen I (July 2023). "Combined oral contraceptive pill for primary dysmenorrhoea". The Cochrane Database of Systematic Reviews. 2023 (7): CD002120. doi:10.1002/14651858.CD002120.pub4. PMC 10388393. PMID 37523477.
- Power J, French R, Cowan F (July 2007). Power J (ed.). "Subdermal implantable contraceptives versus other forms of reversible contraceptives or other implants as effective methods of preventing pregnancy". The Cochrane Database of Systematic Reviews. 2007 (3): CD001326. doi:10.1002/14651858.CD001326.pub2. PMC 7025801. PMID 17636668.
- Glasier A (2006). "Contraception". In DeGroot LJ, Larry JJ (eds.). Endocrinology (5th ed.). Philadelphia: Elsevier Saunders. pp. 2993–3003. ISBN 978-0-7216-0376-6.
- Loose DS, Stancel GM (2006). "Estrogens and Progestins". In Brunton LL, Lazo JS, Parker KL (eds.). Goodman & Gilman's The Pharmacological Basis of Therapeutics (11th ed.). New York: McGraw-Hill. pp. 1541–1571. ISBN 978-0-07-142280-2.
- Gupta HP, Singh U, Sinha S (July 2007). "Laevonorgestrel intra-uterine system--a revolutionary intra-uterine device". Journal of the Indian Medical Association. 105 (7): 380, 382–380, 385. PMID 18178990.
- Morgan PJ, Kung R, Tarshis J (May 2002). "Nitroglycerin as a uterine relaxant: a systematic review". Journal of Obstetrics and Gynaecology Canada. 24 (5): 403–409. doi:10.1016/S1701-2163(16)30403-0. PMID 12196860.
- Parazzini F, Di Martino M, Pellegrino P (February 2017). "Magnesium in the gynecological practice: a literature review". Magnesium Research. 30 (1): 1–7. doi:10.1684/mrh.2017.0419. PMID 28392498.
- Nagy, H.; Khan MAB (2020). "Dysmenorrhea". StatPearls. PMID 32809669.
 Text was copied from this source, which is available under a Creative Commons Attribution 4.0 International License.
Text was copied from this source, which is available under a Creative Commons Attribution 4.0 International License. - Thomas B, Magos A (2009). "Modern management of dysmenorrhoea". Trends in Urology, Gynaecology & Sexual Health. 14 (5): 25–29. doi:10.1002/tre.120.
- Armour M, Ee CC, Naidoo D, Ayati Z, Chalmers KJ, Steel KA, et al. (September 2019). "Exercise for dysmenorrhoea". The Cochrane Database of Systematic Reviews. 2019 (9): CD004142. doi:10.1002/14651858.CD004142.pub4. PMC 6753056. PMID 31538328.
- Pattanittum P, Kunyanone N, Brown J, Sangkomkamhang US, Barnes J, Seyfoddin V, Marjoribanks J (March 2016). "Dietary supplements for dysmenorrhoea". The Cochrane Database of Systematic Reviews. 2016 (3): CD002124. doi:10.1002/14651858.CD002124.pub2. PMC 7387104. PMID 27000311.
- Nagulapalli Venkata KC, Swaroop A, Bagchi D, Bishayee A (June 2017). "A small plant with big benefits: Fenugreek (Trigonella foenum-graecum Linn.) for disease prevention and health promotion". Molecular Nutrition & Food Research. 61 (6): 1600950. doi:10.1002/mnfr.201600950. PMID 28266134. S2CID 23539394.
- Latthe PM, Champaneria R, Khan KS (February 2011). "Dysmenorrhoea". BMJ Clinical Evidence. 2011. PMC 3275141. PMID 21718556.
- Daily JW, Zhang X, Kim DS, Park S (December 2015). "Efficacy of Ginger for Alleviating the Symptoms of Primary Dysmenorrhea: A Systematic Review and Meta-analysis of Randomized Clinical Trials". Pain Medicine. 16 (12): 2243–2255. doi:10.1111/pme.12853. PMID 26177393.
- Zhu X, Proctor M, Bensoussan A, Wu E, Smith CA (April 2008). Zhu X (ed.). "Chinese herbal medicine for primary dysmenorrhoea". The Cochrane Database of Systematic Reviews (2): CD005288. doi:10.1002/14651858.CD005288.pub3. PMID 18425916.
- Gao L, Jia C, Zhang H, Ma C (October 2017). "Wenjing decoction (herbal medicine) for the treatment of primary dysmenorrhea: a systematic review and meta-analysis". Archives of Gynecology and Obstetrics. 296 (4): 679–689. doi:10.1007/s00404-017-4485-7. PMID 28791471. S2CID 32573698.
- Smith CA, Armour M, Zhu X, Li X, Lu ZY, Song J (April 2016). "Acupuncture for dysmenorrhoea". The Cochrane Database of Systematic Reviews. 2016 (4): CD007854. doi:10.1002/14651858.CD007854.pub3. PMC 8406933. PMID 27087494.
- Proctor ML, Murphy PA, Pattison HM, Suckling J, Farquhar CM (July 2007). Proctor M (ed.). "Behavioural interventions for primary and secondary dysmenorrhoea". The Cochrane Database of Systematic Reviews. 2007 (3): CD002248. doi:10.1002/14651858.CD002248.pub3. PMC 7137212. PMID 17636702.
- Chapman-Smith D (2000). "Scope of practice". The Chiropractic Profession: Its Education, Practice, Research and Future Directions. West Des Moines, IA: NCMIC. ISBN 978-1-892734-02-0.
- Proctor ML, Hing W, Johnson TC, Murphy PA (July 2006). Proctor M (ed.). "Spinal manipulation for primary and secondary dysmenorrhoea". The Cochrane Database of Systematic Reviews. 3 (3): CD002119. doi:10.1002/14651858.CD002119.pub3. PMC 6718213. PMID 16855988.
- Ramirez C, Donnellan N (August 2017). "Pelvic denervation procedures for dysmenorrhea". Current Opinion in Obstetrics & Gynecology. 29 (4): 225–230. doi:10.1097/GCO.0000000000000379. PMID 28683027. S2CID 205607600.
- Sharma P, Malhotra C, Taneja DK, Saha R (February 2008). "Problems related to menstruation amongst adolescent girls". Indian Journal of Pediatrics. 75 (2): 125–129. doi:10.1007/s12098-008-0018-5. PMID 18334791. S2CID 58327516.
- Holder A, Edmundson LD, Mert E (31 December 2009). "Dysmenorrhea". eMedicine. Archived from the original on 2011-02-22.
- Banikarim C, Chacko MR, Kelder SH (December 2000). "Prevalence and impact of dysmenorrhea on Hispanic female adolescents". Archives of Pediatrics & Adolescent Medicine. 154 (12): 1226–1229. doi:10.1001/archpedi.154.12.1226. PMID 11115307.
- Sule ST, Umar HS, Madugu NH (June 2007). "Premenstrual symptoms and dysmenorrhoea among Muslim women in Zaria, Nigeria". Annals of African Medicine. 6 (2): 68–72. doi:10.4103/1596-3519.55713. PMID 18240706.
- Juang CM, Yen MS, Horng HC, Cheng CY, Yuan CC, Chang CM (October 2006). "Natural progression of menstrual pain in nulliparous women at reproductive age: an observational study". Journal of the Chinese Medical Association. 69 (10): 484–488. doi:10.1016/S1726-4901(09)70313-2. PMID 17098673. S2CID 24518670.
- "Mozon: Sykemelder seg på grunn av menssmerter". Mozon. 2004-10-25. Archived from the original on 2007-03-17. Retrieved 2007-02-02.
- French L (2008). "Dysmenorrhea in adolescents: diagnosis and treatment". Paediatric Drugs. 10 (1): 1–7. doi:10.2165/00148581-200810010-00001. PMID 18162003. S2CID 33563026.