Peripheral artery disease
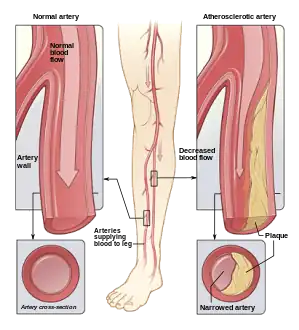
Peripheral artery disease (PAD) is an abnormal narrowing of arteries other than those that supply the heart or brain.[5][15] PAD can happen in any blood vessel, but it is more common in the legs than the arms.[16]
| Peripheral artery disease | |
|---|---|
| Other names | Peripheral vascular disease (PVD), peripheral artery occlusive disease, peripheral obliterative arteriopathy |
 | |
| An arterial insufficiency ulcer in a person with severe peripheral artery disease[1] | |
| Specialty | Interventional radiology, vascular surgery |
| Symptoms | Leg pain when walking that resolves with rest, skin ulcers, bluish skin, cold skin[2][3] |
| Complications | Infection, amputation[4] |
| Causes | Atherosclerosis, artery spasm[5][6] |
| Risk factors | Cigarette smoking, diabetes, high blood pressure, high blood cholesterol.[4][7] |
| Diagnostic method | Ankle-brachial index < 0.90, duplex ultrasonography, angiography[8][9] |
| Treatment | Stopping smoking, supervised exercise therapy, surgery[10][11][12] |
| Medication | Statins, ACE inhibitors, cilostazol[12] |
| Frequency | 155 million (2015)[13] |
| Deaths | 52,500 (2015)[14] |
When narrowing occurs in the heart, it is called coronary artery disease (CAD), and in the brain, it is called cerebrovascular disease.[4] Peripheral artery disease most commonly affects the legs, but other arteries may also be involved, such as those of the arms, neck, or kidneys.[4][17]
Peripheral artery disease (PAD) is a form of peripheral vascular disease. Vascular refers to both the arteries and veins within the body. PAD differs from peripheral veinous disease. PAD means the arteries are narrowed or blocked—the vessels that carry oxygen-rich blood as it moves away from the heart to other parts of the body. Peripheral veinous disease, on the other hand, refers to problems with veins—the vessels that bring the blood back to the heart.[18]
The classic symptom is leg pain when walking, which resolves with rest and is known as intermittent claudication.[2] Other symptoms include skin ulcers, bluish skin, cold skin, or abnormal nail and hair growth in the affected leg.[3] Complications may include an infection or tissue death, which may require amputation; coronary artery disease; or stroke.[4] Up to 50% of people with PAD do not have symptoms.[2]
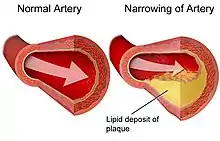
The greatest risk factor for PAD is cigarette smoking.[4] Other risk factors include diabetes, high blood pressure, kidney problems, and high blood cholesterol.[7][19] PAD is primarily caused by the buildup of fatty plaque in the arteries, which is called atherosclerosis, especially in individuals over 40 years old.[6][20][16] Other mechanisms include artery spasm, blood clots, trauma, fibromuscular dysplasia, and vasculitis.[5][19] PAD is typically diagnosed by finding an ankle-brachial index (ABI) less than 0.90, which is the systolic blood pressure at the ankle divided by the systolic blood pressure of the arm.[9] Duplex ultrasonography and angiography may also be used.[8] Angiography is more accurate and allows for treatment at the same time; however, it is associated with greater risks.[9]
It is unclear if screening for peripheral artery disease in people without symptoms is useful, as it has not been properly studied.[21][22][20] For those with intermittent claudication from PAD, stopping smoking and supervised exercise therapy may improve outcomes.[11][12] Medications, including statins, ACE inhibitors, and cilostazol, may also help.[12][23] Aspirin, which helps with thinning the blood and thus improving blood flow, does not appear to help those with mild disease but is usually recommended for those with more significant disease due to the increased risk of heart attacks.[20][24][25] Anticoagulants (blood thinners) such as warfarin show no definitive scientific evidence of benefit in PAD.[26] Surgical procedures used to treat PAD include bypass grafting, angioplasty, and atherectomy.[10]
In 2015, about 155 million people had PAD worldwide.[13] It becomes more common with age.[27] In the developed world, it affects about 5.3% of 45- to 50-year-olds and 18.6% of 85- to 90-year-olds.[7] In the developing world, it affects 4.6% of people between the ages of 45 and 50 and 15% of people between the ages of 85 and 90.[7] PAD in the developed world is equally common among men and women, though in the developing world, women are more commonly affected.[7] In 2015, PAD resulted in about 52,500 deaths, which is an increase from the 16,000 deaths in 1990.[14][28]
Signs and symptoms

The signs and symptoms of peripheral artery disease are based on the part of the body that is affected. About 66% of patients affected by PAD either do not have symptoms or have atypical symptoms.[19] The most common presenting symptom is intermittent claudication (IC), which typically refers to lower extremity skeletal muscle pain that occurs during exercise. IC presents when there is insufficient oxygen delivery to meet the metabolic requirements of the skeletal muscles. IC is a common manifestation of peripheral arterial disease (PAD). The pain is usually located in the calf muscles of the affected leg and is relieved by rest.[30] This occurs because during exercise, the muscles require more oxygen. Normally, the arteries would be able to increase the amount of blood flow and therefore increase the amount of oxygen going to the exercised muscle. However, in PAD, the artery is unable to respond appropriately to the increased demand for oxygen from the muscles, and as a result, the muscles are deprived of oxygen, leading to muscle pain that subsides with rest.[30]
Other symptoms may include:[31]
- Pain, aches, and/or cramps in the buttocks, hip, or thigh
- Muscle atrophy (muscle loss) of the affected limb
- Hair loss of the affected limb
- Skin that is smooth, shiny, or cool to the touch in the affected area
- Decreased or absent pulse in the feet
- Cold and/or numbness in the toes
- Sores/ulcers on the affected limb that do not heal
In individuals with severe PAD, complications may arise, including critical limb ischemia and gangrene. Critical limb ischemia occurs when the obstruction of blood flow in the artery is compromised to the point where the blood is unable to maintain oxygenation of the tissue at rest.[19] This can lead to pain at rest, a feeling of coldness, or numbness in the affected foot and toes. Other complications of severe PAD include lower limb tissue loss (amputation), arterial insufficiency ulcers, erectile dysfunction, and gangrene.[32] People with diabetes are affected by gangrene of the feet at a rate that is 30 times higher than the unaffected population. Many of these severe complications, such as those leading to amputation, are irreversible.[33]
Causes
Risk factors
Factors contributing to an increased risk of PAD are the same as those for atherosclerosis.[34][35] These include age, sex, and ethnicity.[36] PAD is twice as common in males as in females. In terms of ethnicity, PAD is more common in people of color compared to the white population in a 2:1 ratio.[37] The factors with the greatest risk associations are hyperlipidemia, hypertension, diabetes mellitus, chronic kidney disease, and smoking. Presenting three of these factors or more increases the risk of developing PAD tenfold.[38]
- Smoking – Tobacco use in any form is the single greatest risk factor for peripheral artery disease internationally. Smokers have up to a 10-fold increase in the risk of PAD in a dose-response relationship.[35] Exposure to second-hand smoke has also been shown to promote changes in the lining of blood vessels (endothelium), which can lead to atherosclerosis. Smokers are 2-3 times more likely to have lower extremity PAD than coronary artery disease.[39] Greater than 80%–90% of patients with lower extremity peripheral arterial disease are current or former smokers.[40] The risk of PAD increases with the number of cigarettes smoked per day and the number of years smoked.[41][42]
- High blood sugar – Diabetes mellitus is shown to increase the risk of PAD by 2-4 fold. It does this by causing endothelial and smooth-muscle cell dysfunction in peripheral arteries.[43][44][45] The risk of developing lower extremity peripheral arterial disease is proportional to the severity and duration of diabetes.[46]
- High blood cholesterol – Dyslipidemia, which is an abnormally high level of cholesterol or fat in the blood.[36] Dyslipidemia is caused by a high level of a protein called low-density lipoprotein (LDL cholesterol), low levels of high-density lipoprotein (HDL cholesterol), elevation of total cholesterol, and/or high triglyceride levels. This abnormality in blood cholesterol levels has been correlated with accelerated peripheral artery disease. Management of dyslipidemia by diet, exercise, and/or medication is associated with a major reduction in rates of heart attack and stroke.[47]
- High blood pressure – Hypertension or elevated blood pressure can increase a person's risk of developing PAD. Similarly to PAD, there is a known association between high blood pressure and heart attacks, strokes, and abdominal aortic aneurysms. High blood pressure increases the risk of intermittent claudication, the most common symptom of PAD, by 2.5- to 4-fold in men and women, respectively.[48]
- Other risk factors that are being studied include levels of various inflammatory mediators such as C-reactive protein, fibrinogen, homocysteine, and lipoprotein A.[49] Individuals with increased levels of homocysteine in their blood have a 2-fold risk of developing peripheral artery disease.[36] While there are genetic factors leading to risk factors for peripheral artery disease, including diabetes and high blood pressure, there have been no specific genes or gene mutations directly associated with the development of peripheral artery disease.[36]
High risk populations
Peripheral arterial disease is more common in these populations:[42][50]
- All people who have leg symptoms with exertion (suggestive of claudication) or ischemic rest pain
- All people aged 65 years and over, regardless of risk factor status
- All people between 50 and 69 who have a cardiovascular risk factor (particularly diabetes or smoking)
- Age less than 50 years, with diabetes and one other atherosclerosis risk factor (smoking, dyslipidemia, hypertension, or hyperhomocysteinemia)
- Individuals with an abnormal lower extremity pulse examination
- Those with known atherosclerotic coronary, carotid, or renal artery disease
- All people with a Framingham risk score of 10%–20%
- All people who have previously experienced chest pain
Etiology and pathophysiology
Peripheral arterial disease is considered to be a set of chronic or acute syndromes, generally derived from the presence of occlusive arterial disease, which causes inadequate blood flow to the limbs.[51][52]
As previously mentioned, the most common etiology of peripheral artery disease, especially in patients over 40 years old, is atherosclerosis.[19] Atherosclerosis is a narrowing of the arteries caused by lipid or fat buildup and calcium deposition in the wall of the affected arteries.
The pathophysiology of atherosclerosis involves complex interactions between cholesterol and vascular cells.[52] In the early stages of PAD, the arteries compensate for the plaque buildup by dilating to preserve flow through the vessel. Eventually, the artery cannot dilate any further, and the atherosclerotic plaque starts to narrow the arterial flow lumen.[51]
When there is an imbalance between the needs of the peripheral tissues and the blood supply, we are faced with a situation of ischemia.
From the pathophysiologic point of view, a restriction of blood supply (ischemia) to the lower limbs can be classified as either functional or critical. Functional ischemia occurs when the blood flow is normal at rest but insufficient during exercise, presenting clinically as intermittent claudication. Critical ischemia is produced when the reduction in blood flow results in a perfusion deficit at rest and is defined by the presence of pain at rest or trophic lesions in the legs. In this situation, precise diagnosis is fundamental, as there is a clear risk of loss of the limb if adequate blood flow is not re-established, either by surgery or by endovascular therapy. Differentiating between the two concepts is important in order to establish the therapeutic indication and the prognosis in patients with PAD.[52]
Other causes include vasculitis and in situ thrombosis related to hypercoagulable states.[53] Additional mechanisms of peripheral artery disease include arterial spasm and fibromuscular dysplasia.[19] The cause and pathophysiology of arterial spasm are not fully understood, but it is hypothesised that they can occur secondary to trauma.[54] The symptoms of claudication ensue when the artery spasms, or clamps down on itself, creating an obstruction. Similar to atherosclerosis, this leads to decreased blood flow to the tissue downstream of the obstruction. Thrombosis, or the formation of a blood clot, usually occurs due to stasis or trauma.[54]
Diagnosis

Diagnosing or identifying peripheral artery disease requires a history of symptoms and a physical exam, followed by confirmatory testing.[20] These tests could include CT scans (Computed Tomographic Angiography), MRA scans (Magnetic Resonance Angiography), or ultrasounds for imaging.[31] In the setting of symptoms consistent with peripheral artery disease, a physician will then examine an individual for specific exam findings. Abnormal physical exam findings can lead a health care provider to consider a specific diagnosis.[19] However, in order to confirm a diagnosis, confirmatory testing is required.[20]
These findings are associated with peripheral artery disease:[19]
- Decreased or absent pulses
- Muscle atrophy or wasting
- Noticeable blueness of the affected limb
- Decreased temperature (coolness) in the affected limb when compared to the other
- Thickened nails
- Smooth or shiny skin and hair loss
- Buerger's test can check for pallor when the affected limb is in an elevated position. The limb is then moved from an elevated to a sitting position and checked for redness, which is called reactive hyperemia. Buerger's test is an assessment of arterial sufficiency, which is the ability of the artery to supply oxygenated blood to the tissue that it goes to.
- Nonhealing lower extremity wound[38]
If peripheral artery disease is suspected, the initial study is the ankle–brachial index (ABI).[20] The ABI is a simple, non-invasive test that measures the ratio of systolic blood pressure in the ankle to the systolic blood pressure in the upper arm. This is based on the idea that if blood pressure readings in the ankle are lower than those in the arm, a blockage in the arteries that provide blood from the heart to the ankle is suspected.[55] An ABI range of 0.90 to 1.40 is considered normal. A person is considered to have PAD when the ABI is ≤ 0.90. However, PAD can be further graded as mild to moderate if the ABI is between 0.41 and 0.90, and severe if the ABI is less than 0.40. These categories can provide insight into the disease course.[42] Furthermore, ABI values of 0.91 to 0.99 are considered borderline, and values >1.40 indicate noncompressible arteries. If an ABI >1.40 is calculated, this could indicate vessel wall stiffness caused by calcification, which can occur in people with uncontrolled diabetes. Abnormally high ABIs (>1.40) are usually considered false negatives, and thus, such results merit further investigation and higher-level studies.[56] Individuals with noncompressible arteries have an increased risk of cardiovascular mortality within a two-year period.[57]
Individuals with suspected PAD with normal ABIs can undergo exercise testing for ABI. A baseline ABI is obtained prior to exercise. The patient is then asked to exercise (usually patients are made to walk on a treadmill at a constant speed) until claudication pain occurs (for a maximum of 5 minutes), after which the ankle pressure is again measured. A decrease in ABI of 15%–20% would be diagnostic of PAD.[42][50]
If ABIs are abnormal, the next step is generally a lower limb Doppler ultrasound to look at the site of obstruction and extent of atherosclerosis. Other imaging can be performed by angiography,[34] where a catheter is inserted into the common femoral artery and selectively guided to the artery in question. While injecting a radio-dense contrast agent, an X-ray is taken. Any blood flow-limiting blockage found in the X-ray can be identified and treated by procedures including atherectomy, angioplasty, or stenting. Contrast angiography is the most readily available and widely used imaging technique. Modern computerized tomography (CT) scanners provide direct imaging of the arterial system. Studies have shown the sensitivity and specificity of CT in identifying lesions with >50% stenosis to be 95% and 96%, respectively.[58] As such, CT may be considered as an alternative to invasive angiography. An important distinction between the two is that, unlike invasive angiography, assessment of the arterial system with CT does not allow for vascular intervention.[59]
Magnetic resonance angiography (MRA) is a noninvasive diagnostic procedure that uses a combination of a large magnet, radio frequencies, and a computer to produce detailed images of blood vessels inside the body. The advantages of MRA include its safety and ability to provide high-resolution, three-dimensional imaging of the entire abdomen, pelvis, and lower extremities in one sitting.[60][61]
Classification

The two most commonly used methods to classify peripheral artery disease are the Fontaine and Rutherford systems of classification.[62] The Fontaine stages were introduced by René Fontaine in 1954 to define the severity of chronic limb ischemia:[50][62][63]
- Stage I: asymptomatic
- Stage IIa: intermittent claudication after walking a distance of more than 200 meters
- Stage IIb: intermittent claudication after walking a distance of less than 200 meters
- Stage III: rest pain
- Stage IV: ulcers or gangrene of the limb
The Rutherford classification was created by the Society for Vascular Surgery and the International Society of Cardiovascular Surgery, introduced in 1986 and revised in 1997 (and known as the Rutherford classification after the lead author, Robert B. Rutherford). This classification system consists of four grades and seven categories (categories 0–6):[50][64]
- Grade 0, Category 0: asymptomatic
- Grade I, Category 1: mild claudication
- Grade I, Category 2: moderate claudication
- Grade I, Category 3: severe claudication
- Grade II, Category 4: rest pain
- Grade III, Category 5: minor tissue loss; ischemic ulceration not exceeding ulcer of the digits of the foot
- Grade IV, Category 6: major tissue loss; severe ischemic ulcers or frank gangrene
Moderate to severe PAD, classified by Fontaine's stages III to IV or Rutherford's categories 4 to 5, presents a limb threat (risk of limb loss) in the form of critical limb ischemia.[65]
Recently, the Society for Vascular Surgery came out with a classification system based on "wound, ischemia and foot infection" (WIfI).[66] This classification system, published in 2013, was created to account for the demographic changes that have occurred over the past forty years, including the increased incidence of high blood sugar and evolving techniques and abilities for revascularization. This system was created on the basis that ischemia and angiographic disease patterns are not the sole determinants of amputation risk.[67] The WIfI classification system is broken up into two parts: wounds and ischemia. Wounds are graded 0 through 3 based on the presence of ulceration, gangrene, and ischemia.[66]
- Grade 0: no ulcer, no gangrene
- Grade 1: small, shallow ulcer; no gangrene
- Grade 2: deep ulcer with exposed tendon or bone, gangrene limited to toes
- Grade 3: extensive, full-thickness ulcer; gangrene extending to the forefoot or midfoot
Ischemia is graded 0 through 3 based on ABI, ankle systolic pressure, and toe pressure.[66]
- Grade 0: ABI ≥0.80, ankle systolic pressure ≥100 mm Hg, toe pressure ≥60 mm Hg
- Grade 1: arterial brachial index 0.6 to 0.79, ankle systolic pressure 70 to 100 mm Hg, toe pressure 40 to 59 mm Hg
- Grade 2: ABI 0.4–0.59, ankle systolic pressure 50 to 70 mm Hg, toe pressure 30 to 39 mm Hg
- Grade 3: ABI ≤0.39, ankle systolic pressure <50 mm Hg, toe pressure <30 mm Hg
The TASC (and TASC II) classification suggests PAD treatment is based on the severity of disease seen on an angiogram.[50]
Screening
It is not clear if screening for disease in the general population is useful, as it has not been extensively studied.[21] This includes screening with the ankle-brachial index[68] (ABI), although a systematic review of the literature did not support the use of routine ABI screening in asymptomatic patients.[69]
Testing for coronary artery disease or carotid artery disease is of unclear benefit.[20] While PAD is a risk factor for abdominal aortic aneurysms (AAA), there is no data on screening individuals with asymptomatic PAD for abdominal aortic aneurysms.[20] For people with symptomatic PAD, screening by ultrasound for AAA is not unreasonable.[20]
Wearable devices and remote patient monitoring
A 2022 review found that a variety of wearable medical devices measuring different parameters (such as body temperature) were being combined with remote patient monitoring of PAD patients, in a goal to improve health outcomes.[70]
Some studies propose the development of devices measuring oxygen continuously during exercise. This is because resting perfusion and metabolic activity are extremely low and differences between non-patients and PAD patients are barely measurable. As such, testing of vascular function and energetics requires a physiological challenge.[71] Pulse oximeters can be inconvenient to wear during exercise and only give oxygen values at discrete time points, nor is there sufficient evidence to support any use in identifying PAD. Some publications and studies therefore discuss the use of wearable sensors measuring oxygen levels continuously in PAD patients, such as through transcutaneous means. However, because transcutaneous measurements are affected by movement (such as during exercise) and body temperature, use of oxygen sensors that are inserted subcutaneously as opposed to transcutaneously may most effectively help monitor a PAD patient’s progress and direct therapy decisions.[72] To date, one oxygen sensing system has been approved for use in Europe to measure tissue perfusion in all PAD patients.[73]
Treatment
Depending on the severity of the disease, these steps can be taken, according to these guidelines:[74]
Lifestyle
- Stopping smoking (cigarettes promote PAD and are a risk factor for cardiovascular disease)
- Regular exercise for those with claudication helps open up alternative small vessels (collateral flow), and the limitation in walking often improves. Treadmill exercise (35 to 50 minutes, three or four times per week[34]) has been reviewed as another treatment with a number of positive outcomes, including a reduction in cardiovascular events and improved quality of life. Supervised exercise programs increase pain-free walking time and the maximum walking distance in people with PAD.
Medication
- Management of diabetes
- Management of hypertension
- Management of high cholesterol, and antiplatelet drugs such as aspirin and clopidogrel. Statins reduce clot formation and cholesterol levels, respectively, and can help with disease progression and address the other cardiovascular risks that the affected person is likely to have.
According to guidelines, taking aspirin or clopidogrel is recommended to reduce AMI ("heart attack"), stroke, and other causes of vascular death in people with symptomatic peripheral artery disease.[20] It is recommended that aspirin and clopidogrel be taken alone and not in conjunction with one another (i.e., not as dual antiplatelet therapy). The recommended daily dosage of aspirin for treating PAD is between 75 and 325 mg, while the recommended daily dosage for clopidogrel is 75 mg.[38] The effectiveness of both aspirin and clopidogrel to reduce the risk of cardiovascular ischemic events in people with symptomatic PAD is not well established. Research also suggests that low-dose rivaroxaban plus aspirin is effective as a new anti-thrombotic regimen for PAD.[75]
Cilostazol can improve symptoms in some people.[23] Pentoxifylline is of unclear benefit.[76] Cilostazol may improve walking distance for people who experience claudication due to peripheral artery disease, but no strong evidence suggests that it improves the quality of life, decreases mortality, or decreases the risk of cardiovascular events.[23]
Treatment with other drugs or vitamins is unsupported by clinical evidence, "but trials evaluating the effect of folate and vitamin B12 on hyperhomocysteinemia, a putative vascular risk factor, are near completion".[74]
Revascularization
After a trial of the best medical treatment outlined above, if symptoms persist, patients may be referred to a vascular or endovascular surgeon. The benefit of revascularization is thought to correspond to the severity of ischemia and the presence of other risk factors for limb loss, such as wound and infection severity.[67]
- Angioplasty (or percutaneous transluminal angioplasty) can be done on solitary lesions in large arteries, such as the femoral artery, but may not have sustained benefits.[77] Patency rates following angioplasty are highest for iliac arteries and decrease with arteries towards the toes. Other criteria that affect the outcome following revascularization are the length of the lesion and the number of lesions.[78][79] There do not appear to be any long-term advantages or sustained benefits to placing a stent following angioplasty in order to hold the narrowing of the subsartorial artery open.[80]
 3D Medical Animation still shot depicting the Vascular Bypass Grafting
3D Medical Animation still shot depicting the Vascular Bypass Grafting - Atherectomy, in which the plaque is scraped off the inside of the vessel wall (albeit with no better results than angioplasty).[81]
- Vascular bypass grafting can be performed to circumvent a diseased area of the arterial vasculature. The great saphenous vein is used as a conduit if available, although artificial (Gore-Tex or PTFE) material is often used for long grafts when adequate venous conduit is unavailable.
- When gangrene has set in, amputation may be required to prevent infected tissues from causing sepsis, a life-threatening illness.
- Thrombolysis and thrombectomy are used in cases of arterial thrombosis or embolism.
- shockwave intravascular lithotripsy, a minimally-invasive method which uses ultrasound waves to break up plaque within the artery without need for penetration. The method was first approved by the US Food and Drug Administration in February 2021,[82] and has been used as a complement to more widely-used methods of atherectomy.
Guidelines
A guideline from the American College of Cardiology and American Heart Association for the diagnosis and treatment of lower extremity, renal, mesenteric, and abdominal aortic PAD was compiled in 2013, combining the 2005 and 2011 guidelines.[42] For chronic limb-threatening ischemia, the ACCF/AHA guidelines recommend balloon angioplasty only for people with a life expectancy of 2 years or less or those who do not have an autogenous vein available. For those with a life expectancy greater than 2 years or who have an autogenous vein, bypass surgery is recommended.[83]
Prognosis
Individuals with PAD have an "exceptionally elevated risk for cardiovascular events and the majority will eventually die of a cardiac or cerebrovascular etiology".[84] Prognosis is correlated with the severity of the PAD as measured by an ABI.[84] Large-vessel PAD increases mortality from cardiovascular disease significantly. PAD carries a greater than "20% risk of a coronary event in 10 years".[84]
The risk is low that an individual with claudication will develop severe ischemia and require amputation, but the risk of death from coronary events is three to four times higher than matched controls without claudication.[74] Of patients with intermittent claudication, only "7% will undergo lower-extremity bypass surgery, 4% major amputations, and 16% worsening claudication", but stroke and heart attack events are elevated, and the "5-year mortality rate is estimated to be 30% (versus 10% in controls)".[84]
Epidemiology
The prevalence of PAD in the general population is 3–7%, affecting up to 20% of those over 70;[85] 70%–80% of affected individuals are asymptomatic; only a minority ever require revascularization or amputation. Peripheral artery disease affects one in three diabetics over the age of 50. In the US, it affects 12–20 percent of Americans age 65 and older. Around 10 million Americans have PAD. Despite its prevalence and implications for cardiovascular risk, there are still low levels of awareness of risk factors and symptoms, with 26% of the population in the US reported to have knowledge of PAD.[86]
In 2000, among people aged 40 years and older in the United States, rates of PAD were 4.3%.[87] Rates were 14.5% for people aged 70 years or over. Within age groups, rates were generally higher for women than men. Non-Hispanic blacks had a rate of 7.9% compared to 4.4% in Non-Hispanic whites and 3.0% (1.4%–4.6%) in Mexican Americans.[87]
The incidence of symptomatic PAD increases with age, from about 0.3% per year for men aged 40–55 years to about 1% per year for men aged over 75 years. The prevalence of PAD varies considerably depending on how PAD is defined and the age of the population being studied. People diagnosed with PAD have a greater risk of a MACE (Major Adverse Cardiac Event) and stroke. Their risk of developing a reinfarction, stroke, or transient ischemic attack within one year following a heart attack increases to 22.9%, compared to 11.4% for those without PAD.[88]
The Diabetes Control and Complications Trial and the UK Prospective Diabetes Study trials in people with type 1 and type 2 diabetes, respectively, demonstrated that glycemic control is more strongly associated with microvascular disease than macrovascular disease. Pathologic changes occurring in small vessels may be more sensitive to chronically elevated glucose levels than atherosclerosis occurring in larger arteries.[89]
Research
Research is being done on therapies to prevent the progression of PAD.[90] In those who have developed critically poor blood flow to the legs, the benefit of autotransplantation of autologous mononuclear cells is unclear.[91]
Only one randomized controlled trial has been conducted comparing vascular bypass to angioplasty for the treatment of severe PAD.[92] The trial found no difference in amputation-free survival between vascular bypass and angioplasty at the planned clinical endpoint, but the trial has been criticized as being underpowered, limiting endovascular options, and comparing inappropriate endpoints.[93] As of 2017, two randomized clinical trials are being conducted to better understand the optimal revascularization technique for severe PAD and critical limb ischemia (CLI), the BEST-CLI (Best Endovascular Versus Best Surgical Therapy for Patients With Critical Limb Ischemia) Trial and the BASIL-2 (Bypass Versus Angioplasty in Severe Ischaemia of the Leg – 2 )Trial.[94][95]
In 2011, pCMV-vegf165 was registered in Russia as the first-in-class gene therapy drug for the treatment of PAD, including the advanced stage of critical limb ischemia.[96][97]
References
- Moore J (September 1, 2008). "Creating the Ideal Microcosm for Rapid Incorporation of Bioengineered Alternative Tissues Using An Advanced Hydrogel Impregnated Gauze Dressing: A Case Series". The Foot & Ankle Journal. doi:10.3827/faoj.2008.0109.0002.
- Violi F, Basili S, Berger JS, Hiatt WR (2012). "Antiplatelet Therapy in Peripheral Artery Disease". Antiplatelet Agents. Handbook of Experimental Pharmacology. Vol. 210. pp. 547–563. doi:10.1007/978-3-642-29423-5_22. ISBN 978-3-642-29422-8. PMID 22918746.
- "What Are the Signs and Symptoms of Peripheral Arterial Disease?". nhlbi.nih.gov. August 2, 2011. Archived from the original on February 25, 2015. Retrieved February 26, 2015.
- "What Is Peripheral Arterial Disease?". nhlbi.nih.gov. August 2, 2011. Archived from the original on February 25, 2015. Retrieved February 25, 2015.
- "What Is Peripheral Vascular Disease?" (PDF). American Heart Association (heart.org). 2012. Archived (PDF) from the original on April 12, 2015. Retrieved February 26, 2015.
Peripheral artery disease (PAD) is the narrowing of the arteries to the legs, stomach, arms and head.
- "What Causes Peripheral Arterial Disease?". nhlbi.nih.gov. August 2, 2011. Archived from the original on February 25, 2015. Retrieved February 26, 2015.
- Fowkes FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, et al. (October 2013). "Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis". Lancet. 382 (9901): 1329–1340. doi:10.1016/s0140-6736(13)61249-0. PMID 23915883. S2CID 38652734.
- "How Is Peripheral Arterial Disease Diagnosed?". August 2, 2011. Archived from the original on April 7, 2015. Retrieved March 27, 2015.
- Ruiz-Canela M, Martínez-González MA (2014). "Lifestyle and dietary risk factors for peripheral artery disease". Circulation Journal. 78 (3): 553–559. doi:10.1253/circj.cj-14-0062. PMID 24492064.
- "How Is Peripheral Arterial Disease Treated?". nhlbi.nih.gov. August 2, 2011. Archived from the original on February 25, 2015. Retrieved February 26, 2015.
- Hageman D, Fokkenrood HJ, Gommans LN, van den Houten MM, Teijink JA (April 2018). "Supervised exercise therapy versus home-based exercise therapy versus walking advice for intermittent claudication". The Cochrane Database of Systematic Reviews. 2018 (4): CD005263. doi:10.1002/14651858.CD005263.pub4. PMC 6513337. PMID 29627967.
- Hankey GJ, Norman PE, Eikelboom JW (February 2006). "Medical treatment of peripheral arterial disease". JAMA. 295 (5): 547–553. doi:10.1001/jama.295.5.547. PMID 16449620.
- Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. (GBD 2015 Disease and Injury Incidence and Prevalence Collaborators) (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- Wang, Haidong; et al. (October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- "Overview of Peripheral Arterial Disease – Heart and Blood Vessel Disorders". Merck Manuals Consumer Version. Retrieved April 30, 2019.
Disorders of arteries that supply the brain with blood are considered separately as cerebrovascular disease.
- Creager MA, Loscalzo J (2018). "Arterial Diseases of the Extremities Chapter 275". Harrison's Principles of Internal Medicine. McGraw Hill. 20. Retrieved April 10, 2023 – via Access Medicine.
- Shantulli S (2018). "Update on peripheral arterial disease: Epidemiology and evidence-based facts". Atherosclerosis.
- Gul F, Janzer SD (2023), "Peripheral Vascular Disease", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 32491414, retrieved April 10, 2023
- Harrison's principles of internal medicine (20 ed.). McGraw-Hill Education / Medical. 2018. ISBN 9781259644047.
- Gerhard-Herman MD, Gornik HL, Barrett C, Barshes NR, Corriere MA, Drachman DE, et al. (March 2017). "2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines". Journal of the American College of Cardiology. 69 (11): 1465–1508. doi:10.1016/j.jacc.2016.11.008. PMID 27851991.
- Andras A, Ferket B (April 2014). "Screening for peripheral arterial disease". The Cochrane Database of Systematic Reviews. 4 (4): CD010835. doi:10.1002/14651858.CD010835.pub2. PMID 24711093.
- U.S. Preventive Services Task Force (December 15, 2014). "Peripheral artery disease screening and cardiovascular disease risk assessment with the ankle-brachial index in adults: recommendation statement". Am Fam Physician. 90 (12): 858A–858D. Archived from the original on March 31, 2017.
- Brown T, Forster RB, Cleanthis M, Mikhailidis DP, Stansby G, Stewart M (June 2021). "Cilostazol for intermittent claudication". The Cochrane Database of Systematic Reviews. 2021 (6): CD003748. doi:10.1002/14651858.CD003748.pub5. PMC 8245159. PMID 34192807.
- Lin JS, Olson CM, Johnson ES, Whitlock EP (September 2013). "The ankle-brachial index for peripheral artery disease screening and cardiovascular disease prediction among asymptomatic adults: a systematic evidence review for the U.S. Preventive Services Task Force". Annals of Internal Medicine. 159 (5): 333–341. doi:10.7326/0003-4819-159-5-201309030-00007. PMID 24026319.
- Poredos P, Jezovnik MK (March 2013). "Is aspirin still the drug of choice for management of patients with peripheral arterial disease?". VASA. Zeitschrift für Gefässkrankheiten. 42 (2): 88–95. doi:10.1024/0301-1526/a000251. PMID 23485835.
- Hauk L (May 2012). "ACCF/AHA update peripheral artery disease management guideline". American Family Physician. 85 (10): 1000–1001. PMID 22612053.
- Creager MA, Beckman JA, Loscalzo J (2013). Vascular medicine : a companion to Braunwald's heart disease (2nd ed.). Philadelphia, PA: Elsevier/Saunders. ISBN 9781455737369. OCLC 810335904.
- GBD 2013 Mortality and Causes of Death Collaborators (January 2015). "Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013". Lancet. 385 (9963): 117–171. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
{{cite journal}}:|author1=has generic name (help) - Münter KC (2016). "Education in wound care: Curricula for doctors and nurses, and experiences from the German wound healing society ICW". Military Medical Research. 3 (1): 29. doi:10.1186/s40779-016-0094-1. PMC 5011891. PMID 27602234.
- Patel SK, Surowiec SM (2023), "Intermittent Claudication", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 28613529, retrieved April 10, 2023
- CDC (September 27, 2021). "Peripheral Arterial Disease (PAD) | cdc.gov". Centers for Disease Control and Prevention. Retrieved November 10, 2021.
- Papadakis MA, McPhee SJ, Rabow RW (September 7, 2018). Current medical diagnosis & treatment 2019 (Fifty-eighth ed.). New York, N.Y. ISBN 9781260117431. OCLC 1048597590.
{{cite book}}: CS1 maint: location missing publisher (link) - Sahu A, Sagar R, Sarkar S, Sagar S (2016). "Psychological effects of amputation: A review of studies from India". Industrial Psychiatry Journal. 25 (1): 4–10. doi:10.4103/0972-6748.196041. PMC 5248418. PMID 28163401.
- Peripheral Arterial Disease at Merck Manual of Diagnosis and Therapy Professional Edition. Retrieved August 9, 2010.
- Joosten MM, Pai JK, Bertoia ML, Rimm EB, Spiegelman D, Mittleman MA, Mukamal KJ (October 2012). "Associations between conventional cardiovascular risk factors and risk of peripheral artery disease in men". JAMA. 308 (16): 1660–1667. doi:10.1001/jama.2012.13415. PMC 3733106. PMID 23093164.
- Elsevier Point of Care (December 11, 2018). "Atherosclerotic peripheral artery disease". Clinical Key. Retrieved December 14, 2018.
- "Peripheral Artery Disease". The Lecturio Medical Concept Library. Retrieved October 4, 2021.
- Avery DM, Skinner CA, Reed MD (April 2019). "Supporting Family Physician Maternity Care Providers". Family Medicine. 51 (4): 362. doi:10.22454/fammed.2019.636289. PMID 30973629. S2CID 108295670.
- Price JF, Mowbray PI, Lee AJ, Rumley A, Lowe GD, Fowkes FG (March 1999). "Relationship between smoking and cardiovascular risk factors in the development of peripheral arterial disease and coronary artery disease: Edinburgh Artery Study". European Heart Journal. 20 (5): 344–353. doi:10.1053/euhj.1998.1194. PMID 10206381.
- Smith GD, Shipley MJ, Rose G (December 1990). "Intermittent claudication, heart disease risk factors, and mortality. The Whitehall Study". Circulation. 82 (6): 1925–1931. doi:10.1161/01.cir.82.6.1925. PMID 2242518.
- Cole CW, Hill GB, Farzad E, Bouchard A, Moher D, Rody K, Shea B (October 1993). "Cigarette smoking and peripheral arterial occlusive disease". Surgery. 114 (4): 753–6, discussion 756–7. PMID 8211690.
- Rooke TW, Hirsch AT, Misra S, Sidawy AN, Beckman JA, Findeiss L, et al. (April 2013). "Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines". Journal of the American College of Cardiology. 61 (14): 1555–1570. doi:10.1016/j.jacc.2013.01.004. PMC 4492473. PMID 23473760.
- Kannel WB, McGee DL (1979). "Diabetes and glucose tolerance as risk factors for cardiovascular disease: the Framingham study". Diabetes Care. 2 (2): 120–126. doi:10.2337/diacare.2.2.120. PMID 520114. S2CID 39307266.
- Creager MA, Lüscher TF, Cosentino F, Beckman JA (September 2003). "Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: Part I". Circulation. 108 (12): 1527–1532. doi:10.1161/01.cir.0000091257.27563.32. PMID 14504252.
- Lüscher TF, Creager MA, Beckman JA, Cosentino F (September 2003). "Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: Part II". Circulation. 108 (13): 1655–1661. doi:10.1161/01.cir.0000089189.70578.e2. PMID 14517152.
- Beks PJ, Mackaay AJ, de Neeling JN, de Vries H, Bouter LM, Heine RJ (January 1995). "Peripheral arterial disease in relation to glycaemic level in an elderly Caucasian population: the Hoorn study". Diabetologia. 38 (1): 86–96. doi:10.1007/s001250050257. PMID 7744233.
- Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. (October 2005). "Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins". Lancet. 366 (9493): 1267–1278. doi:10.1016/s0140-6736(05)67394-1. PMID 16214597. S2CID 10716362.
- Kannel WB, McGee DL (January 1985). "Update on some epidemiologic features of intermittent claudication: the Framingham Study". Journal of the American Geriatrics Society. 33 (1): 13–18. doi:10.1111/j.1532-5415.1985.tb02853.x. PMID 3965550. S2CID 13543458.
- Ridker PM, Stampfer MJ, Rifai N (May 2001). "Novel risk factors for systemic atherosclerosis: a comparison of C-reactive protein, fibrinogen, homocysteine, lipoprotein(a), and standard cholesterol screening as predictors of peripheral arterial disease". JAMA. 285 (19): 2481–2485. doi:10.1001/jama.285.19.2481. PMID 11368701.
- TASC II Guidelines
* Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. (2007). "Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II)". European Journal of Vascular and Endovascular Surgery. 33 (Suppl 1): S1-75. doi:10.1016/j.ejvs.2006.09.024. PMID 17140820.
* Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG (January 2007). "Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II)". Journal of Vascular Surgery. 45 (Suppl S): S5-67. doi:10.1016/j.jvs.2006.12.037. PMID 17223489.
* Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, Rutherford RB (June 2007). "Inter-society consensus for the management of peripheral arterial disease". International Angiology. 26 (2): 81–157. PMID 17489079. - Serrano Hernando FJ, Martín Conejero A (September 2007). "[Peripheral artery disease: pathophysiology, diagnosis and treatment]". Revista Espanola de Cardiologia. 60 (9): 969–982. doi:10.1157/13109651. PMID 17915154. S2CID 71164825.
- Zemaitis MR, Boll JM, Dreyer MA (2023), "Peripheral Arterial Disease", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 28613496, retrieved April 10, 2023
- Krishna SM, Moxon JV, Golledge J (May 2015). "A review of the pathophysiology and potential biomarkers for peripheral artery disease". International Journal of Molecular Sciences. 16 (5): 11294–11322. doi:10.3390/ijms160511294. PMC 4463701. PMID 25993296.
- Walls R, Hockberger R, Gausche-Hill M (May 18, 2017). Rosen's Emergency Medicine: Concepts and Clinical Practice (9th ed.). Elsevier, Inc. pp. Chapter 41, pgs 435–444. ISBN 9780323354790.
- Aboyans V, Criqui MH, Abraham P, Allison MA, Creager MA, Diehm C, et al. (December 2012). "Measurement and interpretation of the ankle-brachial index: a scientific statement from the American Heart Association". Circulation. 126 (24): 2890–2909. doi:10.1161/CIR.0b013e318276fbcb. PMID 23159553. S2CID 45644292.
- Vowden P, Vowden K (March 2001). "Doppler assessment and ABPI: Interpretation in the management of leg ulceration". Worldwide Wounds. Archived from the original on May 9, 2008. – describes ABI procedure, interpretation of results, and notes the somewhat arbitrary selection of "ABI of 0.8 has become the accepted endpoint for high-compression therapy, the trigger for referral for a vascular surgical opinion and the defining upper marker for an ulcer of mixed aetiology.
- Amini A, Gordon I, Wilson S, Williams RA (October 2013). "Noncompressible arteries correlate with increased cardiovascular mortality at 2 years". Annals of Vascular Surgery. 27 (7): 918–923. doi:10.1016/j.avsg.2013.01.006. PMID 23993108.
- Met R, Bipat S, Legemate DA, Reekers JA, Koelemay MJ (January 2009). "Diagnostic performance of computed tomography angiography in peripheral arterial disease: a systematic review and meta-analysis". JAMA. 301 (4): 415–424. doi:10.1001/jama.301.4.415. PMID 19176443. S2CID 44960635.
- Shwaiki O, Rashwan B, Fink MA, Kirksey L, Gadani S, Karuppasamy K, et al. (October 2021). "Lower extremity CT angiography in peripheral arterial disease: from the established approach to evolving technical developments". The International Journal of Cardiovascular Imaging. 37 (10): 3101–3114. doi:10.1007/s10554-021-02277-1. PMID 33997924. S2CID 234684675.
- Leiner T, Kessels AG, Nelemans PJ, Vasbinder GB, de Haan MW, Kitslaar PE, et al. (May 2005). "Peripheral arterial disease: comparison of color duplex US and contrast-enhanced MR angiography for diagnosis". Radiology. 235 (2): 699–708. doi:10.1148/radiol.2352040089. PMID 15858107.
- Leiner T (February 2005). "Magnetic resonance angiography of abdominal and lower extremity vasculature". Topics in Magnetic Resonance Imaging. 16 (1): 21–66. doi:10.1097/01.rmr.0000185431.50535.d7. PMID 16314696. S2CID 8026674.
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. (2007). "Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II)". European Journal of Vascular and Endovascular Surgery. 33 (Suppl 1): S1-75. doi:10.1016/j.ejvs.2006.09.024. PMID 17140820.
- Fontaine R, Kim M, Kieny R (December 1954). "[Surgical treatment of peripheral circulation disorders]". Helvetica Chirurgica Acta (in German). 21 (5–6): 499–533. PMID 14366554.
- Rutherford RB, Baker JD, Ernst C, Johnston KW, Porter JM, Ahn S, Jones DN (September 1997). "Recommended standards for reports dealing with lower extremity ischemia: revised version". Journal of Vascular Surgery. 26 (3): 517–538. doi:10.1016/S0741-5214(97)70045-4. PMID 9308598.
- Teraa M, Conte MS, Moll FL, Verhaar MC (February 2016). "Critical Limb Ischemia: Current Trends and Future Directions". Journal of the American Heart Association. 5 (2): e002938. doi:10.1161/JAHA.115.002938. PMC 4802465. PMID 26908409.
- Mills JL, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, Andros G (January 2014). "The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI)". Journal of Vascular Surgery. 59 (1): 220–234.e1–2. doi:10.1016/j.jvs.2013.08.003. PMID 24126108.
- Mills JL, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, Andros G (January 2014). "The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI)". Journal of Vascular Surgery. 59 (1): 220–34.e1–2. doi:10.1016/j.jvs.2013.08.003. PMID 24126108.
- Curry SJ, Krist AH, Owens DK, Barry MJ, Caughey AB, Davidson KW, et al. (July 2018). "Screening for Peripheral Artery Disease and Cardiovascular Disease Risk Assessment With the Ankle-Brachial Index: US Preventive Services Task Force Recommendation Statement". JAMA. 320 (2): 177–183. doi:10.1001/jama.2018.8357. PMID 29998344.
- Alahdab F, Wang AT, Elraiyah TA, Malgor RD, Rizvi AZ, Lane MA, et al. (March 2015). "A systematic review for the screening for peripheral arterial disease in asymptomatic patients". Journal of Vascular Surgery. 61 (3 Suppl): 42S–53S. doi:10.1016/j.jvs.2014.12.008. PMID 25721066.
- Souza, Julio; Escadas, Sara; Baxevani, Isidora; Rodrigues, Daniel; Freitas, Alberto (January 2022). "Smart Wearable Systems for the Remote Monitoring of Selected Vascular Disorders of the Lower Extremity: A Systematic Review". International Journal of Environmental Research and Public Health. 19 (22): 15231. doi:10.3390/ijerph192215231. ISSN 1660-4601. PMC 9690814. PMID 36429951.
- Lopez, D.; Kramer, C. M. (2013). "Oxygenation and flow in the limbs: Novel methods to characterize peripheral artery disease". Curr Cardiovasc Imaging Rep. 6 (2): 157. doi:10.1007/s12410-013-9191-7. PMC 3597748. PMID 23504569.
- Nichols, Scott (2019). "Long-Term in Vivo Oxygen Sensors for Peripheral Artery Disease Monitoring". Oxygen Transport to Tissue XL. Adv Exp Med Biol. Vol. 1072. pp. 351–356. doi:10.1007/978-3-319-91287-5_56. ISBN 978-3-319-91285-1. PMC 6367927. PMID 30178370.
- Inc, Profusa. "Profusa Receives CE Mark Approval to Market the Wireless Lumee® Oxygen Platform for Continuous, Real-Time Monitoring of Tissue Oxygen". www.prnewswire.com. Retrieved September 2, 2023.
{{cite web}}:|last=has generic name (help) - Burns P, Gough S, Bradbury AW (March 2003). "Management of peripheral arterial disease in primary care". BMJ. 326 (7389): 584–588. doi:10.1136/bmj.326.7389.584. PMC 1125476. PMID 12637405.
- Hussain, Mohamad A.; Wheatcroft, Mark; Nault, Patrice; Lindsay, Thomas F.; Bhatt, Deepak L.; Anand, Sonia S.; Verma, Subodh; Al-Omran, Mohammed (2019). "COMPASS for Vascular Surgeons". Current Opinion in Cardiology. 34 (2): 178–184. doi:10.1097/HCO.0000000000000597. PMID 30543542. S2CID 56484366.
- Broderick C, Forster R, Abdel-Hadi M, Salhiyyah K (October 2020). "Pentoxifylline for intermittent claudication". The Cochrane Database of Systematic Reviews. 2020 (10): CD005262. doi:10.1002/14651858.CD005262.pub4. PMC 8094235. PMID 33063850.
- Fowkes FG, Gillespie IN (2000). Fowkes G (ed.). "Angioplasty (versus non surgical management) for intermittent claudication". The Cochrane Database of Systematic Reviews (2): CD000017. doi:10.1002/14651858.CD000017. PMID 10796469.
- Johnston KW, Rae M, Hogg-Johnston SA, Colapinto RF, Walker PM, Baird RJ, et al. (October 1987). "5-year results of a prospective study of percutaneous transluminal angioplasty". Annals of Surgery. 206 (4): 403–413. doi:10.1097/00000658-198710000-00002. PMC 1493220. PMID 2959214.
- Emmerich J (December 2005). "Current state and perspective on medical treatment of critical leg ischemia: gene and cell therapy". The International Journal of Lower Extremity Wounds. 4 (4): 234–241. doi:10.1177/1534734605283538. PMID 16286375. S2CID 18384741.
- Chowdhury MM, McLain AD, Twine CP (June 2014). "Angioplasty versus bare metal stenting for superficial femoral artery lesions". The Cochrane Database of Systematic Reviews. 2014 (6): CD006767. doi:10.1002/14651858.CD006767.pub3. PMC 6544814. PMID 24959692.
- Wardle BG, Ambler GK, Radwan RW, Hinchliffe RJ, Twine CP (September 2020). "Atherectomy for peripheral arterial disease". The Cochrane Database of Systematic Reviews. 2020 (9): CD006680. doi:10.1002/14651858.CD006680.pub3. PMC 8513671. PMID 32990327. S2CID 222151812.
- Health, Center for Devices and Radiological (February 26, 2021). "Shockwave Intravascular Lithotripsy (IVL) System with the Shockwave C2 Coronary Intravascular Lithotripsy (IVL) Catheter – P200039". FDA.
- Rooke TW, Hirsch AT, Misra S, Sidawy AN, Beckman JA, Findeiss LK, et al. (November 2011). "2011 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Peripheral Artery Disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines". Journal of the American College of Cardiology. 58 (19): 2020–2045. doi:10.1016/j.jacc.2011.08.023. PMC 4714326. PMID 21963765.
- Shammas NW (2007). "Epidemiology, classification, and modifiable risk factors of peripheral arterial disease". Vascular Health and Risk Management. 3 (2): 229–234. doi:10.2147/vhrm.2007.3.2.229. PMC 1994028. PMID 17580733.
- Chan KA, Junia A (March 2020). "Lower extremity peripheral artery disease: a basic approach". British Journal of Hospital Medicine. Mark Allen Group. 81 (3): 1–9. doi:10.12968/hmed.2019.0263. PMID 32240007. S2CID 214771540.
- Horváth L, Németh N, Fehér G, Kívés Z, Endrei D, Boncz I (July 2022). "Epidemiology of Peripheral Artery Disease: Narrative Review". Life. 12 (7): 1041. Bibcode:2022Life...12.1041H. doi:10.3390/life12071041. PMC 9320565. PMID 35888129.
- Selvin E, Erlinger TP (August 2004). "Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999-2000". Circulation. 110 (6): 738–743. doi:10.1161/01.CIR.0000137913.26087.F0. PMID 15262830.
- Bauersachs R, Zeymer U, Brière JB, Marre C, Bowrin K, Huelsebeck M (November 26, 2019). "Burden of Coronary Artery Disease and Peripheral Artery Disease: A Literature Review". Cardiovascular Therapeutics. 2019: 8295054. doi:10.1155/2019/8295054. PMC 7024142. PMID 32099582.
- Selvin E, Wattanakit K, Steffes MW, Coresh J, Sharrett AR (April 2006). "HbA1c and peripheral arterial disease in diabetes: the Atherosclerosis Risk in Communities study". Diabetes Care. 29 (4): 877–882. doi:10.2337/diacare.29.04.06.dc05-2018. PMID 16567831. Archived from the original on March 4, 2012.
- Suzuki J, Shimamura M, Suda H, Wakayama K, Kumagai H, Ikeda Y, et al. (April 2016). "Current therapies and investigational drugs for peripheral arterial disease". Hypertension Research. 39 (4): 183–191. doi:10.1038/hr.2015.134. PMID 26631852. S2CID 3070349.
- Moazzami B, Mohammadpour Z, Zabala ZE, Farokhi E, Roohi A, Dolmatova E, Moazzami K (July 2022). "Local intramuscular transplantation of autologous bone marrow mononuclear cells for critical lower limb ischaemia". The Cochrane Database of Systematic Reviews. 2022 (7): CD008347. doi:10.1002/14651858.CD008347.pub4. PMC 9266992. PMID 35802393.
- Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, et al. (December 2005). "Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial". Lancet. 366 (9501): 1925–1934. doi:10.1016/S0140-6736(05)67704-5. PMID 16325694. S2CID 54229954.
- Conte MS (May 2010). "Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) and the (hoped for) dawn of evidence-based treatment for advanced limb ischemia". Journal of Vascular Surgery. 51 (5 Suppl): 69S–75S. doi:10.1016/j.jvs.2010.02.001. PMID 20435263.
- Menard MT, Farber A, Assmann SF, Choudhry NK, Conte MS, Creager MA, et al. (July 2016). "Design and Rationale of the Best Endovascular Versus Best Surgical Therapy for Patients With Critical Limb Ischemia (BEST-CLI) Trial". Journal of the American Heart Association. 5 (7): e003219. doi:10.1161/JAHA.116.003219. PMC 5015366. PMID 27402237.
- Popplewell MA, Davies H, Jarrett H, Bate G, Grant M, Patel S, et al. (January 2016). "Bypass versus angio plasty in severe ischaemia of the leg - 2 (BASIL-2) trial: study protocol for a randomised controlled trial". Trials. 17: 11. doi:10.1186/s13063-015-1114-2. PMC 4704263. PMID 26739146.
- "Gene Therapy for PAD Approved". December 6, 2011. Archived from the original on September 3, 2015. Retrieved August 5, 2015.
- Deev RV, Bozo IY, Mzhavanadze ND, Voronov DA, Gavrilenko AV, Chervyakov YV, et al. (September 2015). "pCMV-vegf165 Intramuscular Gene Transfer is an Effective Method of Treatment for Patients With Chronic Lower Limb Ischemia". Journal of Cardiovascular Pharmacology and Therapeutics. 20 (5): 473–482. doi:10.1177/1074248415574336. PMID 25770117. S2CID 13443907.
External links
- "Peripheral Arterial Disease" at the National Heart, Lung and Blood Institute
- Peripheral Arterial Disease (P.A.D.) at the American College of Foot and Ankle Surgeons
- Gerhard-Herman MD, Gornik HL, Barrett C, Barshes NR, Corriere MA, Drachman DE, et al. (March 2017). "2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines". Circulation. 135 (12): e686–e725. doi:10.1161/CIR.0000000000000470. PMC 5479414. PMID 27840332.