Prostate-specific antigen
Prostate-specific antigen (PSA), also known as gamma-seminoprotein or kallikrein-3 (KLK3), P-30 antigen, is a glycoprotein enzyme encoded in humans by the KLK3 gene. PSA is a member of the kallikrein-related peptidase family and is secreted by the epithelial cells of the prostate gland.
| KLK3 | |||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||
| Identifiers | |||||||||||||||||||||||||||||||||||||||||||||||||||
| Aliases | KLK3, APS, KLK2A1, PSA, hK3, kallikrein related peptidase 3, Prostate Specific Antigen | ||||||||||||||||||||||||||||||||||||||||||||||||||
| External IDs | OMIM: 176820 MGI: 97320 HomoloGene: 68141 GeneCards: KLK3 | ||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||
| Wikidata | |||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||


PSA is produced for the ejaculate, where it liquefies semen in the seminal coagulum and allows sperm to swim freely.[5] It is also believed to be instrumental in dissolving cervical mucus, allowing the entry of sperm into the uterus.[6]
PSA is present in small quantities in the serum of men with healthy prostates, but is often elevated in the presence of prostate cancer or other prostate disorders.[7] PSA is not uniquely an indicator of prostate cancer, but may also detect prostatitis or benign prostatic hyperplasia.[8]
Medical diagnostic uses
Screening
Clinical practice guidelines for prostate cancer screening vary and are controversial, in part due to uncertainty as to whether the benefits of screening ultimately outweigh the risks of overdiagnosis and overtreatment.[9] In the United States, the Food and Drug Administration (FDA) has approved the PSA test for annual screening of prostate cancer in men of age 50 and older. The patient is required to be informed of the risks and benefits of PSA testing prior to performing the test.
In the United Kingdom, the National Health Service (NHS) as of 2018 does not mandate, nor advise for PSA test, but allows patients to decide based on their doctor's advice.[10] The NHS does not offer general PSA screening, for similar reasons.[11]
PSA levels between 4ng/mL to 10 ng/mL (nanograms per milliliter) are considered to be suspicious, and consideration should be given to confirming the abnormal PSA with a repeat test. If indicated, prostate biopsy is performed to obtain a tissue sample for histopathological analysis.
While PSA testing may help 1 in 1,000 avoid death due to prostate cancer, 4 to 5 in 1,000 would die from prostate cancer after 10 years even with screening. This means that PSA screening may reduce mortality from prostate cancer by up to 25%. Expected harms include anxiety for 100 – 120 receiving false positives, biopsy pain, and other complications from biopsy for false positive tests.
Use of PSA screening tests is also controversial due to questionable test accuracy. The screening can present abnormal results even when a man does not have cancer (known as a false-positive result), or normal results even when a man does have cancer (known as a false-negative result).[12] False-positive test results can cause confusion and anxiety in men, and can lead to unnecessary prostate biopsies, a procedure which causes risk of pain, infection, and hemorrhage. False-negative results can give men a false sense of security, though they may actually have cancer.
Of those found to have prostate cancer, overtreatment is common because most cases of prostate cancer are not expected to cause any symptoms due to low rate of growth of the prostate tumor. Therefore, many will experience the side effects of treatment, such as for every 1000 men screened, 29 will experience erectile dysfunction, 18 will develop urinary incontinence, two will have serious cardiovascular events, one will develop pulmonary embolus or deep venous thrombosis, and one perioperative death. Since the expected harms relative to risk of death are perceived by patients as minimal, men found to have prostate cancer usually (up to 90% of cases) elect to receive treatment.[13][14][15]
Risk stratification and staging
Men with prostate cancer may be characterized as low, intermediate, or high risk for having/developing metastatic disease or dying of prostate cancer. PSA level is one of three variables on which the risk stratification is based; the others are the grade of prostate cancer (Gleason grading system) and the stage of cancer based on physical examination and imaging studies. D'Amico criteria for each risk category are:[16]
- Low risk: PSA < 10, Gleason score ≤ 6, AND clinical stage ≤ T2a
- Intermediate risk: PSA 10-20, Gleason score 7, OR clinical stage T2b/c
- High risk: PSA > 20, Gleason score ≥ 8, OR clinical stage ≥ T3
Given the relative simplicity of the 1998 D'Amico criteria (above), other predictive models of risk stratification based on mathematical probability constructs exist or have been proposed to allow for better matching of treatment decisions with disease features.[17] Studies are being conducted into the incorporation of multiparametric MRI imaging results into nomograms that rely on PSA, Gleason grade, and tumor stage.[18]
Post-treatment monitoring
PSA levels are monitored periodically (e.g., every 6–36 months) after treatment for prostate cancer – more frequently in patients with high-risk disease, less frequently in patients with lower-risk disease. If surgical therapy (i.e., radical prostatectomy) is successful at removing all prostate tissue (and prostate cancer), PSA becomes undetectable within a few weeks. A subsequent rise in PSA level above 0.2 ng/mL[19] L is generally regarded as evidence of recurrent prostate cancer after a radical prostatectomy; less commonly, it may simply indicate residual benign prostate tissue.
Following radiation therapy of any type for prostate cancer, some PSA levels might be detected, even when the treatment ultimately proves to be successful. This makes interpreting the relationship between PSA levels and recurrence/persistence of prostate cancer after radiation therapy more difficult. PSA levels may continue to decrease for several years after radiation therapy. The lowest level is referred to as the PSA nadir. A subsequent increase in PSA levels by 2.0 ng/mL above the nadir is the currently accepted definition of prostate cancer recurrence after radiation therapy.
Recurrent prostate cancer detected by a rise in PSA levels after curative treatment is referred to as a "biochemical recurrence". The likelihood of developing recurrent prostate cancer after curative treatment is related to the pre-operative variables described in the preceding section (PSA level and grade/stage of cancer). Low-risk cancers are the least likely to recur, but they are also the least likely to have required treatment in the first place.
Prostatitis
PSA levels increase in the setting of prostate infection/inflammation (prostatitis), often markedly (> 100).
Forensic identification of semen
PSA was first identified by researchers attempting to find a substance in seminal fluid that would aid in the investigation of rape cases.[20] PSA is used to indicate the presence of semen in forensic serology.[21] The semen of adult males has PSA levels far in excess of those found in other tissues; therefore, a high level of PSA found in a sample is an indicator that semen may be present. Because PSA is a biomarker that is expressed independently of spermatozoa, it remains useful in identifying semen from vasectomized and azoospermic males.[22]
PSA can also be found at low levels in other body fluids, such as urine and breast milk, thus setting a high minimum threshold of interpretation to rule out false positive results and conclusively state that semen is present.[23] While traditional tests such as crossover electrophoresis have a sufficiently low sensitivity to detect only seminal PSA, newer diagnostics tests developed from clinical prostate cancer screening methods have lowered the threshold of detection down to 4 ng/mL.[24] This level of antigen has been shown to be present in the peripheral blood of males with prostate cancer, and rarely in female urine samples and breast milk.[23]
No studies have been performed to assess the PSA levels in the tissues and secretions of pre-pubescent children. Therefore, the presence of PSA from a high sensitivity (4 ng/mL) test cannot conclusively identify the presence of semen, so care must be taken with the interpretation of such results.
Sources
PSA is produced in the epithelial cells of the prostate, and can be demonstrated in biopsy samples or other histological specimens using immunohistochemistry. Disruption of this epithelium, for example in inflammation or benign prostatic hyperplasia, may lead to some diffusion of the antigen into the tissue around the epithelium, and is the cause of elevated blood levels of PSA in these conditions.[25]
More significantly, PSA remains present in prostate cells after they become malignant. Prostate cancer cells generally have variable or weak staining for PSA, due to the disruption of their normal functioning. Thus, individual prostate cancer cells produce less PSA than healthy cells; the raised serum levels in prostate cancer patients is due to the greatly increased number of such cells, not their individual activity. In most cases of prostate cancer, though, the cells remain positive for the antigen, which can then be used to identify metastasis. Since some high-grade prostate cancers may be entirely negative for PSA, however, histological analysis to identify such cases usually uses PSA in combination with other antibodies, such as prostatic acid phosphatase and CD57.[25]
Mechanism of action
The physiological function of KLK3 is the dissolution of the coagulum, the sperm-entrapping gel composed of semenogelins and fibronectin. Its proteolytic action is effective in liquefying the coagulum so that the sperm can be liberated. The activity of PSA is well regulated. In the prostate, it is present as an inactive pro-form, which is activated through the action of KLK2, another kallikrein-related peptidase. In the prostate, zinc ion concentrations are 10 times higher than in other bodily fluids. Zinc ions have a strong inhibitory effect on the activity of PSA and on that of KLK2, so that PSA is totally inactive.[26]
Further regulation is achieved through pH variations. Although its activity is increased by higher pH, the inhibitory effect of zinc also increases. The pH of semen is slightly alkaline and the concentrations of zinc are high. On ejaculation, semen is exposed to the acidic pH of the vagina, due to the presence of lactic acid. In fertile couples, the final vaginal pH after coitus approaches the 6-7 levels, which coincides well with reduced zinc inhibition of PSA. At these pH levels, the reduced PSA activity is countered by a decrease in zinc inhibition. Thus, the coagulum is slowly liquefied, releasing the sperm in a well-regulated manner.
Biochemistry
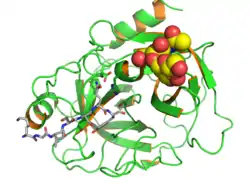
Prostate-specific antigen (PSA, also known as kallikrein III, seminin, semenogelase, γ-seminoprotein and P-30 antigen) is a 34-kD glycoprotein produced almost exclusively by the prostate gland. It is a serine protease (EC 3.4.21.77) enzyme, the gene of which is located on the 19th chromosome (19q13) in humans.[27]
History
The discovery of prostate-specific antigen (PSA) is beset with controversy; as PSA is present in prostatic tissue and semen, it was independently discovered and given different names, thus adding to the controversy.[28]
Flocks was the first to experiment with antigens in the prostate[29] and 10 years later Ablin reported the presence of precipitation antigens in the prostate.[30]
In 1971, Mitsuwo Hara characterized a unique protein in the semen fluid, gamma-seminoprotein. Li and Beling, in 1973, isolated a protein, E1, from human semen in an attempt to find a novel method to achieve fertility control.[31][32]
In 1978, Sensabaugh identified semen-specific protein p30, but proved that it was similar to E1 protein, and that prostate was the source.[33] In 1979, Wang purified a tissue-specific antigen from the prostate ('prostate antigen').[34]
PSA was first measured quantitatively in the blood by Papsidero in 1980,[35] and Stamey carried out the initial work on the clinical use of PSA as a marker of prostate cancer.[28]
Serum levels
PSA is normally present in the blood at very low levels. The reference range of less than 4 ng/mL for the first commercial PSA test, the Hybritech Tandem-R PSA test released in February 1986, was based on a study that found 99% of 472 apparently healthy men had a total PSA level below 4 ng/mL.[36]
Increased levels of PSA may suggest the presence of prostate cancer. However, prostate cancer can also be present in the complete absence of an elevated PSA level, in which case the test result would be a false negative.[37]
Obesity has been reported to reduce serum PSA levels.[38] Delayed early detection may partially explain worse outcomes in obese men with early prostate cancer.[39] After treatment, higher BMI also correlates to higher risk of recurrence.[40]
PSA levels can be also increased by prostatitis, irritation, benign prostatic hyperplasia (BPH), and recent ejaculation,[41][42] producing a false positive result. Digital rectal examination (DRE) has been shown in several studies[43] to produce an increase in PSA. However, the effect is clinically insignificant, since DRE causes the most substantial increases in patients with PSA levels already elevated over 4.0 ng/mL.
The "normal" reference ranges for prostate-specific antigen increase with age, as do the usual ranges in cancer, (per associated table).[44][45]
| Age | 40 - 49 | 50 - 59 | 60 - 69 | 70-79 | years | ||||
|---|---|---|---|---|---|---|---|---|---|
| Cancer | No cancer | Cancer | No cancer | Cancer | No cancer | Cancer | No cancer | ||
| 5th percentile | 0.4[44] | 0.3[44] | 1.2[44] | 0.3[44] | 1.7[44] | 0.3[44] | 2.3[44] | 0.4[44] | ng/mL or µg/L |
| 95th percentile Non-African-American | 163.0[44] | 1.2 - 2.9[45] | 372.5[44] | 2.07 - 4.7[45] | 253.2[44] | 2.8 - 7.2 | 613.2[44] | 4.0 - 9.0[45] | |
| 95th percentile African-American | 2.4 - 2.7[45] | 4.4 - 6.5[45] | 6.7 - 11[45] | 7.7 - 13[45] | |||||
PSA velocity
Despite earlier findings,[46] recent research suggests that the rate of increase of PSA (e.g. >0.35 ng/mL/yr, the 'PSA velocity'[47]) is not a more specific marker for prostate cancer than the serum level of PSA.[48]
However, the PSA rate of rise may have value in prostate cancer prognosis. Men with prostate cancer whose PSA level increased by more than 2.0 ng per milliliter during the year before the diagnosis of prostate cancer have a higher risk of death from prostate cancer despite undergoing radical prostatectomy.[49] PSA velocity (PSAV) was found in a 2008 study to be more useful than the PSA doubling time (PSA DT) to help identify those men with life-threatening disease before start of treatment.[50]
Men who are known to be at risk for prostate cancer, and who decide to plot their PSA values as a function of time (i.e., years), may choose to use a semi-log plot. An exponential growth in PSA values appears as a straight line[51] on a semi-log plot, so that a new PSA value significantly above the straight line signals a switch to a new and significantly higher growth rate,[51] i.e., a higher PSA velocity.
Free PSA
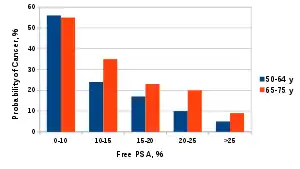
Most PSA in the blood is bound to serum proteins. A small amount is not protein-bound and is called 'free PSA'. In men with prostate cancer, the ratio of free (unbound) PSA to total PSA is decreased. The risk of cancer increases if the free to total ratio is less than 25%. (See graph) The lower the ratio is, the greater the probability of prostate cancer. Measuring the ratio of free to total PSA appears to be particularly promising for eliminating unnecessary biopsies in men with PSA levels between 4 and 10 ng/mL.[53] However, both total and free PSA increase immediately after ejaculation, returning slowly to baseline levels within 24 hours.[41]
Inactive PSA
The PSA test in 1994 failed to differentiate between prostate cancer and benign prostate hyperplasia (BPH) and the commercial assay kits for PSA did not provide correct PSA values.[54] Thus with the introduction of the ratio of free-to-total PSA, the reliability of the test has improved. Measuring the activity of the enzyme could add to the ratio of free-to-total PSA and further improve the diagnostic value of test.[55] Proteolytically active PSA has been shown to have an anti-angiogenic effect [56] and certain inactive subforms may be associated with prostate cancer, as shown by MAb 5D3D11, an antibody able to detect forms abundantly represented in sera from cancer patients.[57] The presence of inactive proenzyme forms of PSA is another potential indicator of disease.[58]
Complexed PSA
PSA exists in serum in the free (unbound) form and in a complex with alpha 1-antichymotrypsin; research has been conducted to see if measurements of complexed PSA are more specific and sensitive biomarkers for prostate cancer than other approaches.[59][60]
PSA in other biologic fluids and tissues
| Fluid | PSA (ng/mL) |
|---|---|
| semen | 200,000 - 5.5 million |
| amniotic fluid | 0.60 - 8.98 |
| breast milk | 0.47 - 100 |
| saliva | 0 |
| female urine | 0.12 - 3.72 |
| female serum | 0.01 - 0.53 |
The term prostate-specific antigen is a misnomer: it is an antigen but is not specific to the prostate. Although present in large amounts in prostatic tissue and semen, it has been detected in other body fluids and tissues.[23]
In women, PSA is found in female ejaculate at concentrations roughly equal to that found in male semen.[61] Other than semen and female ejaculate, the greatest concentrations of PSA in biological fluids are detected in breast milk and amniotic fluid. Low concentrations of PSA have been identified in the urethral glands, endometrium, normal breast tissue and salivary gland tissue. PSA also is found in the serum of women with breast, lung, or uterine cancer and in some patients with renal cancer.[62]
Tissue samples can be stained for the presence of PSA in order to determine the origin of malignant cells that have metastasized.[63]
Interactions
Prostate-specific antigen has been shown to interact with protein C inhibitor.[64][65] Prostate-specific antigen interacts with and activates the vascular endothelial growth factors VEGF-C and VEGF-D, which are involved in tumor angiogenesis and in the lymphatic metastasis of tumors.[66]
See also
References
- GRCh38: Ensembl release 89: ENSG00000142515 - Ensembl, May 2017
- GRCm38: Ensembl release 89: ENSMUSG00000066513 - Ensembl, May 2017
- "Human PubMed Reference:". National Center for Biotechnology Information, U.S. National Library of Medicine.
- "Mouse PubMed Reference:". National Center for Biotechnology Information, U.S. National Library of Medicine.
- Balk SP, Ko YJ, Bubley GJ (January 2003). "Biology of prostate-specific antigen". Journal of Clinical Oncology. 21 (2): 383–391. doi:10.1200/JCO.2003.02.083. PMID 12525533.
- Hellstrom WJG, ed. (1999). "Chapter 8: What is the prostate and what is its function?". American Society of Andrology Handbook. San Francisco: American Society of Andrology. ISBN 978-1-891276-02-6.
- Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino PT, Flanigan RC, et al. (May 1994). "Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men". The Journal of Urology. 151 (5): 1283–1290. doi:10.1016/S0022-5347(17)35233-3. PMID 7512659.
- Velonas VM, Woo HH, dos Remedios CG, Assinder SJ (May 2013). "Current status of biomarkers for prostate cancer". International Journal of Molecular Sciences. 14 (6): 11034–11060. doi:10.3390/ijms140611034. PMC 3709717. PMID 23708103.
- Gomella LG, Liu XS, Trabulsi EJ, Kelly WK, Myers R, Showalter T, et al. (October 2011). "Screening for prostate cancer: the current evidence and guidelines controversy". The Canadian Journal of Urology. 18 (5): 5875–5883. PMID 22018148.
- "Should I have a PSA test?". NHS Choices. 27 February 2018. Archived from the original on 28 February 2018.
- "Prostate cancer - PSA testing - NHS Choices". NHS Choices. 3 January 2015.
- "Can Prostate Cancer Be Found Early?". www.cancer.org. Retrieved 17 January 2020.
- "Talking With Your Patients About Screening for Prostate Cancer" (PDF). Archived from the original (PDF) on 11 October 2014. Retrieved 2 July 2012.
- Grossman DC, Curry SJ, Owens DK, Bibbins-Domingo K, Caughey AB, Davidson KW, et al. (May 2018). "Screening for Prostate Cancer: US Preventive Services Task Force Recommendation Statement". JAMA. 319 (18): 1901–1913. doi:10.1001/jama.2018.3710. PMID 29801017.
- Fenton JJ, Weyrich MS, Durbin S, Liu Y, Bang H, Melnikow J (May 2018). "Prostate-Specific Antigen-Based Screening for Prostate Cancer: Evidence Report and Systematic Review for the US Preventive Services Task Force". JAMA. 319 (18): 1914–1931. doi:10.1001/jama.2018.3712. PMID 29801018.
- D'Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA, et al. (September 1998). "Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer". JAMA. 280 (11): 969–974. doi:10.1001/jama.280.11.969. PMID 9749478.
- Rodrigues G, Warde P, Pickles T, Crook J, Brundage M, Souhami L, Lukka H (April 2012). "Pre-treatment risk stratification of prostate cancer patients: A critical review". Canadian Urological Association Journal. 6 (2): 121–127. doi:10.5489/cuaj.11085. PMC 3328553. PMID 22511420.
- Sperling D. "mpMRI improves the accuracy of the Partin tables and other nomograms". Sperling Prostate Center. Retrieved 31 March 2016.
- Freedland SJ, Sutter ME, Dorey F, Aronson WJ (February 2003). "Defining the ideal cutpoint for determining PSA recurrence after radical prostatectomy. Prostate-specific antigen". Urology. 61 (2): 365–369. doi:10.1016/s0090-4295(02)02268-9. PMID 12597949.
- Hara M, Inorre T, Fukuyama T (1971). "Some physicochemical characteristics of gamma-seminoprotein, an antigenic component specific for human seminal plasma". Jpn J Legal Med. 25: 322–324.
- Gartside BO, Brewer KJ, Strong CL (April 2003). "Estimation of Prostate-Specific Antigen (PSA) Extraction Efficiency from Forensic Samples Using the Serateca PSA Semiquant Semiquantitative Membrane Test". Forensic Science Communications. 5 (2). Archived from the original on 9 April 2008. Retrieved 11 May 2008.
- Hochmeister MN, Budowle B, Rudin O, Gehrig C, Borer U, Thali M, Dirnhofer R (September 1999). "Evaluation of prostate-specific antigen (PSA) membrane test assays for the forensic identification of seminal fluid". Journal of Forensic Sciences. 44 (5): 1057–1060. doi:10.1520/JFS12042J. PMID 10486959.
- Laux DL, Custis SE. Forensic Detection of Semen III. Detection of PSA Using Membrane Based Tests: Sensitivity Issues with Regards to the Presence of PSA in Other Body Fluids (PDF) (Report). Midwestern Association of Forensic Scientists. Archived from the original (PDF) on 27 August 2005. Retrieved 11 May 2008.
- Hochmeister MN, Budowle B, Rudin O, Gehrig C, Borer U, Thali M, Dirnhofer R (September 1999). "Evaluation of prostate-specific antigen (PSA) membrane test assays for the forensic identification of seminal fluid". Journal of Forensic Sciences. 44 (5): 1057–1060. doi:10.1520/JFS12042J. PMID 10486959. Archived from the original on 24 October 2004.
- Leong AS, Cooper K, Leong FJ (2003). Manual of Diagnostic Cytology (2nd ed.). Greenwich Medical Media, Ltd. pp. 79–80. ISBN 978-1-84110-100-2.
- Hara M, Kimura H (May 1989). "Two prostate-specific antigens, gamma-seminoprotein and beta-microseminoprotein". The Journal of Laboratory and Clinical Medicine. 113 (5): 541–548. PMID 2654306.
- Lilja H (November 2003). "Biology of prostate-specific antigen". Urology. 62 (5 Suppl 1): 27–33. doi:10.1016/S0090-4295(03)00775-1. PMID 14607215.
- Rao AR, Motiwala HG, Karim OM (January 2008). "The discovery of prostate-specific antigen". BJU International. 101 (1): 5–10. doi:10.1111/j.1464-410X.2007.07138.x. PMID 17760888. S2CID 27307190.
- Flocks RH, Boatman DL, Hawtrey CE (November 1972). "Tissue specific isoantigens in the dog prostate". Investigative Urology. 10 (3): 215–220. PMID 4629646.
- Ablin RJ, Soanes WA, Gonder MJ (July 1969). "Immunologic studies of the prostate. A review". International Surgery. 52 (1): 8–21. PMID 4977978.
- Li TS, Beling CG (February 1973). "Isolation and characterization of two specific antigens of human seminal plasma". Fertility and Sterility. 24 (2): 134–144. doi:10.1016/S0015-0282(16)39496-1. PMID 4631694.
- Li TS, Beling CG (October 1974). "The effect of antibodies to two human seminal plasma-specific antigens on human sperm". Fertility and Sterility. 25 (10): 851–856. doi:10.1016/S0015-0282(16)40691-6. PMID 4213812.
- Sensabaugh GF (January 1978). "Isolation and characterization of a semen-specific protein from human seminal plasma: a potential new marker for semen identification". Journal of Forensic Sciences. 23 (1): 106–115. doi:10.1520/JFS10659J. PMID 744956.
- Wang MC, Valenzuela LA, Murphy GP, Chu TM (September 1979). "Purification of a human prostate specific antigen". Investigative Urology. 17 (2): 159–163. PMID 89106.
- Kuriyama M, Wang MC, Papsidero LD, Killian CS, Shimano T, Valenzuela L, et al. (December 1980). "Quantitation of prostate-specific antigen in serum by a sensitive enzyme immunoassay". Cancer Research. 40 (12): 4658–4662. PMID 6159971.
- Gina K (30 May 2004). "It Was Medical Gospel, but It Wasn't True". The New York Times. p. 47.
- Thompson IM, Pauler DK, Goodman PJ, Tangen CM, Lucia MS, Parnes HL, et al. (May 2004). "Prevalence of prostate cancer among men with a prostate-specific antigen level < or =4.0 ng per milliliter". The New England Journal of Medicine. 350 (22): 2239–2246. doi:10.1056/NEJMoa031918. PMID 15163773. S2CID 3747157.
- Carter HB (May 2004). "Prostate cancers in men with low PSA levels--must we find them?". The New England Journal of Medicine. 350 (22): 2292–2294. doi:10.1056/NEJMe048003. PMC 3474980. PMID 15163780.
- Myrtle JF, Klimley PG, Ivor L, Bruni JF (1986). "Clinical utility of prostate specific antigen (PSA) in the management of prostate cancer". Advances in Cancer Diagnostics. San Diego: Hybritech Inc.
- Mytrle JF, Ivor L (1989). "Measurement of Prostate-Specific Antigen (PSA) in Serum by a Two-Site Immunometric Method (Hybritech Tandem-R/Tandem-E PSA)". In Catalona WJ, Coffey DS, Karr JP (eds.). Clinical Aspects of Prostate Cancer. Assessment of New Diagnostic and Management Procedures. Proceedings of a workshop of the Prostate Cancer Working Group of the National Cancer Institute's Organ Systems Program, held October 16–19, 1988 at Prout's Neck, Maine, U.S.A. New York: Elsevier. pp. 161–71. ISBN 978-0-444-01514-3.
- Mytrle JF (1989). "Normal Levels of Prostate-Specific Antigen (PSA)". In Catalona WJ, Coffey DS, Karr JP (eds.). Clinical Aspects of Prostate Cancer. Assessment of New Diagnostic and Management Procedures. Proceedings of a workshop of the Prostate Cancer Working Group of the National Cancer Institute's Organ Systems Program, held October 16–19, 1988 at Prout's Neck, Maine, U.S.A. New York: Elsevier. pp. 183–9. ISBN 978-0-444-01514-3.
- Catalona WJ, Smith DS, Ratliff TL, Dodds KM, Coplen DE, Yuan JJ, et al. (April 1991). "Measurement of prostate-specific antigen in serum as a screening test for prostate cancer". The New England Journal of Medicine. 324 (17): 1156–1161. doi:10.1056/NEJM199104253241702. PMID 1707140.
- Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino PT, Flanigan RC, et al. (May 1994). "Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men". The Journal of Urology. 151 (5): 1283–1290. doi:10.1016/S0022-5347(17)35233-3. PMID 7512659.
- Thompson IM, Pauler DK, Goodman PJ, Tangen CM, Lucia MS, Parnes HL, et al. (May 2004). "Prevalence of prostate cancer among men with a prostate-specific antigen level < or =4.0 ng per milliliter". The New England Journal of Medicine. 350 (22): 2239–2246. doi:10.1056/NEJMoa031918. PMID 15163773. S2CID 3747157.
- Bañez LL, Hamilton RJ, Partin AW, Vollmer RT, Sun L, Rodriguez C, et al. (November 2007). "Obesity-related plasma hemodilution and PSA concentration among men with prostate cancer". JAMA. 298 (19): 2275–2280. doi:10.1001/jama.298.19.2275. PMID 18029831.
- Robert Dreicer (20 November 2007). "Why do obese men have lower PSA concentrations?". Journal Watch. 2007 (1120): 1. Archived from the original on 17 February 2008. Retrieved 27 April 2008.
- Cao Y, Ma J (April 2011). "Body mass index, prostate cancer-specific mortality, and biochemical recurrence: a systematic review and meta-analysis". Cancer Prevention Research. 4 (4): 486–501. doi:10.1158/1940-6207.CAPR-10-0229. PMC 3071449. PMID 21233290.
- Herschman JD, Smith DS, Catalona WJ (August 1997). "Effect of ejaculation on serum total and free prostate-specific antigen concentrations". Urology. 50 (2): 239–243. doi:10.1016/S0090-4295(97)00209-4. PMID 9255295. S2CID 46329694.
- Nadler RB, Humphrey PA, Smith DS, Catalona WJ, Ratliff TL (August 1995). "Effect of inflammation and benign prostatic hyperplasia on elevated serum prostate specific antigen levels". The Journal of Urology. 154 (2 Pt 1): 407–413. doi:10.1016/S0022-5347(01)67064-2. PMID 7541857.
- Crawford ED, Schutz MJ, Clejan S, Drago J, Resnick MI, Chodak GW, et al. (1992). "The effect of digital rectal examination on prostate-specific antigen levels". JAMA. 267 (16): 2227–2228. doi:10.1001/jama.267.16.2227. PMID 1372943.
Chybowski FM, Bergstralh EJ, Oesterling JE (July 1992). "The effect of digital rectal examination on the serum prostate specific antigen concentration: results of a randomized study". The Journal of Urology. 148 (1): 83–86. doi:10.1016/S0022-5347(17)36517-5. PMID 1377290.
Collins GN, Martin PJ, Wynn-Davies A, Brooman PJ, O'Reilly PH (May 1997). "The effect of digital rectal examination, flexible cystoscopy and prostatic biopsy on free and total prostate specific antigen, and the free-to-total prostate specific antigen ratio in clinical practice". The Journal of Urology. 157 (5): 1744–1747. doi:10.1016/S0022-5347(01)64849-3. PMID 9112518.
Tarhan F, Orçun A, Küçükercan I, Camursoy N, Kuyumcuoğlu U (December 2005). "Effect of prostatic massage on serum complexed prostate-specific antigen levels". Urology. 66 (6): 1234–1238. doi:10.1016/j.urology.2005.06.077. PMID 16360449. - Connolly D, Black A, Murray L, Gavin A, Keane P (2007). "798 Population Based Age-Specific Reference Ranges for PSA". European Urology Supplements. 6 (2): 222. doi:10.1016/S1569-9056(07)60793-3.
- Luboldt, Hans-Joachim; Schindler, Joachim F.; Rübben, Herbert (2007). "Age-Specific Reference Ranges for Prostate-Specific Antigen as a Marker for Prostate Cancer". EAU-EBU Update Series. 5 (1): 38–48. doi:10.1016/j.eeus.2006.10.003. ISSN 1871-2592.
- Carter HB, Pearson JD, Metter EJ, Brant LJ, Chan DW, Andres R, et al. (1992). "Longitudinal evaluation of prostate-specific antigen levels in men with and without prostate disease". JAMA. 267 (16): 2215–2220. doi:10.1001/jama.267.16.2215. PMC 3461837. PMID 1372942.
- "PSA Velocity Does Not Improve Prostate Cancer Detection". 13 April 2011. Retrieved 25 April 2015.
- Carter HB (April 2006). "Assessing risk: does this patient have prostate cancer?". Journal of the National Cancer Institute. 98 (8): 506–507. doi:10.1093/jnci/djj155. PMID 16622114.
- D'Amico AV, Chen MH, Roehl KA, Catalona WJ (July 2004). "Preoperative PSA velocity and the risk of death from prostate cancer after radical prostatectomy". The New England Journal of Medicine. 351 (2): 125–135. doi:10.1056/NEJMoa032975. PMID 15247353.
- Loeb S, Kettermann A, Ferrucci L, Landis P, Metter EJ, Carter HB (November 2008). "PSA doubling time versus PSA velocity to predict high-risk prostate cancer: data from the Baltimore Longitudinal Study of Aging". European Urology. 54 (5): 1073–1080. doi:10.1016/j.eururo.2008.06.076. PMC 2582974. PMID 18614274.
- "Semi-Log Transformations of Data". Archived from the original on 24 February 2016. Retrieved 4 March 2016.
{{cite web}}: CS1 maint: bot: original URL status unknown (link)(Archived by WebCite® at ) - Catalona WJ, Partin AW, Slawin KM, Brawer MK, Flanigan RC, Patel A, et al. (May 1998). "Use of the percentage of free prostate-specific antigen to enhance differentiation of prostate cancer from benign prostatic disease: a prospective multicenter clinical trial". JAMA. 279 (19): 1542–1547. doi:10.1001/jama.279.19.1542. PMID 9605898.
- Catalona WJ, Smith DS, Ornstein DK (May 1997). "Prostate cancer detection in men with serum PSA concentrations of 2.6 to 4.0 ng/mL and benign prostate examination. Enhancement of specificity with free PSA measurements". JAMA. 277 (18): 1452–1455. doi:10.1001/jama.277.18.1452. PMID 9145717.
- Wu JT (1994). "Assay for prostate specific antigen (PSA): problems and possible solutions". Journal of Clinical Laboratory Analysis. 8 (1): 51–62. doi:10.1002/jcla.1860080110. PMID 7513021. S2CID 13179006.
- "A bioelectronic assay for PSA activity".
- Mattsson JM, Valmu L, Laakkonen P, Stenman UH, Koistinen H (June 2008). "Structural characterization and anti-angiogenic properties of prostate-specific antigen isoforms in seminal fluid". The Prostate. 68 (9): 945–954. doi:10.1002/pros.20751. PMID 18386289. S2CID 30095129.
- Stura EA, Muller BH, Bossus M, Michel S, Jolivet-Reynaud C, Ducancel F (December 2011). "Crystal structure of human prostate-specific antigen in a sandwich antibody complex". Journal of Molecular Biology. 414 (4): 530–544. doi:10.1016/j.jmb.2011.10.007. PMID 22037582.
- Mikolajczyk SD, Catalona WJ, Evans CL, Linton HJ, Millar LS, Marker KM, et al. (June 2004). "Proenzyme forms of prostate-specific antigen in serum improve the detection of prostate cancer". Clinical Chemistry. 50 (6): 1017–1025. doi:10.1373/clinchem.2003.026823. PMID 15054080.
- Mikolajczyk SD, Marks LS, Partin AW, Rittenhouse HG (June 2002). "Free prostate-specific antigen in serum is becoming more complex". Urology. 59 (6): 797–802. doi:10.1016/S0090-4295(01)01605-3. PMID 12031356.
- Naya Y, Okihara K (May 2004). "Role of complexed PSA in the early detection of prostate cancer". Journal of the National Comprehensive Cancer Network. 2 (3): 209–212. doi:10.6004/jnccn.2004.0019. PMID 19795605.
- Wimpissinger F, Stifter K, Grin W, Stackl W (September 2007). "The female prostate revisited: perineal ultrasound and biochemical studies of female ejaculate". The Journal of Sexual Medicine. 4 (5): 1388–93, discussion 1393. doi:10.1111/j.1743-6109.2007.00542.x. PMID 17634056.
- Stanley A Brosman. eMedicine: Prostate-Specific Antigen. WebMD. Retrieved 11 May 2008.
- Chuang AY, DeMarzo AM, Veltri RW, Sharma RB, Bieberich CJ, Epstein JI (August 2007). "Immunohistochemical differentiation of high-grade prostate carcinoma from urothelial carcinoma". The American Journal of Surgical Pathology. 31 (8): 1246–1255. doi:10.1097/PAS.0b013e31802f5d33. PMID 17667550. S2CID 11535862.
- Christensson A, Lilja H (February 1994). "Complex formation between protein C inhibitor and prostate-specific antigen in vitro and in human semen". European Journal of Biochemistry. 220 (1): 45–53. doi:10.1111/j.1432-1033.1994.tb18597.x. PMID 7509746.
- Kise H, Nishioka J, Kawamura J, Suzuki K (May 1996). "Characterization of semenogelin II and its molecular interaction with prostate-specific antigen and protein C inhibitor". European Journal of Biochemistry. 238 (1): 88–96. doi:10.1111/j.1432-1033.1996.0088q.x. PMID 8665956.
- Jha SK, Rauniyar K, Chronowska E, Mattonet K, Maina EW, Koistinen H, et al. (May 2019). "KLK3/PSA and cathepsin D activate VEGF-C and VEGF-D". eLife. 8: –44478. doi:10.7554/eLife.44478. PMC 6588350. PMID 31099754.
Further reading
- De Angelis G, Rittenhouse HG, Mikolajczyk SD, Blair Shamel L, Semjonow A (2007). "Twenty Years of PSA: From Prostate Antigen to Tumor Marker". Reviews in Urology. 9 (3): 113–123. PMC 2002501. PMID 17934568.
- Henttu P, Vihko P (June 1994). "Prostate-specific antigen and human glandular kallikrein: two kallikreins of the human prostate". Annals of Medicine. 26 (3): 157–164. doi:10.3109/07853899409147884. PMID 7521173.
- Diamandis EP, Yousef GM, Luo LY, Magklara A, Obiezu CV (March 2000). "The new human kallikrein gene family: implications in carcinogenesis". Trends in Endocrinology and Metabolism. 11 (2): 54–60. doi:10.1016/S1043-2760(99)00225-8. PMID 10675891. S2CID 25806934.
- Lilja H (November 2003). "Biology of prostate-specific antigen". Urology. 62 (5 Suppl 1): 27–33. doi:10.1016/S0090-4295(03)00775-1. PMID 14607215.
External links
- "The Prostate-Specific Antigen (PSA) Test: Questions and Answers". National Cancer Institute. 21 March 2022.
- Prostate-Specific+Antigen at the U.S. National Library of Medicine Medical Subject Headings (MeSH)
- Overview of all the structural information available in the PDB for UniProt: P07288 (Prostate-specific antigen) at the PDBe-KB.