Phobia
A phobia is an anxiety disorder, defined by a persistent and excessive fear of an object or situation.[1] Phobias typically result in a rapid onset of fear and are usually present for more than six months.[1] Those affected go to great lengths to avoid the situation or object, to a degree greater than the actual danger posed.[1] If the object or situation cannot be avoided, they experience significant distress.[1] Other symptoms can include fainting, which may occur in blood or injury phobia,[1] and panic attacks, often found in agoraphobia and emetophobia.[6] Around 75% of those with phobias have multiple phobias.[1]
| Phobia | |
|---|---|
 | |
| The fear of spiders is one of the most common phobias. | |
| Specialty | Psychiatry, clinical psychology |
| Symptoms | Fear of an object or situation[1] |
| Complications | Suicide, high risk of comorbidities[1] |
| Usual onset | Rapid[1] |
| Duration | More than six months[1] |
| Types | Specific phobias, social anxiety disorder, agoraphobia[1][2] |
| Causes | Genetic and environmental factors[3] |
| Treatment | Exposure therapy, counselling, medication[4][5][2] |
| Medication | Antidepressants, benzodiazepines, beta-blockers[4] |
| Frequency | Specific phobias: ~5%[1] Social phobia: ~5%[6] Agoraphobia: ~2%[6] |
Phobias can be divided into specific phobias, social anxiety disorder, and agoraphobia.[1][2] Specific phobias are further divided to include certain animals, natural environment, blood or injury, and particular situations.[1] The most common are fear of spiders, fear of snakes, and fear of heights.[7] Specific phobias may be caused by a negative experience with the object or situation in early childhood.[1] Social phobia is when a person fears a situation due to worries about others judging them.[1] Agoraphobia is a fear of a situation due to perceived difficulty or inability to escape.[1]
It is recommended that specific phobias be treated with exposure therapy, in which the person is introduced to the situation or object in question until the fear resolves.[2] Medications are not helpful for specific phobias.[2] Social phobia and agoraphobia may be treated with counseling, medications, or a combination of both.[4][5] Medications used include antidepressants, benzodiazepines, or beta-blockers.[4]
Specific phobias affect about 6–8% of people in the Western world and 2–4% in Asia, Africa, and Latin America in a given year.[1] Social phobia affects about 7% of people in the United States and 0.5–2.5% of people in the rest of the world.[6] Agoraphobia affects about 1.7% of people.[6] Women are affected by phobias about twice as often as men.[1][6] The typical onset of a phobia is around 10–17, and rates are lower with increasing age.[1][6] Those with phobias are more likely to attempt suicide.[1]
Classification
Fear is an emotional response to a current perceived danger. This differs from anxiety which is a response in preparation of a future threat. Fear and anxiety often can overlap but this distinction can help identify subtle differences between disorders, as well as differentiate between a response that would be expected given a person's developmental stage and culture.[1]
ICD-11
The International Classification of Diseases (11th version: ICD-11) is a globally used diagnostic tool for epidemiology, health management and clinical purposes maintained by the World Health Organization (WHO). The ICD classifies phobic disorders under the category of mental, behavioural or neurodevelopmental disorders. The ICD-10 differentiates between Phobic anxiety disorders, such as Agoraphobia, and Other anxiety disorders, such as Generalized anxiety disorder. The ICD-11 merges both groups together as Anxiety or fear-related disorders.[8]
DSM-5
Most phobias are classified into 3 categories. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), such phobias are considered subtypes of anxiety disorder. The categories are:
- Specific phobias: Fear of particular objects or situations that results in anxiety and avoidance. May lead to panic attacks if exposed to feared stimulus or in anticipation of encounter. A specific phobia may be further subdivided into five categories: animal, natural environment, situational, blood-injection-injury, and other.[1][9]
- Agoraphobia: a generalized fear of leaving home or a small familiar 'safe' area and of possible panic attacks that might follow. Various specific phobias may also cause it, such as fear of open spaces, social embarrassment (social agoraphobia), fear of contamination (fear of germs, possibly complicated by obsessive–compulsive disorder) or PTSD (post-traumatic stress disorder) related to a trauma that occurred outdoors.[1]
- Social anxiety disorder (SAD), also known as social phobia, is when the situation is feared out of a worrying about others judging them. Performance only is a subtype of social anxiety disorder[1]
Phobias vary in severity among individuals. Some individuals can avoid the subject and experience relatively mild anxiety over that fear. Others experience full-fledged panic attacks with all the associated impairing symptoms. Most individuals understand that their fear is irrational but cannot override their panic response. These individuals often report dizziness, loss of bladder or bowel control, tachypnea, feelings of pain, and shortness of breath.[10]
Causes
Phobias may develop for a variety of reasons. Childhood experiences, past traumatic experiences, brain chemistry, genetics, or learned behavior, can all be reasons why phobias develop. There are even phobias that may run in families and be passed down from one generation to another.[11]
There are multiple theories about how phobias develop and likely occur due to a combination of environmental and genetic factors. The degree to whether environment or genetic influences have a more significant role varies by condition, with social anxiety disorder and agoraphobia having around a 50% heritability rate.[12]
Environmental
Rachman proposed three pathways for the development of phobias: direct or classical conditioning (exposure to phobic stimulus), vicarious acquisition (seeing others experience phobic stimulus), and informational/instructional acquisition (learning about phobic stimulus from others).[13][14]
Classical conditioning
Much of the progress in understanding the acquisition of fear responses in phobias can be attributed to classical conditioning (Pavlovian model).[15] When an aversive stimulus and a neutral one are paired together, for instance, when an electric shock is given in a specific room, the subject can start to fear not only the shock but the room as well. In behavioral terms, the room is a conditioned stimulus (CS). When paired with an aversive unconditioned stimulus (UCS) (the shock), it creates a conditioned response (CR) (fear for the room) (CS+UCS=CR).[15] For example, in case of the fear of heights (acrophobia), the CS is heights. Such as a balcony on the top floors of a high rise building. The UCS can originate from an aversive or traumatizing event in the person's life, such as almost falling from a great height. The original fear of nearly falling is associated with being high, leading to a fear of heights. In other words, the CS (heights) associated with the aversive UCS (almost falling) leads to the CR (fear). Though historically influential in the theory of fear acquisition, this direct conditioning model is not the only proposed way to acquire a phobia. This theory in fact has limitations as not everyone that has experienced a traumatic event develops a phobia and vice versa.[14]
Vicarious conditioning
Vicarious fear acquisition is learning to fear something, not by a subject's own experience of fear, but by watching others, oftentimes a parent (observational learning). For instance, when a child sees a parent reacting fearfully to an animal, the child can also become afraid of the animal.[16] Through observational learning, humans can learn to fear potentially dangerous objects—a reaction observed in other primates.[17] A study on non-human primates, showed that the primates learned to fear snakes at a fast rate after watching parents' fearful reactions.[17] An increase in fearful behaviours was observed as the non-human primates observed their parents' fearful reactions.[17] Although observational learning has proven effective in creating reactions of fear and phobias, it has also been shown that by physically experiencing an event, increases the chance of fearful and phobic behaviours.[17] In some cases, physically experiencing an event may increase the fear and phobia more than observing a fearful reaction of another human or non-human primate.
Informational/Instructional acquisition
Informational/instructional fear acquisition is learning to fear something by getting information. For instance, fearing electrical wire after hearing that touching it causes an electric shock.[18]
A conditioned fear response to an object or situation is not always a phobia. There must also be symptoms of impairment and avoidance. Impairment is defined as an inability to complete routine tasks, whether occupational, academic, or social. For example, an occupational impairment can result from acrophobia, from not taking a job solely because of its location on the top floor of a building, or socially not participating in an event at a theme park. The avoidance aspect is defined as behaviour that results in the omission of an aversive event that would otherwise occur, intending to prevent anxiety.[19]
Genetic
With the completion of the Human Genome Project in 2003, much research has been completed looking at specific genes that may cause or contribute to medical conditions.[20] Candidate genes were the focus of most of these studies until the past decade, when the cost and ability to perform genome-wide analyses became more available. The GLRB gene was identified as a possible target for agoraphobia.[21] An area still in development is reviewing epigenetic components or the interaction of the environment on genes through methylation. A number of genes are being examined through this epigenetic lens which may be linked with social anxiety disorder, including MAOA, CRHR1, and OXTR.[12] Each phobia related disorder has some degree of genetic susceptibility. Those with specific phobias are more likely to have first degree relatives with the same specific phobia. Similarly, social anxiety disorder is found two to six times more frequently in those with first degree relatives that have it versus those that do not. Agoraphobia is believed to have the strongest genetic association.[6][12]
Mechanism
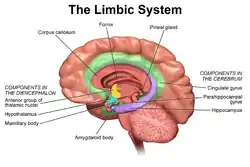
Limbic system
Beneath the lateral fissure in the cerebral cortex, the insula, or insular cortex, of the brain has been identified as part of the limbic system, along with the cingulated gyrus, hippocampus, corpus callosum, and other nearby cortices. This system has been found to play a role in emotion processing,[23] and the insula, in particular, may contribute to maintaining autonomic functions.[24] Studies by Critchley et al. indicate the insula as being involved in the experience of emotion by detecting and interpreting threatening stimuli.[25] Similar studies monitoring insula activity have shown a correlation between increased insular activation and anxiety.[23]
In the frontal lobes, other cortices involved with phobia and fear are the anterior cingulate cortex and the medial prefrontal cortex. In the processing of emotional stimuli, studies on phobic reactions to facial expressions have indicated that these areas are involved in the processing and responding to negative stimuli.[26] The ventromedial prefrontal cortex has been said to influence the amygdala by monitoring its reaction to emotional stimuli or even fearful memories.[23] Most specifically, the medial prefrontal cortex is active during the extinction of fear and is responsible for long-term extinction. Stimulation of this area decreases conditioned fear responses, so its role may be in inhibiting the amygdala and its reaction to fearful stimuli.[27]
The hippocampus is a horseshoe-shaped structure that plays an essential part in the brain's limbic system. This is because it forms memories and connects them with emotions and the senses. When dealing with fear, the hippocampus receives impulses from the amygdala that allow it to connect the fear with a certain sense, such as a smell or sound.
Amygdala
The amygdala is an almond-shaped mass of nuclei located deep in the brain's medial temporal lobe. It processes the events associated with fear and is linked to social phobia and other anxiety disorders. The amygdala's ability to respond to fearful stimuli occurs through fear conditioning. Like classical conditioning, the amygdala learns to associate a conditioned stimulus with a negative or avoidant stimulus, creating a conditioned fear response often seen in phobic individuals. The amygdala is responsible for recognizing certain stimuli or cues as dangerous and plays a role in the storage of threatening stimuli to memory. The basolateral nuclei (or basolateral amygdala) and the hippocampus interact with the amygdala in-memory storage. This connection suggests why memories are often remembered more vividly if they have emotional significance.[28]
In addition to memory, the amygdala also triggers the secretion of hormones that affect fear and aggression. When the fear or aggression response is initiated, the amygdala releases hormones into the body to put the human body into an "alert" state, which prepares the individual to move, run, fight, etc.[29] This defensive "alert" state and response are known as the fight-or-flight response.[30]
However, inside the brain, this stress response can be observed in the hypothalamic-pituitary-adrenal axis (HPA). This circuit incorporates the process of receiving stimuli, interpreting them, and releasing certain hormones into the bloodstream. The parvocellular neurosecretory neurons of the hypothalamus release corticotropin-releasing hormone (CRH), which is sent to the anterior pituitary. Here the pituitary releases adrenocorticotropic hormone (ACTH), which ultimately stimulates the release of cortisol. In relation to anxiety, the amygdala activates this circuit, while the hippocampus is responsible for suppressing it. Glucocorticoid receptors in the hippocampus monitor the amount of cortisol in the system and through negative feedback can tell the hypothalamus to stop releasing CRH.[24]
Studies on mice engineered to have high concentrations of CRH showed higher levels of anxiety, while those engineered to have no or low amounts of CRH receptors were less anxious. In people with phobias, therefore, high amounts of cortisol may be present, or there may be low levels of glucocorticoid receptors or even serotonin (5-HT).[24]
Disruption by damage
For the areas in the brain involved in emotion—most specifically fear— the processing and response to emotional stimuli can be altered when one of these regions is damaged. Damage to the cortical areas involved in the limbic system, such as the cingulate cortex or frontal lobes, has resulted in extreme emotion changes.[24] Other types of damage include Klüver–Bucy syndrome and Urbach–Wiethe disease. In Klüver–Bucy syndrome, a temporal lobectomy, or removal of the temporal lobes, results in changes involving fear and aggression. Specifically, the removal of these lobes results in decreased fear, confirming its role in fear recognition and response. Damage to both side (Bilateral damage) of the medial temporal lobes is known as Urbach–Wiethe disease. It presents with similar symptoms of decreased fear and aggression but with the addition of the inability to recognize emotional expressions, especially angry or fearful faces.[24]
The amygdala's role in learned fear includes interactions with other brain regions in the neural circuit of fear. While damage in the amygdala can inhibit its ability to recognize fearful stimuli, other areas such as the ventromedial prefrontal cortex and the basolateral nuclei of the amygdala can affect the region's ability to not only become conditioned to fearful stimuli but to extinguish them eventually. Through receiving stimulus info, the basolateral nuclei undergo synaptic changes that allow the amygdala to develop a conditioned response to fearful stimuli. Damage to this area, therefore, have been shown to disrupt the acquisition of learned responses to fear.[24] Likewise, damage in the ventromedial prefrontal cortex (the area responsible for monitoring the amygdala) has been shown to slow down the speed of extinguishing a learned fear response and how effective the extinction is. This suggests there is a pathway or circuit among the amygdala and nearby cortical areas that process emotional stimuli and influence emotional expression, all of which can be disrupted when damage occurs.[23]
Diagnosis
It is recommended that the terms distress and impairment take into account the context of the person's environment during diagnosis. The DSM-IV-TR states that if a feared stimulus, whether it be an object or a situation, is absent entirely in an environment, a diagnosis cannot be made. An example of this situation would be an individual who has a fear of mice but lives in an area without mice. Even though the concept of mice causes marked distress and impairment within the individual, because the individual does not usually encounter mice, no actual distress or impairment is ever experienced. It is recommended that proximity to, and ability to escape from, the stimulus also be considered. As the phobic person approaches a feared stimulus, anxiety levels increase, and the degree to which the person perceives they might escape from the stimulus affects the intensity of fear in instances such as riding an elevator (e.g. anxiety increases at the midway point between floors and decreases when the floor is reached and the doors open). The DSM-V has been updated to reflect that an individual may have changed their daily activities around the feared stimulus in such a way that they may avoid it altogether. The person may still meet criteria for the diagnosis if they continue to avoid or refuse to participate in activities they would involve possible exposure to the phobic stimulus.[1]
| Specific phobia | Social anxiety disorder | Agoraphobia | |
|---|---|---|---|
| Features | Fear out of proportion to the danger presented by an object or situation | Anxiety of social encounters due to potential scrutiny from others | Fear of leaving a protective place or situations viewed as being unable to escape from |
| Duration | ≥ 6 months | ≥ 6 months | ≥ 6 months |
Specific phobias
A specific phobia is a marked and persistent fear of an object or situation. Specific phobias may also include fear of losing control, panicking, and fainting from an encounter with the phobia.[1] Specific phobias are defined concerning objects or situations, whereas social phobias emphasize social fear and the evaluations that might accompany them.
The DSM breaks specific phobias into five subtypes: animal, natural environment, blood-injection-injury, situational and other.[1] In children, blood-injection-injury phobia, animal phobias, and natural environment phobias usually develop between the ages of 7 and 9 reflective of normal development. Additionally, specific phobias are most prevalent in children between the ages 10 and 13.[31] Situational phobias are typically found in older children and adults.[1]
Treatments
There are various methods used to treat phobias. These methods include systematic desensitization, progressive relaxation, virtual reality, modeling, medication, and hypnotherapy. Over the past several decades, psychologists and other researchers have developed effective behavioral, pharmacological, and technological interventions for the treatment of phobia.[32]
Virtual Reality treatments produce similar effects to in vivo exposure, another efficacious therapy great for treating phobias. Although Virtual Reality is great for treating phobias, the treatment will not work for every phobia. The treatment has positive effects, but depending on the phobia, in vivo would be another ideal treatment to use over Virtual Reality. In vivo exposure is a great way to reduce fear overtime and is actually more preferred when trying to treat anxiety and fear related problems.
Therapy
Cognitive Behavioral Therapy is an evidence-based treatment that can help with phobias. It is a talk therapy that can be used alone or along with other therapies. CBT is there to help manage stressful situations and respond better. This therapy requires the person to be honest with themselves and confront their feelings and phobias.[33]
Cognitive behavioral therapy (CBT) can be beneficial by allowing the person to challenge dysfunctional thoughts or beliefs by being mindful of their feelings to recognize that their fear is irrational. CBT may occur in a group setting. Gradual desensitization treatment and CBT are often successful, provided the person is willing to endure some discomfort.[34] In one clinical trial, 90% of people no longer had a phobic reaction after successful CBT treatment.[34][35][36][37] Research in the UK has suggested that for childhood phobias a single session of CBT can be effective.[38][39]
Evidence supports that eye movement desensitization and reprocessing (EMDR) is effective in treating some phobias.[40] Its effectiveness in treating complex or trauma-related phobias has not been empirically established.[41] Primarily used to treat post-traumatic stress disorder, EMDR has been demonstrated to ease phobia symptoms following a specific trauma, such as a fear of dogs following a dog bite.[42][43]
Systematic desensitization
.jpg.webp)
Systematic desensitization is a process in which people seeking help slowly become accustomed to their phobia, and ultimately overcome it. Traditional systematic desensitization involves a person being exposed to the object they are afraid of over time so that the fear and discomfort do not become overwhelming. This controlled exposure to the anxiety-provoking stimulus is key to the effectiveness of exposure therapy in the treatment of specific phobias. It has been shown that humor is an excellent alternative when traditional systematic desensitization is ineffective.[44] Humor systematic desensitization involves a series of treatment activities that elicit humor with the feared object.[44] Previously learned progressive muscle relaxation procedures can be used as the activities become more difficult. Progressive muscle relaxation helps people relax before and during exposure to the feared stimulus.
Virtual reality therapy is another technique that helps phobic people confront a feared object. It uses virtual reality to generate scenes that may not have been possible or ethical in the physical world. It is equally as effective as traditional exposure therapy[45] and offers additional advantages. These include controlling the scenes and having the phobic person endure more exposure than they might handle in reality.[46]
Medications
Medications are a treatment option often utilized in combination with CBT or if CBT was not tolerated or effective. Medications can help regulate apprehension and fear of a particular fearful object or situation. There are various medication options available for both social anxiety disorder and agoraphobia. The use of medications for specific phobias, besides the limited role of benzodiazepines, do not currently have established guidelines due to minimal supporting evidence.
Antidepressants
Antidepressant medications such as selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), or monoamine oxidase inhibitors (MAOIs) may be helpful in some cases. SSRIs / SNRIs act on serotonin, a neurotransmitter in the brain. Because of serotonins positive impacts mood, an antidepressant may be offered and prescribed as a treatment option. For social anxiety, the SSRIs sertraline, paroxetine, fluvoxamine, and the SNRI venlafaxine have FDA approval. Similar medications may be offered for agoraphobia.[47]
Benzodiazepines
Sedatives such as benzodiazepines (clonazepam, alprazolam) are another therapeutic option, which can help people relax by reducing the amount of anxiety they feel.[48] Benzodiazepines may be useful in the acute treatment of severe symptoms, but the risk-benefit ratio usually goes against their long-term use in phobic disorders.[49] This class of medication has recently been shown as effective if used with negative behaviours such as excessive alcohol use.[48] Despite this positive finding, benzodiazepines are used with caution due to side effects and risk of developing dependence or withdrawal symptoms. In specific phobia for example if the phobic stimulus is one that is not regularly encountered such as flying a short course may be provided.
Beta-blockers
Beta blockers (propranolol) are another therapeutic option, particularly for those with the performance only subtype of social anxiety disorder. They may stop the stimulating effects of adrenaline, such as sweating, increased heart rate, elevated blood pressure, tremors, and the feeling of a pounding heart.[48] By taking beta-blockers before a phobic event, these symptoms are decreased, making the event less frightening. Beta-blockers are not effective for generalized social anxiety disorder.[50]
Hypnotherapy
Hypnotherapy is another effective therapy that uses hypnosis to help manage anxiety and stress. This therapy can help people gain control over their phobias.[51]
Hypnotherapy can be used alone and in conjunction with systematic desensitization to treat phobias.[52] Through hypnotherapy, the underlying cause of the phobia may be uncovered. The phobia may be caused by a past event that the person does not remember, a phenomenon known as repression. The mind represses traumatic memories from the conscious mind until the person is ready to deal with them.
Hypnotherapy may also eliminate the conditioned responses that occur during different situations. People are first placed into a hypnotic trance, an extremely relaxed state[53] in which the unconscious can be retrieved. This state makes people more open to suggestion, which helps bring about desired change.[53] Consciously addressing old memories helps individuals understand the event and see it less threateningly.
Prognosis
Outcomes vary widely among the phobic anxiety disorders. There is a possibility that remission occurs without intervention but relapses are common. Response to treatment as well as remission and relapse rates are impacted by the severity of an individual's disorder as well as how long they have been experiencing symptoms. For example, in social anxiety disorder (social phobia) a majority of individuals will experience remission within the first couple of years of symptom onset without specific treatment. On the other hand, in Agoraphobia as few as 10% of individuals are seen to reach complete remission without treatment.[6] A study looking at the 2 year remission rates for anxiety disorders found that those with multiple anxieties were less likely to experience remission.[54]
Specific phobia
The majority of those that develop a specific phobia first experience symptoms in childhood. Often individuals will experience symptoms periodically with periods of remission before complete remission occurs. However, specific phobias that continue into adulthood are likely to experience a more chronic course. Specific phobias in older adults has been linked with a decrease in quality of life. Those with specific phobias are at an increased risk of suicide. Greater impairment is found in those that have multiple phobias.[1] Response to treatment is relatively high but many do not seek treatment due to lack of access, ability to avoid phobia, or unwilling to face feared object for repeated CBT sessions.[55]
Comorbidities
Many of those with a phobia often have more than one phobia. There are also a number of psychological and physiological disorders that tend to occur or coexist at higher rates among this population. As with all anxiety disorders the most common psychiatric condition to occur with a phobia is major depressive disorder.[12] Additionally bipolar disorder, substance dependence disorder, obsessive-compulsive disorder, and post traumatic stress disorder have also been found to occur in those with phobias at higher rates.
Epidemiology
Phobias are a common form of anxiety disorder, and distributions are heterogeneous by age and gender. An American study by the National Institute of Mental Health (NIMH) found that between 8.7 percent and 18.1 percent of Americans have phobias,[56] making it the most common mental illness among women in all age groups and the second most common illness among men older than 25. Between 4 percent and 10 percent of all children experience specific phobias during their lives,[31] and social phobias occur in one percent to three percent of children.[57][58][59]
A Swedish study found that females have a higher number of cases per year than males (26.5 percent for females and 12.4 percent for males).[60] Among adults, 21.2 percent of women and 10.9 percent of men have a single specific phobia, while multiple phobias occur in 5.4 percent of females and 1.5 percent of males.[60] Women are nearly four times as likely as men to have a fear of animals (12.1 percent in women and 3.3 percent in men) — a higher dimorphic than with all specific or generalized phobias or social phobias.[60] Social phobias are more common in girls than boys,[61] while situational phobia occurs in 17.4 percent of women and 8.5 percent of men.[60]
Society and culture
Terminology
The word phobia comes from the Greek: φόβος (phóbos), meaning "aversion", "fear" or "morbid fear". The regular system for naming specific phobias uses prefixes based on a Greek word for the object of the fear, plus the suffix -phobia. Benjamin Rush's 1786 satyrical text, 'On the different Species of Phobia', established the term's dictionary sense of specific morbid fears.[62] However, many phobias are irregularly named with Latin prefixes, such as apiphobia instead of melissaphobia (fear of bees) or aviphobia instead of ornithophobia (fear of birds). Creating these terms is something of a word game. Such fears are psychological rather than physiological in origin, and few of these terms are found in medical literature.[63] In ancient Greek mythology Phobos was the twin brother of Deimos (terror).
The word phobia may also refer to conditions other than true phobias. For example, the term hydrophobia is an old name for rabies, since an aversion to water is one of that disease's symptoms. A specific phobia to water is called aquaphobia instead. A hydrophobe is a chemical compound that repels water. Similarly, photophobia usually refers to a physical complaint (aversion to light due to inflamed eyes or excessively dilated pupils), rather than an irrational fear of light.
Non-medical, deterrent and political use
Several terms with the suffix -phobia are used non-clinically to imply irrational fear or hatred. Examples include:
- Chemophobia – Irrational fear or hatred of chemistry and synthetic chemicals.
- Xenophobia – Irrational fear or hatred of strangers or the unknown, sometimes used to describe nationalistic political beliefs and movements.
- Homophobia – Irrational fear or hatred of homosexuality or people who identify or perceived as being lesbian, gay, bisexual or transgender (LGBT).[64]
- Islamophobia – Irrational fear or hatred of Islam.
- Hinduphobia – Irrational fear or hatred for Hindus or Hinduism.
- Biphobia – Irrational fear or hatred of bisexual people.
- Transphobia – Irrational fear or hatred of transgender people.
- Christophobia – Irrational fear or hatred of Christianity or Jesus Christ.
Usually, these kinds of "phobias" are described as fear, dislike, disapproval, prejudice, hatred, discrimination, or hostility towards the object of the "phobia". It is a form of hyperbole.
Popular culture
A number of films and TV shows have portrayed individuals with a variety of phobic disorders.
Movies
- Benchwarmers – Howie Goodman (Nick Swardson) is portrayed as being agoraphobic and heliophobic.[65]
Television shows
- Monk – Adrian Monk (Tony Shalhoub) is a former homicide detective and a consultant for the San Francisco Police Department. He has an extreme case of OCD, and is well known for his various fears and phobias, including (but certainly not limited to) heights, snakes, crowds, glaciers, rodeos, wind, and milk.[66]
- Shameless (American TV series) – Sheila Jackson (Joan Cusack) has agoraphobia and mysophobia (fear of germs).[67]
Research directions
Before the development of pharmacotherapy, the treatment of phobias and mental health disorders relied solely on therapy such as CBT. Although therapy can be incredibly effective for many, it does not always achieve the desired effect. Interventional psychiatry is an additional branch in medicine that has expanded treatment options, and further research continues to explore effectiveness and applications. Electroconvulsive therapy (ECT) and transcranial magnetic stimulation (TMS) are two examples of device-based interventions widely utilized.[68][69] In terms of use in treating phobias and anxiety disorders as a whole, TMS is being explored as an augmentation option for those who do not have the desired response to other therapeutic options or side effects from medications. A majority of research has been conducted exploring the use of TMS in PTSD and generalized anxiety disorder. A meta‐analysis conducted in 2019 found only two clinical trials for the use of TMS in specific phobias, one of which explored anxiety and avoidance rates in individuals with acrophobia. Although the study found decreased rates in both anxiety and avoidance after two TMS sessions because of the limited number of studies and small sample size, few conclusions can be made.[70] D-cycloserine (DCS), a partial N-methyl-D-aspartate agonist, is an additional investigational approach to augmentation specific phobias that a meta-analysis suggested had better outcomes and less symptom severity when utilized before initiating CBT.[71]
See also
References
- American Psychiatric Association (2013), Diagnostic and Statistical Manual of Mental Disorders (5th ed.), Arlington: American Psychiatric Publishing, pp. 190, 197–202, ISBN 978-0890425558
- Hamm AO (September 2009). "Specific phobias". The Psychiatric Clinics of North America. 32 (3): 577–591. doi:10.1016/j.psc.2009.05.008. PMID 19716991. S2CID 5458941.
- Straight A's in Psychiatric and Mental Health Nursing. A Review Series. Lippincott Williams & Wilkins. 2006. p. 172. ISBN 9781582554488. OCLC 61247134.
- "Anxiety Disorders". NIMH. March 2016. Archived from the original on 27 July 2016. Retrieved 27 July 2016.
- Perugi G, Frare F, Toni C (2007). "Diagnosis and treatment of agoraphobia with panic disorder". CNS Drugs. 21 (9): 741–764. doi:10.2165/00023210-200721090-00004. PMID 17696574. S2CID 43437233.
- American Psychiatric Association (2013), Diagnostic and Statistical Manual of Mental Disorders (5th ed.), Arlington: American Psychiatric Publishing, pp. 204, 218–219, ISBN 978-0890425558
- "Specific Phobias". USVA. Archived from the original on 14 July 2016. Retrieved 26 July 2016.
- Reed GM, First MB, Kogan CS, Hyman SE, Gureje O, Gaebel W, et al. (February 2019). "Innovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disorders". World Psychiatry. 18 (1): 3–19. doi:10.1002/wps.20611. PMC 6313247. PMID 30600616.
- LeBeau RT, Glenn D, Liao B, Wittchen HU, Beesdo-Baum K, Ollendick T, Craske MG (February 2010). "Specific phobia: a review of DSM-IV specific phobia and preliminary recommendations for DSM-5". Depression and Anxiety. 27 (2): 148–167. CiteSeerX 10.1.1.590.6020. doi:10.1002/da.20655. PMID 20099272. S2CID 16835235.
- Tamparo C, Lewis M (2011). Diseases of the Human Body. Philadelphia, PA: F.A. Davis Company. pp. 153. ISBN 9780803625051.
- Garcia, René (2017-09-01). "Neurobiology of fear and specific phobias". Learning & Memory. 24 (9): 462–471. doi:10.1101/lm.044115.116. ISSN 1072-0502. PMC 5580526. PMID 28814472.
- Penninx BW, Pine DS, Holmes EA, Reif A (March 2021). "Anxiety disorders". Lancet. 397 (10277): 914–927. doi:10.1016/S0140-6736(21)00359-7. PMC 9248771. PMID 33581801. S2CID 231885253.
- Rachman SJ (1978). Fear and Courage. San Francisco: WH Freeman & Co.
- King NJ, Eleonora G, Ollendick TH (March 1998). "Etiology of childhood phobias: current status of Rachman's three pathways theory". Behaviour Research and Therapy. 36 (3): 297–309. doi:10.1016/S0005-7967(98)00015-1. PMID 9642849.
- Myers KM, Davis M (February 2007). "Mechanisms of fear extinction". Molecular Psychiatry. 12 (2): 120–150. doi:10.1038/sj.mp.4001939. PMID 17160066. S2CID 3364934. ProQuest 221163409.
- "vicarious conditioning". BehaveNet. Retrieved 2013-06-21.
- Mineka S, Davidson M, Cook M, Keir R (November 1984). "Observational conditioning of snake fear in rhesus monkeys". Journal of Abnormal Psychology. 93 (4): 355–372. doi:10.1037/0021-843x.93.4.355. PMID 6542574.
- Olsson A, Phelps EA (December 2004). "Learned fear of "unseen" faces after Pavlovian, observational, and instructed fear" (PDF). Psychological Science. 15 (12): 822–828. doi:10.1111/j.0956-7976.2004.00762.x. PMID 15563327. S2CID 13889777. Archived (PDF) from the original on 2013-11-09.
- Bolles RC (1970). "Species-specific Defense Reactions and Avoidance Learning". Psychological Review. 77: 32–38. doi:10.1037/h0028589.
- "Human Genome Project FAQ". Genome.gov. Retrieved 2022-03-11.
- Deckert J, Weber H, Villmann C, Lonsdorf TB, Richter J, Andreatta M, et al. (October 2017). "GLRB allelic variation associated with agoraphobic cognitions, increased startle response and fear network activation: a potential neurogenetic pathway to panic disorder". Molecular Psychiatry. 22 (10): 1431–1439. doi:10.1038/mp.2017.2. hdl:10023/11399. PMID 28167838. S2CID 10177012.
- "Post Traumatic Stress Disorder Research Fact Sheet". National Institutes of Health. Archived from the original on 2014-01-23.
- Tillfors M (2004). "Why do some individuals develop social phobia? A review with emphasis on the neurobiological influences". Nordic Journal of Psychiatry. 58 (4): 267–276. doi:10.1080/08039480410005774. PMID 15370775. S2CID 39942168.
- Bear MF, Connors BW, Paradiso MA, eds. (2007). Neuroscience: Exploring the Brain (3rd ed.). Lippincott Williams & Wilkins. ISBN 9780781760034.
- Straube T, Mentzel HJ, Miltner WH (2005). "Common and distinct brain activation to threat and safety signals in social phobia". Neuropsychobiology. 52 (3): 163–168. doi:10.1159/000087987. PMID 16137995. S2CID 7030421.
- Etkin A, Egner T, Kalisch R (February 2011). "Emotional processing in anterior cingulate and medial prefrontal cortex". Trends in Cognitive Sciences. 15 (2): 85–93. doi:10.1016/j.tics.2010.11.004. PMC 3035157. PMID 21167765.
- Akirav I, Maroun M (15 May 2006). "The role of the medial prefrontal cortex-amygdala circuit in stress effects on the extinction of fear". Neural Plasticity. 2007: 30873. doi:10.1155/2007/30873. PMC 1838961. PMID 17502909.
- Whalen PJ, Phelps EA, eds. (2009). The Human Amygdala. New York: The Guilford Press.
- Winerman L (August 2007). "Figuring Out Phobia". Monitor on Psychology. American Psychological Association. Archived from the original on 2007-10-05.
- Rogers K. "Fight-or-flight response". Britannica.com. Retrieved 19 February 2019.
- Bolton D, Eley TC, O'Connor TG, Perrin S, Rabe-Hesketh S, Rijsdijk F, Smith P (March 2006). "Prevalence and genetic and environmental influences on anxiety disorders in 6-year-old twins". Psychological Medicine. 36 (3): 335–344. doi:10.1017/S0033291705006537. PMID 16288680. S2CID 44579250.
- "Figuring out phobia". www.apa.org. Retrieved 2020-09-18.
- Paquette, Vincent; Lévesque, Johanne; Mensour, Boualem; Leroux, Jean-Maxime; Beaudoin, Gilles; Bourgouin, Pierre; Beauregard, Mario (2003-02-01). ""Change the mind and you change the brain": effects of cognitive-behavioral therapy on the neural correlates of spider phobia". NeuroImage. 18 (2): 401–409. doi:10.1016/S1053-8119(02)00030-7. ISSN 1053-8119. PMID 12595193. S2CID 10113900.
- Wolpe J (1958). "Psychotherapy by reciprocal inhibition". Conditional Reflex. 3 (4): 234–240. doi:10.1007/BF03000093. PMID 5712667. S2CID 46015274.
- Foa EB, Blau JS, Prout M, Latimer P (1977). "Is horror a necessary component of flooding (implosion)?". Behaviour Research and Therapy. 15 (5): 397–402. doi:10.1016/0005-7967(77)90043-2. PMID 612340.
- Craske M, Antony MM, Barlow DH (2006). Mastering your fears and phobias. US: Oxford University Press. ISBN 978-0-19-518917-9.
- Eysenck H (1977). You and Neurosis.
- Fischer K (2023-04-13). "CBT for phobias: one-session treatment is effective". NIHR Evidence. doi:10.3310/nihrevidence_57627. S2CID 258149486. Retrieved 2023-04-13.
- Wright B, Tindall L, Scott AJ, Lee E, Biggs K, Cooper C, et al. (October 2022). "One-session treatment compared with multisession CBT in children aged 7-16 years with specific phobias: the ASPECT non-inferiority RCT". Health Technology Assessment. 26 (42): 1–174. doi:10.3310/IBCT0609. PMC 9638885. PMID 36318050.
- Valiente-Gómez A, Moreno-Alcázar A, Treen D, Cedrón C, Colom F, Pérez V, Amann BL (2017-09-26). "EMDR beyond PTSD: A Systematic Literature Review". Frontiers in Psychology. 8: 1668. doi:10.3389/fpsyg.2017.01668. PMC 5623122. PMID 29018388.
- Triscari MT, Faraci P, Catalisano D, D'Angelo V, Urso V (2015). "Effectiveness of cognitive behavioral therapy integrated with systematic desensitization, cognitive behavioral therapy combined with eye movement desensitization and reprocessing therapy, and cognitive behavioral therapy combined with virtual reality exposure therapy methods in the treatment of flight anxiety: a randomized trial". Neuropsychiatric Disease and Treatment. 11: 2591–2598. doi:10.2147/ndt.s93401. PMC 4605250. PMID 26504391.
- De Jongh A, ten Broeke E (2007). "Treatment of Specific Phobias With EMDR: Conceptualization and Strategies for the Selection of Appropriate Memories". Journal of EMDR Practice and Research. 1 (1): 46–56. doi:10.1891/1933-3196.1.1.46. ISSN 1933-3196. S2CID 219207280.
- De Jongh A, Ten Broeke E, Renssen MR (1999). "Treatment of specific phobias with Eye Movement Desensitization and Reprocessing (EMDR): protocol, empirical status, and conceptual issues". Journal of Anxiety Disorders. 13 (1–2): 69–85. doi:10.1016/S0887-6185(98)00040-1. PMID 10225501.
- Ventis WL, Higbee G, Murdock SA (April 2001). "Using humor in systematic desensitization to reduce fear". The Journal of General Psychology. 128 (2): 241–253. doi:10.1080/00221300109598911. PMID 11506052. S2CID 27950041.
- Botella C, Fernández-Álvarez J, Guillén V, García-Palacios A, Baños R (July 2017). "Recent Progress in Virtual Reality Exposure Therapy for Phobias: A Systematic Review". Current Psychiatry Reports. 19 (7): 42. doi:10.1007/s11920-017-0788-4. hdl:10234/169957. PMID 28540594. S2CID 22637578.
- North MM, North SM, Coble JR (1997). "Virtual reality therapy: an effective treatment for psychological disorders". Studies in Health Technology and Informatics. IOS Press. 44: 59–70. PMID 10175343.
- Feldman MD, Christensen JF, Satterfield JM, Laponis R (2020). Behavioral medicine : a guide for clinical practice (Fifth ed.). New York. ISBN 978-1-260-14269-3. OCLC 1112141174.
{{cite book}}: CS1 maint: location missing publisher (link) - Marshall JR (1995). "Integrated treatment of social phobia". Bulletin of the Menninger Clinic. 59 (2 Suppl A): A27–A37. PMID 7795569.
- Stein DJ (16 February 2004). "Specific Phobia". Clinical Manual of Anxiety Disorders (1st ed.). US: American Psychiatric Press Inc. p. 53. ISBN 978-1-58562-076-0.
Fears are common in children and adolescents. However, for some youth, these fears persist and develop into specific phobias. A specific phobia is an intense, enduring fear of an identifiable object or situation that may lead to panic symptoms, distress, and avoidance (e.g., fears of dogs, snakes, storms, heights, costumed characters, the dark, and similar objects or situations). Moreover, phobias can affect a youngster's quality of life by interfering with school, family, friends, and free-time. It is estimated that 5% to 10% of youth will develop a phobia before reaching the age of 16.
- Loscalzo J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL (April 2022). Harrison's principles of internal medicine (21st ed.). New York: McGraw Hill / Medical. pp. Chapter 452. ISBN 978-1-264-26849-8. OCLC 1282172709.
- Williamson, Ann (January 2019). "What is hypnosis and how might it work?". Palliative Care: Research and Treatment. 12: 117822421982658. doi:10.1177/1178224219826581. ISSN 1178-2242. PMC 6357291. PMID 30728719.
- Iglesias A, Iglesias A, Iglesias A (October 2013). "I-95 phobia treated with hypnotic systematic desensitization: a case report". The American Journal of Clinical Hypnosis. 56 (2): 143–151. doi:10.1080/00029157.2013.785930. PMID 24665816. S2CID 25059518.
- Vickers A, Zollman C, Payne DK (October 2001). "Hypnosis and relaxation therapies". The Western Journal of Medicine. 175 (4): 269–272. doi:10.1136/ewjm.175.4.269. PMC 1071579. PMID 11577062.
- Hendriks SM, Spijker J, Licht CM, Beekman AT, Penninx BW (September 2013). "Two-year course of anxiety disorders: different across disorders or dimensions?". Acta Psychiatrica Scandinavica. 128 (3): 212–221. doi:10.1111/acps.12024. PMID 23106669. S2CID 8009247.
- de Vries YA, Harris MG, Vigo D, Chiu WT, Sampson NA, Al-Hamzawi A, et al. (June 2021). "Perceived helpfulness of treatment for specific phobia: Findings from the World Mental Health Surveys". Journal of Affective Disorders. 288: 199–209. doi:10.1016/j.jad.2021.04.001. PMC 8154701. PMID 33940429.
- Kessler et al., Prevalence, Severity, and Comorbidity of 12-Month DSM-IV Disorders in the National Comorbidity Survey Replication, June 2005, Archive of General Psychiatry, Volume 20
- "Phobias Symptoms & Causes". Boston Children's Hospital. Archived from the original on 4 February 2019. Retrieved 8 June 2019.
- den Boer JA (September 1997). "Social phobia: epidemiology, recognition, and treatment". BMJ. 315 (7111): 796–800. doi:10.1136/bmj.315.7111.796. PMC 2127554. PMID 9345175.
- Merikangas KR, Nakamura EF, Kessler RC (2009-03-11). "Epidemiology of mental disorders in children and adolescents". Dialogues in Clinical Neuroscience. 11 (1): 7–20. doi:10.31887/DCNS.2009.11.1/krmerikangas. PMC 2807642. PMID 19432384.
- Fredrikson M, Annas P, Fischer H, Wik G (January 1996). "Gender and age differences in the prevalence of specific fears and phobias". Behaviour Research and Therapy. 34 (1): 33–39. doi:10.1016/0005-7967(95)00048-3. PMID 8561762.
- Essau CA, Conradt J, Petermann F (September 1999). "Frequency and comorbidity of social phobia and social fears in adolescents". Behaviour Research and Therapy. 37 (9): 831–843. doi:10.1016/S0005-7967(98)00179-X. PMID 10458047.
- Janssen DF (September 2021). "'On the different Species of Phobia' and 'On the different Species of Mania' (1786): from popular furies to mental disorders in America". Medical Humanities. BMJ Journals. 47 (3): 365–374. doi:10.1136/medhum-2020-011859. PMID 33318050. S2CID 229163411.
- Abbasi J (25 Jul 2011), "Is Trypophobia a real phobia?", Popular Science, archived from the original on 2016-04-07, retrieved 10 Apr 2016
- Griffin, Gabriele (2008). homophobia. ISBN 978-0-19-183483-7. Retrieved 2022-07-13.
{{cite book}}:|work=ignored (help) - Dugan D (2006-04-07), The Benchwarmers (Comedy, Sport), Revolution Studios, Happy Madison Productions, retrieved 2022-03-08
- "Monk TV Series, Detective Monk Television Show – USA Network". 2009-11-03. Archived from the original on 3 November 2009. Retrieved 2022-03-08.
- "Shameless". SHO.com. Retrieved 2022-03-08.
- "Electroconvulsive Therapy (ECT)". Stanford Health Care. Healthwise. 2021. Retrieved 2022-03-16.
- "Transcranial Magnetic Stimulation (TMS)". Stanford Health Care. Healthwise. Retrieved 2022-03-16.
- Cirillo P, Gold AK, Nardi AE, Ornelas AC, Nierenberg AA, Camprodon J, Kinrys G (June 2019). "Transcranial magnetic stimulation in anxiety and trauma-related disorders: A systematic review and meta-analysis". Brain and Behavior. 9 (6): e01284. doi:10.1002/brb3.1284. PMC 6576151. PMID 31066227.
- Mataix-Cols D, Fernández de la Cruz L, Monzani B, Rosenfield D, Andersson E, Pérez-Vigil A, et al. (May 2017). "D-Cycloserine Augmentation of Exposure-Based Cognitive Behavior Therapy for Anxiety, Obsessive-Compulsive, and Posttraumatic Stress Disorders: A Systematic Review and Meta-analysis of Individual Participant Data". JAMA Psychiatry. 74 (5): 501–510. doi:10.1001/jamapsychiatry.2016.3955. PMID 28122091. S2CID 205144078.
Further reading
- Wechsler TF, Kümpers F, Mühlberger A (2019). "Inferiority or Even Superiority of Virtual Reality Exposure Therapy in Phobias?-A Systematic Review and Quantitative Meta-Analysis on Randomized Controlled Trials Specifically Comparing the Efficacy of Virtual Reality Exposure to Gold Standard in vivo Exposure in Agoraphobia, Specific Phobia, and Social Phobia". Frontiers in Psychology. 10: 1758. doi:10.3389/fpsyg.2019.01758. PMC 6746888. PMID 31551840.
- Igawa M, Kato M (2017-09-20). "A new species of hermit crab, Diogenes heteropsammicola (Crustacea, Decapoda, Anomura, Diogenidae), replaces a mutualistic sipunculan in a walking coral symbiosis". PLOS ONE. 12 (9): e0184311. Bibcode:2017PLoSO..1284311I. doi:10.1371/journal.pone.0184311. PMC 5606932. PMID 28931020.
External links
 Media related to Phobias at Wikimedia Commons
Media related to Phobias at Wikimedia Commons- Social Anxiety at Curlie