Sonodynamic therapy
Sonodynamic therapy (SDT) is a noninvasive treatment, often used for tumor irradiation, that utilizes a sonosensitizer and the deep penetration of ultrasound to treat lesions of varying depths by reducing target cell number and preventing future tumor growth.[1][2] Many existing cancer treatment strategies cause systemic toxicity or cannot penetrate tissue deep enough to reach the entire tumor; however, emerging ultrasound stimulated therapies could offer an alternative to these treatments with their increased efficiency, greater penetration depth, and reduced side effects. Sonodynamic therapy could be used to treat cancers and other diseases, such as atherosclerosis, and diminish the risk associated with other treatment strategies since it induces cytotoxic effects only when externally stimulated by ultrasound and only at the cancerous region, as opposed to the systemic administration of chemotherapy drugs.[3][4][5]
.jpg.webp)
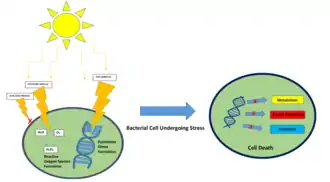
Reactive oxygen species (ROS) are an essential component of SDT as they provide the cytotoxicity of sonodynamic therapy; they are produced when ultrasound is coupled with a sensitizing drug and molecular oxygen.[1] Without ultrasound, the drug is not toxic. However, once the drug is exposed to ultrasound and molecular oxygen, it becomes toxic.[1] Photodynamic therapy, from which sonodynamic therapy was derived, uses a similar mechanism. Instead of ultrasound, light is used to activate the drug.[1] SDT allows the ultrasound to reach deeper into the tissue (to about 30 centimeters) compared to photodynamic therapy (PDT) since it can be highly focused.[1] This increased penetration depth ultimately means that SDT can be utilized to treat deeper, less accessible tumors and is more cost-effective than PDT.[6][1] Photodynamic therapy can be used in combination with sonodynamic therapy and is expanded upon in the Applications section of this article. Sonodynamic therapy can be used synergistically with other therapeutic methods such as drug-loaded microbubbles, nanoparticles, exosomes, liposomes, and genes for improved efficacy. Currently, SDT does not have any clinical products and acts as an adjuvant for the aforementioned therapeutic methods, but it has been explored for use in atherosclerosis and cancer treatment to reduce tumor size in breast, pancreas, liver, and spinal sarcomas. [7][3] [8][9][10] [11][12][13] [14][15][16]
Mechanism of Action
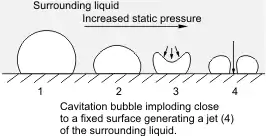
The mechanism of action for sonodynamic therapy is the use of low-intensity ultrasound through the use of focused mechanical waves to create a cytotoxic effect. However, SDT itself is non-thermal, non-toxic, and is able to non-invasively penetrate deep into tissue compared to other delivery methods such as photodynamic therapy. SDT is often performed alongside the use of a sonosensitizer such as porphyrin, phthalocyanines, xanthenes, and antitumor drugs.[17] Ultrasound waves are also classified as acoustic waves, and the effect they have on the tissue of application can be described by a process called cavitation. Cavitation occurs as a specific interaction between ultrasound and aqueous surroundings and causes gas bubbles to break upon exposure to particular ultrasonic parameters, thus promoting penetration of the therapeutic into the biological tissues by generating cavities near the edge of the membrane.[18][1] Cavitation can be broken down into stable and inertial cavitation. In stable cavitation, the oscillation of gas bubbles causes the environmental media to intermix.[1] In inertial cavitation, gas bubbles increase in volume and almost reach their resonance volume, swelling before aggressively collapsing.[1] The implosion of vesicles results in a drastic temperature and pressure change, thereby increasing the cell membrane's permeability to various drugs.[1][19] Microbubbles are created by the acoustic waves from the ultrasound that expand and collapse, releasing energy, bringing the sonosensitizer into an excited state, and generating a ROS. The cavitation of this gas bubble can form the ROS with different methodologies such as sonoluminescence and pyrolysis.[1] Apoptosis results from the formation of ROS and mechanical forces of SDT through membrane disruption in a process called lipid peroxidation. Necrosis is also a potential result of SDT.
The influence of sonoluminescence on SDT and ROS has not been fully elaborated within literature.[1] Currently, it is understood that sonoluminescence allows the emission of light upon bubble collapse which can activate sensitizers. A study by Hachimine et al. highlights the use of SDT as a method to activate a low photosensitive sonosensitizer, DCPH-P-Na(I), for cancer that is too deep within the tissue to combat utilizing PDT without skin irritation.[1][20] Pyrolysis raises the surrounding temperature, enhances the cavitation process, breaks down the sensitizer, generating free radicals, and the free radicals interact within their environment to generate ROS.[1] For both methods, the importance of the singlet oxygen compared to the hydroxyl radical to induce cytotoxicity has been highlighted.[1][20][21] While other studies[1][22][23] have found the singlet oxygen to not have a substantial effect. Overall, both of these methodologies lack significant breadth in literature to fully explain their role in ROS formation. However, literature has shown success in their analysis and application.[1][4][24]
Sonoluminescence
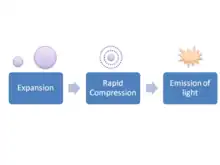
Two primary mechanisms of ROS generation exist in sonodynamic therapy: sonoluminescence and pyrolysis.[1] Sonoluminescence occurs when ultrasound produces light after irradiating an aqueous solution[1][25] The exact mechanism with which light is produced remains unclear. However, it is suggested that inertial cavitation is a key element for this process.[1][26] Other studies also indicate the potential role of stable cavitation[1][27]
Pyrolysis
Pyrolysis is believed to occur when inertial cavitation induces an extreme temperature increase, degrades the sonosensitizers, thus producing free radicals that can react and ultimately produce ROS necessary for SDT.[1][28] The localized temperature increase assists in the inertial cavitation and breakdown of the sonosensitizer in order to create ROS. The pyrolysis within the cavitation bubbles will produce H+ and OH- via weak bonding within the solute molecule.[1][19]
Lipid Peroxidation
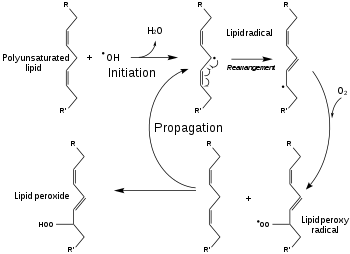
In addition to chemical methods, mechanical properties of the acoustic wave generated from the ultrasound can assist in initiating cytotoxic effects. This occurs through disruption of the membrane with a hydrophobic sonosensitizer. The mechanical disruption of the membrane causes a process called lipid peroxidation and adjustments to the cell membrane can change cell drug permeability.[1][29] Both sonochemical and sonomechanical methodologies are used to generate ROS and release cargo from vesicles for applications such as tumor targeting.
Apoptosis
Low intensity ultrasound has been shown within past literature to induce apoptotic effects within surrounding cells. It has been found that it is not the initial ROS that causes apoptosis within the cells, but the free radicals within the mitochondria. In a study by Honda et al., it was determined that the mitochondria-caspase pathway is responsible for apoptosis through the increase of intracellular calcium.[1][30] Outside of ROS induced apoptosis, cavitation is another factor involved within apoptosis of surrounding cells. Both cavitation types are able to induce apoptosis through damage to the membrane. Conditions such as frequency, duty cycle, pulse, and intensity can be manipulated to optimize cell death conditions such as necrosis, lysis, or apoptosis.[31][24][32]
Autophagy
This method of cell death can occur by cell organelles becoming entrapped into autophagosomes that combine with lysosomes. Continuation of this process will lead to cell death and autophagy inhibitors or promoters can be controlled to encourage or discourage cell death and uptake of chemotherapeutics.[1]
Sonosensitizers
Sonosensitizers, or sonosensitizing therapeutics, are the primary element of SDT and can be tailored to treat various cancers and generate different effects.[2] These therapeutics, often involving the use of porphyrin or xanthene, will initiate a toxic effect via the ROS upon exposure to ultrasound.
Porphyrin-based sensitizers
Porphyrin-based sensitizers, initially used as a photosensitizer in PDT, are fairly hydrophobic molecules derived from hematoporphyrin.[1] Single oxygen atoms or hydroxyl radicals are produced by porphyrin-based sensitizers upon exposure to ultrasound or light, providing the cytotoxic effects desired with sonodynamic and photodynamic therapies.[1] However, the result of porphyrin-based sensitizers is not as local as desired for sonodynamic therapy since they are also located in non-targeted tissue between the tumor and the ultrasound emitter.[1]
Xanthene-based sensitizers

Xanthene-based sensitizers, on the other hand, have shown successful cytotoxicity in vitro by producing reactive oxygen species after being triggered by ultrasound.[1] More research is necessary to improve its potential in vivo performance since it is quickly processed by the liver and cleared from the body.[1] Rose Bengal is a commonly used xanthene-based sonosensitizer.[1]
Additional sensitizers
Other sensitizers that have been investigated for their potential in sonodynamic therapy (and have also been used previously in PDT) include acridine orange, methylene blue, curcumin, and indocyanine green.[1] A study by Suzuki et al. used acridine orange, a fluorescent cationic dye that can insert itself into nucleic acids, for treating sarcoma 180 cells with ultrasound and demonstrated that reactive oxygen species are a critical element of SDT considering that their absence decreased the efficacy of SDT.[33] Similar to the previous study, a recent study by Komori et al. utilized ultrasound coupled with methylene blue (a phenothiazine dye commonly used in PDT that exhibits low toxicity) to irradiate sarcoma 180 cells and found that methylene blue was an effective sonosensitizer in decreasing cell viability.[34] Interestingly, curcumin is a spice that also can act as a sensitizer for PDT and SDT.[1] In a study by Waksman et al., curcumin was able to impact macrophages, which are important for development of plaques found in atherosclerosis patients, thus reducing the amount of plaque in an animal model.[35] These findings along with other research indicate that curcumin sensitizers could be used in SDT cancer treatments. Indocyanine green is a dye that absorbs near infrared wavelengths and is another sensitizer that has been shown to reduce cell viability when coupled with ultrasound and/or light.[36] An in vivo study demonstrated that treating a mouse tumor model with indocyanine green coupled with ultrasound and light resulted in a 98% reduction in tumor volume by 27 days after treatment.[36]
| Name | Structure |
|---|---|
| Phthalocyanine |  Phthalocyanine |
| Indocyanine Green |  Indocyanine Green |
| Phenothiazine |  Phenothiazine |
| Curcumin-keto | .svg.png.webp) Curcumin_structure_(Keto) |
| Curcumin-enol |  Curcumin-enol |
Carriers
As aforementioned, sonosensitizers are often used in conjunction with different drug carriers such as microbubbles, nanobubbles, liposomes, and exosomes to improve therapeutic agent concentration and penetration.[18]
Liposomes

Liposomes are a common vehicle in drug delivery and specifically for the treatment of cancer. Liposomes contain a phospholipid bilayer. It is prevalent due to its ability to penetrate leaky vasculature and poor lymphatic drainage within tumors for enhanced permeability retention.[37] These drug carriers can encapsulate hydrophobic and lipophilic molecules within their lipid bilayer and can be made naturally or synthetically.[38][39] In addition, liposomes can entrap hydrophilic molecules in their hydrophilic core.[38] Compared to the common cancer treatment chemotherapy, drugs loaded into liposomes allow for decreased systemic toxicity and a potential increase in the efficacy of targeted delivery.[18] Success with liposomes as drug delivery systems has been shown both in vivo and in vitro.[38] A study by Liu et al. showed that liposomes can be used alongside SDT to trigger the release of drugs via oxidation of the lipid components.[40] Another study by Ninomiya et al. utilized nanoemulsion droplets exposed to ultrasonic waves for the formation of larger gas bubbles to disrupt the liposome membrane for drug release. Many properties and elements of liposomes can be altered for their specific purpose and to increase effectiveness, particularly their ability to travel in the blood and interact with cells and tissues in the body.[38] These elements include their diameter, charge, arrangement, as well as the makeup of their membranes.[38] Dai et al. proposed the incorporation of sonosensitizers with liposomes to enhance target specificity.[18] Since SDT stimulates cancerous tissues to absorb and retain sonosentizers followed by activation with extracorporeal ultrasound, Dai et al. investigated the effect of liposome-encapsulated drugs on the efficacy of targeted delivery in SDT. They found that, in addition to its convenience and practicality, SDT is a safe and effective option for treating cancer.[18]
Exosomes
Exosomes are nanocarriers that can provide targeted drug delivery of therapeutics to enhance local cytotoxic effects while minimizing any systemic impact. They are acquired from cells and are used for transportation purposes within the cell as membrane-bound vesicles. Advantages of exosomes for drug delivery purposes include their ability to be manipulated and engineered, in addition to their low toxicity and immunogenicity.[41][42] They have also inspired research into non-cell-based treatment methods for various cancers and diseases.[41] Other desirable aspects of exosomes include their overall biocompatibility and stability.[42] A study by Nguyen Cao et al. investigated the use of exosomes for the delivery of indocyanine green (ICG), a sonosensitizer for breast cancer treatment.[43] Significantly increased reactive oxygen species generation was observed in breast cancer cells treated with folic acid-conjugated exosomes.[43] This is one example of a sonosensitizer used to treat a specific cancer using sonodynamic therapy. Another example of exosome-based sonodynamic therapy was illustrated by Liu et al. In this study, exosomes were decorated with porphyrin sensitizers and this system was used with an external ultrasound device to control and target drug delivery through SDT.[40] Liu et al. provided a non-invasive method for treating cancer through extracorporeal activation of exosomes through ultrasound.[40]
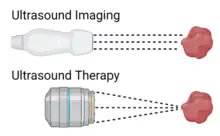
Microbubbles

Due to their ability to oscillate with exposure to low-frequency ultrasound, microbubbles have been used as contrast agents in order to visualize tissues in which the microbubbles have permeated.[44] However, when these microspheres are exposed to higher pressure ultrasound, they can rupture, which could be beneficial for drug delivery purposes.[44] Through SDT, these microbubbles could be selectively bursted at the tumor microenvironment in order to decrease systemic levels of the encapsulated drug and increase therapeutic efficacy. When applying SDT, the increase in acoustic pressure leads to the inertial cavitation, or collapse of the microbubble and local release of the cargo within. The inertial cavitation of the microbubbles when exposed to SDT is also referred to as ultrasound mediated microbubble destruction (UMMD).[45] The shell of microbubbles can be decorated with different components, including polymers, lipids, or proteins depending on their intended purpose.[44] Microbubbles have also been used for the localized release of attached cargo. This cargo is typically chemotherapeutics, antibiotics, or genes.[12] Different drugs can be directly loaded into the microbubble with methods such as conjugation and nanoparticle, liposome loading, and genes. The combination of genes and SDT is referred to as sonotransfection.[12] Examples of outer shell modifications can be seen in a study by McEwan et al. which found that lipid microbubbles showed reduced stability when sonosensitizers were added to their shells.[44] However, attaching the polymer poly lactic-co-glycolic acid (PLGA) to the shell resulted in increased stability compared to the lipid microbubbles without losing other desirable properties such as targeted delivery and selective cytotoxicity.[44] In another study, McEwan et al. investigated the ability of microbubbles carrying oxygen to increase production of reactive oxygen species, which are a necessary component of SDT, in the hypoxic environment of many solid tumors.[46] These microbubbles were stabilized with lipids and a Rose Bengal sonosensitizer was attached to the surface to treat pancreatic cancer.[46] Their work showed that coupling oxygen-loaded microbubbles that are sensitive to ultrasound with sonosensitizing drugs could allow for increased drug activation at the desired target even if hypoxia is present. Examples of therapeutics that have been loaded into microbubbles are gemcitabine, paclitaxel nanoparticles, plasmid DNA and 2,2′-azobis[2-(2-imidazolin-2-yl)propane]dihydrochloride loaded liposomes.[47][45][48][49] Due to the targeting nature of the ligands connected to the microbubble, it allows for the controlled and specific targeting of the desired tissue for treatment. Another study performed by Nesbitt et al. has shown improved tumor reduction when gemcitabine was loaded into the microbubble and applied to a human pancreatic cancer xenograft model with SDT.[48]
Nanobubbles
Similar to microbubbles, nanobubbles have shown efficacy in SDT.[50] However, due to their smaller size, nanobubbles are able to reach targets that microbubbles cannot. Nanobubbles can reach deeper tissue and travel past the vasculature. Previous research has demonstrated that nanobubbles are more capable of reaching the tumor since they can permeate endothelial cells and migrate away from the vasculature.[51][50] One study by Nittayacharn et al. developed doxorubicin-loaded nanobubbles and paired them with porphyrin sensitizers to be used in SDT for treatment of breast and ovarian cancer cells in vitro.[50] They found an almost 70% increase in cytotoxicity when using SDT compared to only perfluoropropane nanobubbles filled with iridium(III).[50] Additionally, compared to empty nanobubbles and/or free iridium(III), they observed greatest reactive oxygen species generation in the iridium(III)-nanobubbles exposed to ultrasound.[50] These results demonstrate that nanobubbles loaded with a sonosensitizer and exposed to ultrasound could be a potential effective treatment for cancer using SDT. As with microbubbles, nanobubbles have also shown promise as oxygen-delivering vesicles to enhance the effectiveness of SDT. In order to mitigate hypoxia of target tissue, Owen et al. used a pancreatic cancer rodent model to deliver phospholipid stabilized nanobubbles filled with oxygen.[52] The mice were divided into groups, one that received oxygen-filled nanobubbles prior to injection of a sonosensitizer and one that didn't.[52] A statistically significant difference between the levels of oxygen in the tumors of the two groups was observed, indicating that nanobubbles could be an effective addition to SDT to treat cancers in a hypoxic environment.[52]
Applications
Combination with other therapies
Sonodynamic therapy can be combined with other therapeutic techniques to enhance treatment efficacy for various types of cancers and diseases. SDT can be combined with photodynamic therapy, chemotherapy, radiation, MRI, and immunotherapy. PDT has often been used in combination with SDT as sonosensitizers are also photosensitive.[1] During initial development of SDT, Umemura et al., have determined that hematoporphyrins were able to initiate cell death similarly to PDT.[21] This is due to SDT being able to initiate sonoluminescence. However, the advantage of SDT over PDT is that it can penetrate deep and precisely into the targeted tissue. In a study by Lui et al., it was shown that using a combination of these two delivery methods results in increased cytotoxicity with sino porphyrin in a metastatic xenograft model.[53] In another example of combining SDT with PDT, Borah et al. investigated the advantage of 2-(1-hexyloxyethyl)-2-devinyl pyropheophorbide-a (HHPH), a photodynamic therapy drug, as a sonosensitizer and a photosensitizer for treating glioblastoma.[54] Combining these therapies showed increased cell kill/tumor response, possibly caused by synergistic effects.[54]
The goal of a study by Browning et al. was to investigate the potential enhancement of chemoradiation efficacy through combining it with sonodynamic therapy in pancreatic cancer patients. In one model, survival increased with the combination compared to chemoradiation alone. Differences in the results for the two different models could be attributed to variations in tumor organization.[6] The tumors that showed the greatest reduction in size were less vascularized, perhaps making them more vulnerable to SDT.[6] Another study, by Huang et al. used elements of mesoporous organosilica-based nanosystems to fabricate a sonosensitizer to be used with MRI-guided SDT.[55] Increased cell death and inhibiting tumor growth was induced by the sonosensitizers, indicating high SDT efficiency.[55] This shows how SDT can assist with both removal and inhibition of tumor growth.
SDT has also been combined with immunotherapy. A study by Lin et al. aimed to use cascade immuno-sonodynamic therapy to enhance tumor treatment using antibodies.[56] The nanosonosensitizers resulted in high drug loading efficiency and a tumor-specific adaptive immune response. This serves as an example as to how SDT can be coupled with checkpoint blockade immunotherapy to enhance efficiency in cancer treatments. Another study by Yue et al. strived to combine checkpoint-blockade immunotherapy with nanosonosensitizers-augmented noninvasive sonodynamic therapy.[57] Along with inhibiting lung metastasis, this combination promoted an anti-tumor response that prohibited tumor growth. This provides a proof-of-concept for combining SDT with another therapy to enhance treatment effects for the short and long term.
Cancer Treatment
The treatment of many different types of cancers has been investigated using sonodynamic therapy both in vitro and/or in vivo including, glioblastoma, pancreatic, breast, ovarian, lung, prostate, liver, stomach, and colon cancers.[54][6][20][50][52] A study by Gao et al. showed that SDT is capable of inhibiting angiogenesis through the production of ROS. This hindered the proliferation, migration, and invasion of endothelial cells, tumor growth, intratumoral vascularity, and vascular endothelial growth factor expression within the tumor cell in xenograft rat models.[58] Hachimine et al. performed a large in vitro study testing SDT on seventeen different cancer cell lines.[20] The types of cancers included were pancreatic, breast, lung, prostate, liver, stomach, and colon cancers.[20] The most successful treatment was that of lung cancer with 23.4% cell viability post-therapy.[1][20] Qu et al. aimed to develop an “all-in-one” nanosensitizer platform triggered by SDT that combines various diagnostic and therapeutic effects to treat glioblastoma.[59] Apoptosis was successfully induced and mitophagy was inhibited in glioma cells. This is an example of how SDT can be used with a different platform to treat glioblastoma. Borah et al., as mentioned above, also investigated the ability of SDT (and PDT) to treat glioblastoma and found that SDT (combined with PDT) was able to increase the number of tumor cells killed.[54] McEwan et al. and Owen et al. both demonstrated the use of micro/nanobubbles to enhance the oxygen concentration near hypoxic pancreatic tumors, thereby increasing the efficacy of SDT.[46][52]
Breast Cancer

12% of women in the US will be diagnosed with breast cancer.[60] Metastasis and recurrence is a large challenge for deep-seated solid state tumors.[39] SDT is currently being explored as a treatment method for breast cancer, while avoiding the side effects associated with current therapeutic methods.[61] There has been shown success in utilizing SDT in animal and human clinical trials in reduction of tumor size through mitochondrial targeting to initiate apoptosis of tumor cells and autophagy and immune response regulation.[62][39][63][64][24][53][60][65][61] However, there are still complications with proper therapeutic efficacy when used alone.
Glioma
Malignant glioma is an extremely difficult to treat brain tumor that is a leading cause of death worldwide and half of cancer-related deaths.[14] Complications associated with treating glioma include the blood brain barrier (BBB).[14] This protective mechanism for the brain also raises challenges for drug delivery through the tight junctions between endothelial cells, only allowing small lipid-soluble drugs (<400 Da) to permeate.[14] Current delivery methods are surgery and chemotherapy. SDT has been implemented as a method to open the BBB and has shown success in opening tight junctions for delivery. Examples of sonosensitizers that have shown success in glioma treatment are hematopor-phyrin monomethyl ether (HMME), porfimer sodium (Photofrin), di-sulfo-di-phthalimidomethyl phthalolcyaninezinc (ZnPcS2P2), Photolon, 5-aminolevulinic acid (5-ALA), and rose bengal (RB).[14] These have shown to induce effects such as opening of the BBB, improved vascular permeability, and apoptosis of glioma cells.
Prostate Cancer

Prostate cancer is the second cause of cancer and the most common malignancy associated with deaths in men worldwide.[66] Current methods of treatments are invasive resection therapy, radiation therapy, and prostatectomy that can cause complications such as incontinence, impotence, and damage to surrounding organs and tissues.[67][17] Current studies have shown success in using SDT as a stand-alone treatment.[68] SDT uses mitochondria related apoptosis for the reduction of cell viability. SDT for prostate cancer treatment has also been used alongside chemotherapeutics such as docetaxel microbubbles.[17][67][68] This has shown to enhance the effects of docetaxel through a reduction in tumor perfusion and enhanced necrosis and apoptosis.[68] The SDT and docetaxel group showed reduction in tumor growth.[68] Overall, the use of SDT has shown promising results in prostate cancer treatment.
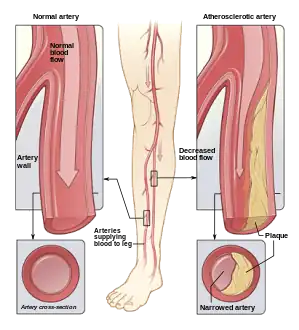
Arterial Diseases
Sonodynamic therapy could be used to treat more than just cancers. Atherosclerosis, which is a chronic arterial disease, is another target that has been observed in the literature.[3][5] This disease occurs when fatty plaques aggregate on the inner surface of the artery and could be caused by malfunctions in lipid metabolism.[3] More specifically, atherosclerosis is caused by an increase in endothelial permeability causing low-density lipoprotein particles to become oxidized and undergo sedimentation.[3] These lipoproteins cause an increase in macrophages and lead to intensified plaque build up. As a result, the high influx of macrophages is the target for AS treatment in order to slow plaque build-up.[3] Alongside the relationship between plaque build-up and macrophages, monocyte's differentiation into macrophages exacerbates the aforementioned process in addition to causing inflammation.[3]
A study by Wang et al. aimed to understand the underlying mechanisms regarding the potential effect of non-lethal SDT on atheroscleroic plaques. It was determined that non-lethal SDT prevents plaque development.[5] A study performed by Jiang et al., showed success in SDT through the reduction of macrophage inflammatory factors such as TNF-alpha, IL-12, and IL-1B. They also showed that SDT could inhibit plaque inflammation in patients with peripheral artery disease and continue to promote positive results for longer than six months.[4] Popular sonosensitizers for AS treatment are protoporphyrin IX (PpIX) and 5-aminolevulinic acid (5-ALA).[69][3] PpIX is often used in PDT and is generated through 5-ALA, a non ultrasound-activated component, through increasing PpIX concentration within a cell. A study by Cheng et al. determined that THP-1 macrophage apoptosis is induced by an increase in PpiX concentration, leading to the production of large amounts of ROS.[70][13][3] The use of SDT for AS treatment has also shown success in promoting the repopulation of vascular smooth muscle cells (VMSCs) through inducing further expression and autophagy to prevent VMSC evolution into plaque-holding macrophages. A study performed by Dan et al. showed the increase in smooth muscle a-actin, smooth muscle 22a, p38 mitogen-activated protein kinase phosphorylation.[71][3] While a study by Geng et al. showed improved VMSC autophagy. Each of these factors contributed to the improved differentiation and development of VMSCs.[3]
In vitro
In vitro experimentation provides great insight and knowledge to characterize the potential of sonosensitizer behavior in vivo. In addition, SDT has shown success through its low intensity allowing increased plasma membrane permeability without cell death.[1] Sonosensitizers have also been used in vitro in applications with different cell lines and to further understand the mechanism of action for cell death. It is currently understood that PDT and SDT have similar mechanisms for free radical generation for inducing apoptosis and necrosis.[1] However, each cell line is unique and can cause cell death with different efficacy.[20][1][72] Some examples of in vitro work include initial studies that were performed by Yumita et al., 1989 who used haematoprophyrin and SDT for mouse sarcoma 180 and rat ascites hepatoma (AH) that showed a relationship between dosage and ultrasound, and microbubbles causing cavitation leading to cell damage without the use of drugs. This study also emphasized the difference in efficacy between cell lines through SDT 180 having less lysis compared to AH-130 cells. Another study by Hachimine et al. emphasized efficacy between cell lines by examining seven different cancers with 17 cell lines total under the use of DCPH-P-NA(I).[1][20] This study revealed that the stomach and lung cancer lines of MKN-28 and LU65A respectively had the highest survival rate, but the stomach and lung cancer lines of RERFLC-KJ and MKN-45 respectively had the lowest survival rates.[20][1] Another study by Honda et al., with U937 and K562 showed that sonication increases the intracellular calcium ion levels and decreases GSH concentration respectively.[30] This increased concentration of calcium plays a significant role in cell death through DNA fragmentation and mitochondrial membrane disruption.[1][30] While a decreased concentration of GSH plays a significant role in allowing the formation of more free radicals.[30][1] A study by Umemura et al., found that ATX-70 versus hematoporphyrin has increased cytotoxic activity.[21][1] Current research typically focuses on using tumor xenograft models to determine the effect of SDT on target cells and delivery efficacy.[1]
In vivo
Building upon the study by Umemura et al. and ATX-70, it was found that 24h after administration of the sonosensitizer had improved efficacy when ultrasound was applied compared to immediate administration.[21][1] It was also determined that most ultrasound frequencies range between 1-3 MHz and 0.5-4W/cm^2. Higher frequencies at values such as 20W/cm^2 and 25W/cm^2 resulted in large necrotic lesions.[73][1] This established a relationship between sonosensitizer formulation and ultrasound intensity to necrosis. Other studies have continued to innovate upon this by controlling drug ultrasound interval (DUI) for different sonosensitizers in order to determine the optimal time period to apply the ultrasound for improved efficacy.[58][1] In addition, it has been shown that SDT can disturb surrounding vasculature in tumors.[1][58] This has been shown in studies by Gao et al. with 5-ALA in mice and human umbilical vein endothelial cell lines through inhibition of microvessel density and cell proliferation, migration, and invasion.[58][1]
Challenges and Development
One of the many advantages of SDT compared to PDT is the ability of SDT to penetrate deeply placed solid tumors allowing a wider treatment range.[1] Despite this fact, there are limitations to SDT that must be overcome or have optimized components in order to expand the effect and application of SDT.[31] SDT does allow for precise activation of the therapeutic, but is limited in the delivery and accumulation of the delivery modality to penetrate deeply into the desired tumor site.[74] This is often accommodated for through delivery vessels such as nanoparticles or liposomes.[1] However, nanomedicine is limited by the enhanced permeability and retention effect and struggles to deliver in targeted abundance depending on the delivery vesicle.[31][74] This can be seen in nanoparticles struggling with non-specific delivery. Future research has been focused on developing high targeting and penetrating nanoparticles for improved delivery and pharmacokinetics.[75][31] Due to the complex nature of tumors and their microenvironments, they are difficult to treat with only one therapy. In order to enhance the oftentimes low production of reactive oxygen species to address the hypoxic tumor environment, SDT can be combined with other therapies, such as PDT, chemotherapy, and immunotherapy to improve patient outcomes.[2][56][54][6] SDT alone does not respond well in hypoxic environments. However, bioreductive therapy could be used to reduce the impact of SDT's limitations regarding hypoxia in the tumor while leaving healthy/normal tissue alone.[2] Sonosensitizers also require continuous high levels of oxygen to create ROS, which is not readily available within a hypoxic tumor microenvironment.[31] However, strategies such as oxygen supplementation and production to supply the required oxygen and enhance cavitation, and glutathione depletion to avoid the reduction of the free radicals produced have been implemented alongside sonosensitizers to supply the required oxygen or reduce the combative function.[76][74] In addition to its relatively low generation of reactive oxygen species, SDT also can cause permanent destruction of normal tissues. This lack of selectivity is caused by ultrasound divergence, resulting in heat and shear that impacts off-target tissues.[2] Although advantages of organic sonosensitizers exist, such as high reproducibility, biocompatibility, production of reactive oxygen species, they also have limitations.[2] Factors that limit the translation of organic sensitizers to clinical applications include low water solubility, sonotoxicity, and targetability as well as high phototoxiticty.[2] Other properties could promote rapid clearance of the drug, which is why various nano and microparticles are used to transport the drug to the desired location.[2] In addition, sonosensitizers in SDT often require increased dosage, and the relationship between therapeutic dosage and toxicity of sonosensitizers has not been properly characterized alongside other variables such as tissue type and acoustic pressure.[31] Inorganic sensitizers produce reactive oxygen species, but in lower concentrations than desirable for SDT, limiting their ability to be used in a clinical setting.[2] Another challenge is reflected in vitro and in vivo work. An example of this can be seen in a study using rose bengal, a xanthene dye.[1] It was found to be successful in vitro, but in vivo showed significantly less efficacy due to liver squestation and clearance.[1] Lastly, there are no current standardized computer simulations to predict the characteristics of different sonosenistizers within tissue, which would provide further insight into how sonosensitizers may behave.[16]
Current Clinical Use

SDT has been researched most commonly to combat cancers and atherosclerosis such as breast cancer, pancreatic cancer, liver, and spinal sarcomas.[7][3][8][9][13][12][11][10][16][15][14][77] Currently, there are no FDA approved clinical applications of SDT. However, for PDT, Photofrin is an FDA approved hematoporphyrin (PHOTOFRIN®). However, SDT has been used in a clinical trial in combination with PDT to assess for reduction in tumor size in patients with breast cancer.[1] However, it was difficult to determine if SDT PDT or the drug dosage was the primary mechanism of treatment.[1] Another case study expanded on this by using SDT as a standalone treatment with a Gc protein hormone therapy with the use of 5-ALA or chlorin e6 as a sonosensitizer. It was shown that tumor markers significantly decreased during treatment.[1][78]
Future Directions
The effectiveness of sonodynamic therapy as a cancer treatment is supported by many in vitro and in vivo studies.[1] However, large-scale clinical trials are necessary for translation into the clinical setting. In order to mitigate the limitations aforementioned, new sonosensitizers are being developed and SDT is being combined with other therapies in novel ways. Particularly, organic sonosensitizers with high solubility in water, high sonotoxocity, increased ability to target tumors, and low phototoxicity need to be developed in order to improve the therapeutic efficacy of SDT and allow it to be used for treating cancers.[2] In addition, the mechanisms by which ROS are produced by sonosensitizers upon exposure to ultrasound is yet to be determined, reducing the ability to control its function and outcomes. Ultimately, the synergistic effects of combining SDT with other therapies would allow each to compensate for the limitations of the other, improving their therapeutic efficacy and increasing their ability to destroy tumors.[2]
References
- Costley, David; Mc Ewan, Conor; Fowley, Colin; McHale, Anthony P.; Atchison, Jordan; Nomikou, Nikolitsa; Callan, John F. (17 February 2015). "Treating cancer with sonodynamic therapy: A review". International Journal of Hyperthermia. 31 (2): 107–117. doi:10.3109/02656736.2014.992484. ISSN 0265-6736. PMID 25582025. S2CID 23665143.
- Xing, Xuejian; Zhao, Shaojing; Xu, Ting; Huang, Li; Zhang, Yi; Lan, Minhuan; Lin, Changwei; Zheng, Xiuli; Wang, Pengfei (15 October 2021). "Advances and perspectives in organic sonosensitizers for sonodynamic therapy". Coordination Chemistry Reviews. 445: 214087. doi:10.1016/j.ccr.2021.214087. ISSN 0010-8545.
- Geng, Chi; Zhang, Yunlong; Hidru, Tesfaldet Habtemariam; Zhi, Lianyun; Tao, Mengxing; Zou, Leixin; Chen, Chen; Li, Huihua; Liu, Ying (15 August 2018). "Sonodynamic therapy: A potential treatment for atherosclerosis". Life Sciences. 207: 304–313. doi:10.1016/j.lfs.2018.06.018. ISSN 0024-3205. PMID 29940244. S2CID 49404799.
- Jiang, Yongxing; Fan, Jingxue; Li, Yong; Wu, Guodong; Wang, Yuanqi; Yang, Jiemei; Wang, Mengjiao; Cao, Zhengyu; Li, Qiannan; Wang, Hui; Zhang, Zhengyan; Wang, Yu; Li, Bicheng; Sun, Fengyu; Zhang, Haiyu; Zhang, Zhiguo; Li, Kang; Tian, Ye (15 February 2021). "Rapid reduction in plaque inflammation by sonodynamic therapy inpatients with symptomatic femoropopliteal peripheral artery disease:A randomized controlled trial". International Journal of Cardiology. 325: 132–139. doi:10.1016/j.ijcard.2020.09.035. ISSN 0167-5273. PMID 32966832. S2CID 221884358.
- Wang, Yu; Wang, Wei; Xu, Haobo; Sun, Yan; Sun, Jing; Jiang, Yongxing; Yao, Jianting; Tian, Ye (2017). "Non-Lethal Sonodynamic Therapy Inhibits Atherosclerotic Plaque Progression in ApoE-/- Mice and Attenuates ox-LDL-mediated Macrophage Impairment by Inducing Heme Oxygenase-1". Cellular Physiology and Biochemistry. 41 (6): 2432–2446. doi:10.1159/000475913. ISSN 1015-8987. PMID 28468003. S2CID 32744546.
- Browning, Richard J.; Able, Sarah; Ruan, Jia-Ling; Bau, Luca; Allen, Philip D.; Kersemans, Veerle; Wallington, Sheena; Kinchesh, Paul; Smart, Sean; Kartsonaki, Christiana; Kamila, Sukanta; Logan, Keiran; Taylor, Mark A.; McHale, Anthony P.; Callan, John F.; Stride, Eleanor; Vallis, Katherine A. (10 September 2021). "Combining sonodynamic therapy with chemoradiation for the treatment of pancreatic cancer". Journal of Controlled Release. 337: 371–377. doi:10.1016/j.jconrel.2021.07.020. ISSN 0168-3659. PMID 34274382.
- Fan, Ching-Hsiang; Ting, Chien-Yu; Liu, Hao-Li; Huang, Chiung-Yin; Hsieh, Han-Yi; Yen, Tzu-Chen; Wei, Kuo-Chen; Yeh, Chih-Kuang (1 March 2013). "Antiangiogenic-targeting drug-loaded microbubbles combined with focused ultrasound for glioma treatment". Biomaterials. 34 (8): 2142–2155. doi:10.1016/j.biomaterials.2012.11.048. ISSN 0142-9612. PMID 23246066.
- Hadi, Marym Mohammad; Nesbitt, Heather; Masood, Hamzah; Sciscione, Fabiola; Patel, Shiv; Ramesh, Bala S.; Emberton, Mark; Callan, John F.; MacRobert, Alexander; McHale, Anthony P.; Nomikou, Nikolitsa (10 January 2021). "Investigating the performance of a novel pH and cathepsin B sensitive, stimulus-responsive nanoparticle for optimised sonodynamic therapy in prostate cancer". Journal of Controlled Release. 329: 76–86. doi:10.1016/j.jconrel.2020.11.040. ISSN 0168-3659. PMC 8551370. PMID 33245955.
- McHale, Anthony P.; Callan, John F.; Nomikou, Nikolitsa; Fowley, Colin; Callan, Bridgeen (2016). "Sonodynamic Therapy: Concept, Mechanism and Application to Cancer Treatment". Therapeutic Ultrasound. Advances in Experimental Medicine and Biology. Vol. 880. pp. 429–450. doi:10.1007/978-3-319-22536-4_22. ISBN 978-3-319-22535-7. PMID 26486350.
- Pan, Xueting; Wang, Hongyu; Wang, Shunhao; Sun, Xiao; Wang, Lingjuan; Wang, Weiwei; Shen, Heyun; Liu, Huiyu (1 April 2018). "Sonodynamic therapy (SDT): a novel strategy for cancer nanotheranostics". Science China Life Sciences. 61 (4): 415–426. doi:10.1007/s11427-017-9262-x. ISSN 1869-1889. PMID 29666990. S2CID 4937368.
- Sun, Shengjie; Wu, Meiying (1 January 2021). "Sonodynamic therapy: Another "light" in tumor treatment by exogenous stimulus". Smart Materials in Medicine. 2: 145–149. doi:10.1016/j.smaim.2021.05.001. ISSN 2590-1834. S2CID 236730960.
- Tachibana, Katsuro; Feril, Loreto B.; Ikeda-Dantsuji, Yurika (1 August 2008). "Sonodynamic therapy". Ultrasonics. 48 (4): 253–259. doi:10.1016/j.ultras.2008.02.003. ISSN 0041-624X. PMID 18433819.
- Wan, Guo-Yun; Liu, Yang; Chen, Bo-Wei; Liu, Yuan-Yuan; Wang, Yin-Song; Zhang, Ning (September 2016). "Recent advances of sonodynamic therapy in cancer treatment". Cancer Biology & Medicine. 13 (3): 325–338. doi:10.20892/j.issn.2095-3941.2016.0068. ISSN 2095-3941. PMC 5069838. PMID 27807500.
- Wang, Xiaobing; Jia, Yali; Wang, Pan; Liu, Quanhon; Zheng, Hairong (1 July 2017). "Current status and future perspectives of sonodynamic therapy in glioma treatment". Ultrasonics Sonochemistry. 37: 592–599. doi:10.1016/j.ultsonch.2017.02.020. ISSN 1350-4177. PMID 28427672.
- Wu, Nan; Fan, Ching-Hsiang; Yeh, Chih-Kuang (2 March 2022). "Ultrasound-activated nanomaterials for sonodynamic cancer theranostics". Drug Discovery Today. 27 (6): 1590–1603. doi:10.1016/j.drudis.2022.02.025. ISSN 1359-6446. PMID 35247594. S2CID 247244458.
- Zhou, Yiming; Wang, Mengxuan; Dai, Zhifei (30 July 2020). "The molecular design of and challenges relating to sensitizers for cancer sonodynamic therapy". Materials Chemistry Frontiers. 4 (8): 2223–2234. doi:10.1039/D0QM00232A. ISSN 2052-1537. S2CID 225442575.
- Yamaguchi, Toshihiro; Kitahara, Shuji; Kusuda, Kaori; Okamoto, Jun; Horise, Yuki; Masamune, Ken; Muragaki, Yoshihiro (8 December 2021). "Current Landscape of Sonodynamic Therapy for Treating Cancer". Cancers. 13 (24): 6184. doi:10.3390/cancers13246184. ISSN 2072-6694. PMC 8699567. PMID 34944804.
- Dai, Zhi-Jun; Li, Sha; Gao, Jie; Xu, Xiao-Na; Lu, Wang-Feng; Lin, Shuai; Wang, Xi-Jing (1 March 2013). "Sonodynamic therapy (SDT): A novel treatment of cancer based on sonosensitizer liposome as a new drug carrier". Medical Hypotheses. 80 (3): 300–302. doi:10.1016/j.mehy.2012.12.009. ISSN 0306-9877. PMID 23294609.
- Mišík, Vladimír; Riesz, Peter (25 January 2006). "Free Radical Intermediates in Sonodynamic Therapy". Annals of the New York Academy of Sciences. 899 (1): 335–348. doi:10.1111/j.1749-6632.2000.tb06198.x. PMID 10863551. S2CID 13503189.
- Hachimine, Ken; Shibaguchi, Hirotomo; Kuroki, Motomu; Yamada, Hiromi; Kinugasa, Tetsushi; Nakae, Yoshinori; Asano, Ryuji; Sakata, Isao; Yamashita, Yuichi; Shirakusa, Takayuki; Kuroki, Masahide (June 2007). "Sonodynamic therapy of cancer using a novel porphyrin derivative, DCPH-P-Na(I), which is devoid of photosensitivity". Cancer Science. 98 (6): 916–920. doi:10.1111/j.1349-7006.2007.00468.x. ISSN 1347-9032. PMID 17419708. S2CID 25732120.
- Umemura, Shin-ichiro; Yumita, Nagahiko; Nishigaki, Ryuichiro; Umemura, Koshiro (September 1990). "Mechanism of Cell Damage by Ultrasound in Combination with Hematoporphyrin". Japanese Journal of Cancer Research. 81 (9): 962–966. doi:10.1111/j.1349-7006.1990.tb02674.x. PMC 5918111. PMID 2172198.
- Hiraoka, Wakako; Honda, Hidemi; Feril, Loreto B.; Kudo, Nobuki; Kondo, Takashi (1 September 2006). "Comparison between sonodynamic effect and photodynamic effect with photosensitizers on free radical formation and cell killing". Ultrasonics Sonochemistry. 13 (6): 535–542. doi:10.1016/j.ultsonch.2005.10.001. ISSN 1350-4177. PMID 16325451.
- Miyoshi, Norio; Igarashi, Takashi; Riesz, Peter (1 July 2000). "Evidence against singlet oxygen formation by sonolysis of aqueous oxygen-saturated solutions of Hematoporphyrin and Rose Bengal: The mechanism of sonodynamic therapy". Ultrasonics Sonochemistry. 7 (3): 121–124. doi:10.1016/S1350-4177(99)00042-5. ISSN 1350-4177. PMID 10909730.
- Liao, Ai-Ho; Li, Ying-Kai; Lee, Wei-Jiunn; Wu, Ming-Fang; Liu, Hao-Li; Kuo, Min-Liang (1 November 2012). "Estimating the Delivery Efficiency of Drug-Loaded Microbubbles in Cancer Cells with Ultrasound and Bioluminescence Imaging". Ultrasound in Medicine & Biology. 38 (11): 1938–1948. doi:10.1016/j.ultrasmedbio.2012.07.013. ISSN 0301-5629. PMID 22929655.
- Pickworth, M J W; Dendy, P P; Leighton, T G; Walton, A J (1 November 1988). "Studies of the cavitational effects of clinical ultrasound by sonoluminescence: 2. Thresholds for sonoluminescence from a therapeutic ultrasound beam and the effect of temperature and duty cycle". Physics in Medicine and Biology. 33 (11): 1249–1260. Bibcode:1988PMB....33.1249P. doi:10.1088/0031-9155/33/11/003. ISSN 0031-9155. S2CID 250766457.
- Saksena, T. K.; Nyborg, W. L. (1 September 1970). "Sonoluminescence from Stable Cavitation". The Journal of Chemical Physics. 53 (5): 1722–1734. Bibcode:1970JChPh..53.1722S. doi:10.1063/1.1674249. ISSN 0021-9606.
- Gaitan, D. Felipe; Crum, Lawrence A.; Church, Charles C.; Roy, Ronald A. (1 June 1992). "Sonoluminescence and bubble dynamics for a single, stable, cavitation bubble". The Journal of the Acoustical Society of America. 91 (6): 3166–3183. Bibcode:1992ASAJ...91.3166G. doi:10.1121/1.402855. ISSN 0001-4966. S2CID 122235287.
- Kessel, David; Lo, Julie; Jeffers, Russell; Brian Fowlkes, J.; Cain, Charles (1 June 1995). "Modes of photodynamic vs. sonodynamic cytotoxicity". Journal of Photochemistry and Photobiology B: Biology. 28 (3): 219–221. doi:10.1016/1011-1344(94)07111-Z. ISSN 1011-1344. PMID 7623187.
- Yumita, Nagahiko; Iwase, Yumiko; Nishi, Koji; Ikeda, Toshihiko; Umemura, Shin-Ichiro; Sakata, Isao; Momose, Yasunori (1 June 2010). "Sonodynamically Induced Cell Damage and Membrane Lipid Peroxidation by Novel Porphyrin Derivative, DCPH-P-Na(I)". Anticancer Research. 30 (6): 2241–2246. ISSN 0250-7005. PMID 20651375.
- Honda, Hidemi; Kondo, Takashi; Zhao, Qing-Li; Feril, Loreto B; Kitagawa, Hiroshi (May 2004). "Role of intracellular calcium ions and reactive oxygen species in apoptosis induced by ultrasound". Ultrasound in Medicine & Biology. 30 (5): 683–692. doi:10.1016/j.ultrasmedbio.2004.02.008. PMID 15183235.
- Gong, Zhuoran; Dai, Zhifei (12 March 2021). "Design and Challenges of Sonodynamic Therapy System for Cancer Theranostics: From Equipment to Sensitizers". Advanced Science. 8 (10): 2002178. doi:10.1002/advs.202002178. ISSN 2198-3844. PMC 8132157. PMID 34026428.
- Araújo Martins, Yugo; Zeferino Pavan, Theo; Fonseca Vianna Lopez, Renata (15 December 2021). "Sonodynamic therapy: Ultrasound parameters and in vitro experimental configurations". International Journal of Pharmaceutics. 610: 121243. doi:10.1016/j.ijpharm.2021.121243. ISSN 0378-5173. PMID 34743959. S2CID 240248013.
- Suzuki, Norio; Okada, Kyoji; Chida, Shuichi; Komori, Chiyo; Shimada, Yoichi; Suzuki, Toshio (2007). "Antitumor Effect of Acridine Orange Under Ultrasonic Irradiation In Vitro". Anticancer Research. 27 (6B): 4179–4184. PMID 18225589.
- Komori, Chiyo; Okada, Kyoji; Kawamura, Koichi; Chida, Shuichi; Suzuki, Toshio (2009). "The Sonodynamic Antitumor Effect of Methylene Blue on Sarcoma180 Cells In Vitro". Anticancer Research. 29 (6): 2411–2415. PMID 19528509.
- Waksman, Ron; McEwan, Pauline E.; Moore, Travis I.; Pakala, Rajbabu; Kolodgie, Frank D.; Hellinga, David G.; Seabron, Rufus C.; Rychnovsky, Steven J.; Vasek, Jeffrey; Scott, Robert W.; Virmani, Renu (16 September 2008). "PhotoPoint Photodynamic Therapy Promotes Stabilization of Atherosclerotic Plaques and Inhibits Plaque Progression". Journal of the American College of Cardiology. 52 (12): 1024–1032. doi:10.1016/j.jacc.2008.06.023. PMID 18786486.
- Nomikou, Nikolitsa; Sterrett, Christine; Arthur, Ciara; McCaughan, Bridgeen; Callan, John F.; McHale, Anthony P. (August 2012). "The Effects of Ultrasound and Light on Indocyanine-Green-Treated Tumour Cells and Tissues". ChemMedChem. 7 (8): 1465–1471. doi:10.1002/cmdc.201200233. PMID 22715137. S2CID 28851902.
- Franco, Marina Santiago; Gomes, Eliza Rocha; Roque, Marjorie Coimbra; Oliveira, Mônica Cristina (2021). "Triggered Drug Release From Liposomes: Exploiting the Outer and Inner Tumor Environment". Frontiers in Oncology. 11: 623760. doi:10.3389/fonc.2021.623760. ISSN 2234-943X. PMC 8008067. PMID 33796461.
- Bozzuto, Giuseppina; Molinari, Agnese (2 February 2015). "Liposomes as nanomedical devices". International Journal of Nanomedicine. 10: 975–999. doi:10.2147/IJN.S68861. ISSN 1176-9114. PMC 4324542. PMID 25678787.
- Chen, Huaqing; Liu, Lanlan; Ma, Aiqing; Yin, Ting; Chen, Ze; Liang, Ruijing; Qiu, Yuzhi; Zheng, Mingbin; Cai, Lintao (1 February 2021). "Noninvasively immunogenic sonodynamic therapy with manganese protoporphyrin liposomes against triple-negative breast cancer". Biomaterials. 269: 120639. doi:10.1016/j.biomaterials.2020.120639. ISSN 0142-9612. PMID 33434714. S2CID 231595969.
- Liu, Yichen; Bai, Lianmei; Guo, Kaili; Jia, Yali; Zhang, Kun; Liu, Quanhong; Wang, Pan; Wang, Xiaobing (9 July 2019). "Focused ultrasound-augmented targeting delivery of nanosonosensitizers from homogenous exosomes for enhanced sonodynamic cancer therapy". Theranostics. 9 (18): 5261–5281. doi:10.7150/thno.33183. ISSN 1838-7640. PMC 6691590. PMID 31410214.
- Liang, Yujie; Duan, Li; Lu, Jianping; Xia, Jiang (1 January 2021). "Engineering exosomes for targeted drug delivery". Theranostics. 11 (7): 3183–3195. doi:10.7150/thno.52570. ISSN 1838-7640. PMC 7847680. PMID 33537081.
- Patil, Suyash M.; Sawant, Shruti S.; Kunda, Nitesh K. (1 September 2020). "Exosomes as drug delivery systems: A brief overview and progress update". European Journal of Pharmaceutics and Biopharmaceutics. 154: 259–269. doi:10.1016/j.ejpb.2020.07.026. ISSN 0939-6411. PMID 32717385. S2CID 220839948.
- Nguyen Cao, Thuy Giang; Kang, Ji Hee; You, Jae Young; Kang, Han Chang; Rhee, Won Jong; Ko, Young Tag; Shim, Min Suk (9 June 2021). "Safe and Targeted Sonodynamic Cancer Therapy Using Biocompatible Exosome-Based Nanosonosensitizers". ACS Applied Materials & Interfaces. 13 (22): 25575–25588. doi:10.1021/acsami.0c22883. ISSN 1944-8244. PMID 34033477. S2CID 235204026.
- McEwan, Conor; Fowley, Colin; Nomikou, Nikolitsa; McCaughan, Bridgeen; McHale, Anthony P.; Callan, John F. (16 December 2014). "Polymeric Microbubbles as Delivery Vehicles for Sensitizers in Sonodynamic Therapy". Langmuir. 30 (49): 14926–14930. doi:10.1021/la503929c. ISSN 0743-7463. PMID 25409533.
- Xing, Lingxi; Shi, Qiusheng; Zheng, Kailiang; Shen, Ming; Ma, Jing; Li, Fan; Liu, Yang; Lin, Lizhou; Tu, Wenzhi; Duan, Yourong; Du, Lianfang (2016). "Ultrasound-Mediated Microbubble Destruction (UMMD) Facilitates the Delivery of CA19-9 Targeted and Paclitaxel Loaded mPEG-PLGA-PLL Nanoparticles in Pancreatic Cancer". Theranostics. 6 (10): 1573–1587. doi:10.7150/thno.15164. PMC 4955056. PMID 27446491.
- McEwan, Conor; Owen, Joshua; Stride, Eleanor; Fowley, Colin; Nesbitt, Heather; Cochrane, David; Coussios, Constantin. C.; Borden, M.; Nomikou, Nikolitsa; McHale, Anthony P.; Callan, John F. (10 April 2015). "Oxygen carrying microbubbles for enhanced sonodynamic therapy of hypoxic tumours". Journal of Controlled Release. 203: 51–56. doi:10.1016/j.jconrel.2015.02.004. ISSN 0168-3659. PMID 25660073.
- Lin, Xiahui; Qiu, Yuan; Song, Liang; Chen, Shan; Chen, Xiaofeng; Huang, Guoming; Song, Jibin; Chen, Xiaoyuan; Yang, Huanghao (23 April 2019). "Ultrasound activation of liposomes for enhanced ultrasound imaging and synergistic gas and sonodynamic cancer therapy". Nanoscale Horizons. 4 (3): 747–756. Bibcode:2019NanoH...4..747L. doi:10.1039/C8NH00340H. ISSN 2055-6764. S2CID 104403902.
- Nesbitt, Heather; Sheng, Yingjie; Kamila, Sukanta; Logan, Keiran; Thomas, Keith; Callan, Bridgeen; Taylor, Mark A.; Love, Mark; O'Rourke, Declan; Kelly, Paul; Beguin, Estelle; Stride, Eleanor; McHale, Anthony P.; Callan, John F. (10 June 2018). "Gemcitabine loaded microbubbles for targeted chemo-sonodynamic therapy of pancreatic cancer". Journal of Controlled Release. 279: 8–16. doi:10.1016/j.jconrel.2018.04.018. ISSN 0168-3659. PMID 29653222. S2CID 4929495.
- Shen, Z P; Brayman, A A; Chen, L; Miao, C H (August 2008). "Ultrasound with microbubbles enhances gene expression of plasmid DNA in the liver via intraportal delivery". Gene Therapy. 15 (16): 1147–1155. doi:10.1038/gt.2008.51. PMC 3747825. PMID 18385766.
- Nittayacharn, Pinunta; Abenojar, Eric; La Deda, Massimo; Ricciardi, Loredana; Strangi, Giuseppe; Exner, Agata A. (6 March 2021). "Iridium(III) Complex-Loaded Perfluoropropane Nanobubbles for Enhanced Sonodynamic Therapy". Bioconjugate Chemistry. 33 (6): 1057–1068. doi:10.1021/acs.bioconjchem.1c00082. ISSN 1043-1802. PMC 10108504. PMID 33677967. S2CID 232143610.
- Perera, Reshani H.; de Leon, Al; Wang, Xinning; Wang, Yu; Ramamurthy, Gopal; Peiris, Pubudu; Abenojar, Eric; Basilion, James P.; Exner, Agata A. (1 August 2020). "Real time ultrasound molecular imaging of prostate cancer with PSMA-targeted nanobubbles". Nanomedicine: Nanotechnology, Biology and Medicine. 28: 102213. doi:10.1016/j.nano.2020.102213. ISSN 1549-9634. PMC 7605099. PMID 32348874.
- Owen, Joshua; Logan, Keiran; Nesbitt, Heather; Able, Sarah; Vasilyeva, Alexandra; Bluemke, Emma; Kersemans, Veerle; Smart, Sean; Vallis, Katherine A.; McHale, Anthony P.; Callan, John F.; Stride, Eleanor (February 2022). "Orally administered oxygen nanobubbles enhance tumor response to sonodynamic therapy". Nano Select. 3 (2): 394–401. doi:10.1002/nano.202100038. ISSN 2688-4011. S2CID 237906086.
- Liu, Yichen; Wang, Pan; Liu, Quanhong; Wang, Xiaobing (1 July 2016). "Sinoporphyrin sodium triggered sono-photodynamic effects on breast cancer both in vitro and in vivo". Ultrasonics Sonochemistry. 31: 437–448. doi:10.1016/j.ultsonch.2016.01.038. ISSN 1350-4177. PMID 26964970.
- Borah, Ballav M.; Cacaccio, Joseph; Durrani, Farukh A.; Bshara, Wiam; Turowski, Steven G.; Spernyak, Joseph A.; Pandey, Ravindra K. (11 December 2020). "Sonodynamic therapy in combination with photodynamic therapy shows enhanced long-term cure of brain tumor". Scientific Reports. 10 (1): 21791. Bibcode:2020NatSR..1021791B. doi:10.1038/s41598-020-78153-0. ISSN 2045-2322. PMC 7732989. PMID 33311561.
- Huang, Ping; Qian, Xiaoqin; Chen, Yu; Yu, Luodan; Lin, Han; Wang, Liying; Zhu, Yufang; Shi, Jianlin (25 January 2017). "Metalloporphyrin-Encapsulated Biodegradable Nanosystems for Highly Efficient Magnetic Resonance Imaging-Guided Sonodynamic Cancer Therapy". Journal of the American Chemical Society. 139 (3): 1275–1284. doi:10.1021/jacs.6b11846. ISSN 0002-7863. PMID 28024395.
- Lin, Xiaoning; Huang, Rong; Huang, Yanlin; Wang, Kai; Li, Heng; Bao, Yiheng; Wu, Chaohui; Zhang, Yi; Tian, Xinhua; Wang, Xiaomin (5 March 2021). "Nanosonosensitizer-Augmented Sonodynamic Therapy Combined with Checkpoint Blockade for Cancer Immunotherapy". International Journal of Nanomedicine. 16: 1889–1899. doi:10.2147/IJN.S290796. ISSN 1176-9114. PMC 7943542. PMID 33707944.
- Yue, Wenwen; Chen, Liang; Yu, Luodan; Zhou, Bangguo; Yin, Haohao; Ren, Weiwei; Liu, Chang; Guo, Lehang; Zhang, Yifeng; Sun, Liping; Zhang, Kun; Xu, Huixiong; Chen, Yu (2 May 2019). "Checkpoint blockade and nanosonosensitizer-augmented noninvasive sonodynamic therapy combination reduces tumour growth and metastases in mice". Nature Communications. 10 (1): 2025. Bibcode:2019NatCo..10.2025Y. doi:10.1038/s41467-019-09760-3. ISSN 2041-1723. PMC 6497709. PMID 31048681.
- Gao, Zhongxiuzi; Zheng, Jinhua; Yang, Bin; Wang, Zhu; Fan, Haixia; Lv, Yanhong; Li, Haixia; Jia, Limin; Cao, Wenwu (10 July 2013). "Sonodynamic therapy inhibits angiogenesis and tumor growth in a xenograft mouse model". Cancer Letters. 335 (1): 93–99. doi:10.1016/j.canlet.2013.02.006. ISSN 0304-3835. PMID 23402818.
- Qu, Fei; Wang, Pan; Zhang, Kun; Shi, Yin; Li, Yixiang; Li, Chengren; Lu, Junhan; Liu, Quanhong; Wang, Xiaobing (2 August 2020). "Manipulation of Mitophagy by "All-in-One" nanosensitizer augments sonodynamic glioma therapy". Autophagy. 16 (8): 1413–1435. doi:10.1080/15548627.2019.1687210. PMC 7480814. PMID 31674265.
- Waks, Adrienne G.; Winer, Eric P. (22 January 2019). "Breast Cancer Treatment: A Review". JAMA. 321 (3): 288–300. doi:10.1001/jama.2018.19323. ISSN 0098-7484. PMID 30667505. S2CID 58580711.
- Zuo, Shuting; Zhang, Yan; Wang, Zhenyu; Wang, Jing (5 March 2022). "Mitochondria-Targeted Mesoporous Titanium Dioxide Nanoplatform for Synergistic Nitric Oxide Gas-Sonodynamic Therapy of Breast Cancer". International Journal of Nanomedicine. 17: 989–1002. doi:10.2147/IJN.S348618. PMC 8906874. PMID 35280333.
- Alamolhoda, Mahboobeh; Mokhtari-Dizaji, Manijhe (24 June 2015). "Evaluation of fractionated and repeated sonodynamic therapy by using dual frequency for murine model of breast adenocarcinoma". Journal of Therapeutic Ultrasound. 3 (1): 10. doi:10.1186/s40349-015-0031-x. ISSN 2050-5736. PMC 4484850. PMID 26124951.
- Feng, Qianhua; Yang, Xuemei; Hao, Yutong; Wang, Ning; Feng, Xuebing; Hou, Lin; Zhang, Zhenzhong (11 September 2019). "Cancer Cell Membrane-Biomimetic Nanoplatform for Enhanced Sonodynamic Therapy on Breast Cancer via Autophagy Regulation Strategy". ACS Applied Materials & Interfaces. 11 (36): 32729–32738. doi:10.1021/acsami.9b10948. ISSN 1944-8244. PMID 31415145. S2CID 201019401.
- Huang, Biying; Chen, Sijie; Pei, Wenjing; Xu, Yan; Jiang, Zichao; Niu, Chengcheng; Wang, Long (2020). "Oxygen-Sufficient Nanoplatform for Chemo-Sonodynamic Therapy of Hypoxic Tumors". Frontiers in Chemistry. 8: 358. Bibcode:2020FrCh....8..358H. doi:10.3389/fchem.2020.00358. ISSN 2296-2646. PMC 7199163. PMID 32411675.
- Zhang, Nan; Tan, Yang; Yan, Liwei; Zhang, Chunyang; Xu, Ming; Guo, Huanling; Zhuang, Bowen; Zhou, Luyao; Xie, Xiaoyan (6 August 2020). "Modulation of Tumor Hypoxia by pH-Responsive Liposomes to Inhibit Mitochondrial Respiration for Enhancing Sonodynamic Therapy". International Journal of Nanomedicine. 15: 5687–5700. doi:10.2147/IJN.S256038. ISSN 1176-9114. PMC 7418152. PMID 32821097.
- Aksel, Mehran; Bozkurt-Girit, Ozlem; Bilgin, Mehmet Dincer (1 September 2020). "Pheophorbide a-mediated sonodynamic, photodynamic and sonophotodynamic therapies against prostate cancer". Photodiagnosis and Photodynamic Therapy. 31: 101909. doi:10.1016/j.pdpdt.2020.101909. ISSN 1572-1000. PMID 32619716. S2CID 220336627.
- Evans, Andrew J. (January 2018). "Treatment effects in prostate cancer". Modern Pathology. 31 (1): 110–121. doi:10.1038/modpathol.2017.158. ISSN 1530-0285. PMID 29297495. S2CID 21337740.
- Goertz, David E.; Todorova, Margarita; Mortazavi, Omid; Agache, Vlad; Chen, Branson; Karshafian, Raffi; Hynynen, Kullervo (20 December 2012). "Antitumor Effects of Combining Docetaxel (Taxotere) with the Antivascular Action of Ultrasound Stimulated Microbubbles". PLOS ONE. 7 (12): e52307. Bibcode:2012PLoSO...752307G. doi:10.1371/journal.pone.0052307. ISSN 1932-6203. PMC 3527530. PMID 23284980.
- Jiang, Yueqing; Kou, Jiayuan; Han, Xiaobo; Li, Xuesong; Zhong, Zhaoyu; Liu, Zhongni; Zheng, Yinghong; Tian, Ye; Yang, Liming (2017). "ROS-Dependent Activation of Autophagy through the PI3K/Akt/mTOR Pathway Is Induced by Hydroxysafflor Yellow A-Sonodynamic Therapy in THP-1 Macrophages". Oxidative Medicine and Cellular Longevity. 2017: 1–16. doi:10.1155/2017/8519169. PMC 5278230. PMID 28191279.
- Cheng, Jiali; Sun, Xin; Guo, Shuyuan; Cao, Wei; Chen, Haibo; Jin, Yinghua; Li, Bo; Li, Qiannan; Wang, Huan; Wang, Zhu; Zhou, Qi; Wang, Peng; Zhang, Zhiguo; Cao, Wenwu; Tian, Ye (2013). "Effects of 5-aminolevulinic acid-mediated sonodynamic therapy on macrophages". International Journal of Nanomedicine. 8: 669–676. doi:10.2147/IJN.S39844. ISSN 1176-9114. PMC 3576038. PMID 23426386.
- Dan, Juhua; Sun, Xin; Li, Wanlu; Zhang, Yun; Li, Xuesong; Xu, Haobo; Li, Zhitao; Tian, Zhen; Guo, Shuyuan; Yao, Jianting; Gao, Weidong; Tian, Ye (1 June 2015). "5-Aminolevulinic Acid-Mediated Sonodynamic Therapy Promotes Phenotypic Switching from Dedifferentiated to Differentiated Phenotype via Reactive Oxygen Species and p38 Mitogen-Activated Protein Kinase in Vascular Smooth Muscle Cells". Ultrasound in Medicine & Biology. 41 (6): 1681–1689. doi:10.1016/j.ultrasmedbio.2014.12.664. ISSN 0301-5629. PMID 25796412.
- Yumita, Nagahiko; Nishigaki, Ryuichiro; Umemura, Koshiro; Umemura, Shin-ichiro (March 1989). "Hematoporphyrin as a Sensitizer of Cell-damaging Effect of Ultrasound". Japanese Journal of Cancer Research. 80 (3): 219–222. doi:10.1111/j.1349-7006.1989.tb02295.x. PMC 5917717. PMID 2470713.
- Ohmura, Tadahiro; Fukushima, Takeo; Shibaguchi, Hirotomo; Yoshizawa, Shin; Inoue, Tooru; Kuroki, Masahide; Sasaki, Kazunari; Umemura, Shin-Ichiro (1 July 2011). "Sonodynamic Therapy with 5-Aminolevulinic Acid and Focused Ultrasound for Deep-seated Intracranial Glioma in Rat". Anticancer Research. 31 (7): 2527–2533. ISSN 0250-7005. PMID 21873170.
- Zheng, Yilin; Ye, Jinxiang; Li, Ziying; Chen, Haijun; Gao, Yu (August 2021). "Recent progress in sono-photodynamic cancer therapy: From developed new sensitizers to nanotechnology-based efficacy-enhancing strategies". Acta Pharmaceutica Sinica B. 11 (8): 2197–2219. doi:10.1016/j.apsb.2020.12.016. ISSN 2211-3835. PMC 8424231. PMID 34522584.
- Choi, Victor; Rajora, Maneesha A.; Zheng, Gang (15 April 2020). "Activating Drugs with Sound: Mechanisms Behind Sonodynamic Therapy and the Role of Nanomedicine". Bioconjugate Chemistry. 31 (4): 967–989. doi:10.1021/acs.bioconjchem.0c00029. ISSN 1043-1802. PMID 32129984. S2CID 212416405.
- Cheng, Danling; Wang, Xiaoying; Zhou, Xiaojun; Li, Jingchao (2021). "Nanosonosensitizers With Ultrasound-Induced Reactive Oxygen Species Generation for Cancer Sonodynamic Immunotherapy". Frontiers in Bioengineering and Biotechnology. 9: 761218. doi:10.3389/fbioe.2021.761218. ISSN 2296-4185. PMC 8514668. PMID 34660560.
- Lewis, Thomas J.; Mitchell, Doug (June 2008). "The Tumoricidal Effect of Sonodynamic Therapy (SDT) on S-180 Sarcoma in Mice". Integrative Cancer Therapies. 7 (2): 96–102. doi:10.1177/1534735408319065. ISSN 1534-7354. PMID 18550890. S2CID 22303568.
- Inui, Toshio; Makita, Kaori; Miura, Hirona; Matsuda, Akiko; Kuchiike, Daisuke; Kubo, Kentaro; Mette, Martin; Uto, Yoshihiro; Nishikata, Takahito; Hori, Hitoshi; Sakamoto, Norihiro (1 August 2014). "Case Report: A Breast Cancer Patient Treated with GcMAF, Sonodynamic Therapy and Hormone Therapy". Anticancer Research. 34 (8): 4589–4593. ISSN 0250-7005. PMID 25075104.