Stellate ganglion
The stellate ganglion (or cervicothoracic ganglion[1]) is a sympathetic ganglion formed by the fusion of the inferior cervical ganglion and the first thoracic (superior thoracic sympathetic) ganglion,[2] which is present in 80% of individuals. Sometimes, the second and the third thoracic ganglia are included in this fusion.
| Stellate ganglion | |
|---|---|
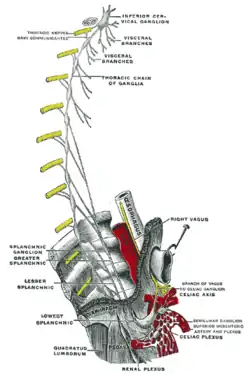 Plan of right sympathetic cord and splanchnic nerves. (Stellate ganglion not visible, but region is shown.) | |
| Details | |
| From | inferior cervical ganglion, first thoracic ganglia |
| Identifiers | |
| Latin | ganglion cervicothoracicum, ganglion stellatum |
| MeSH | D013233 |
| TA98 | A14.3.01.020 |
| TA2 | 6612 |
| FMA | 6469 |
| Anatomical terms of neuroanatomy | |
Anatomy
The stellate ganglion is polygonal in shape (Latin: stellatum, lit. 'star-shaped'). It is relatively big (10–12 × 8–20 mm) compared to the much smaller thoracic, lumbar, and sacral ganglia.
Relations
Stellate ganglion is located at the level of C7, anterior to the transverse process of C7 and the neck of the first rib, superior to the cervical pleura and just below the subclavian artery. It is superiorly covered by the prevertebral lamina of the cervical fascia and anteriorly in relation with common carotid artery, subclavian artery and the beginning of vertebral artery which sometimes leaves a groove at the apex of this ganglion (this groove can sometimes even separate the stellate ganglion into so called vertebral ganglion).
Relations of the apex of the stellate ganglion:
- covered by the endothoracic fascia and parietal pleura
- right stellate ganglion is in relation with right brachiocephalic vein anteriorly
- right stellate ganglion is in relation with sternal part of subclavian artery anteriorly
- laterally: first intercostal artery
- medially: longus colli muscle
Clinical significance
The stellate ganglia may be cut in order to decrease the symptoms exhibited by Raynaud's phenomenon and hyperhydrosis (extreme sweating) of the hands. Injection of local anesthetics near the stellate ganglion can sometimes mitigate the symptoms of sympathetically mediated pain such as complex regional pain syndrome type I (reflex sympathetic dystrophy), and symptoms associated with alterations in arousal and reactivity (Criterion E) of PTSD. Injection is often given near the Chassaignac's tubercle (anterior tubercle of transverse process of C6) due to this being an important landmark lateral to the cricoid cartilage. It is thought that anesthetic is spread along the paravertebral muscles to the stellate ganglion.
Stellate ganglion block also shows great potential as a means of reducing the number of hot flashes and night awakenings suffered by breast cancer survivors and women experiencing severe symptoms of menopause.[3]
There has been interest in using stellate ganglion blocks to treat PTSD, particularly in combat veterans. A 2017 review of the evidence from the VA Evidence-based Synthesis Program found that while the procedure had been reported as effective in unblinded case series, the evidence from randomized controlled trials remained inconclusive.[4]
Nerve fibers from the stellate ganglion go up the superior cervical sympathetic chain and into the pterygopalatine (sphenopalatine) ganglion (SPG). SPG blocks have been shown to reduce anxiety, headaches, migraines, cancer pain and other disorders.[5] Self-administration of SPG blocks (SASPGB) is another method of delivering sphenopalatine blockade and indirect stellate ganglion blockade.
Complications associated with a stellate ganglion block include Horner's syndrome, accidental intra-arterial or intravenous injection, difficulty swallowing, vocal cord paralysis, epidural spread of local anaesthetic, and pneumothorax.
Blunt needling of the stellate ganglion with an acupuncture needle is used in traditional Chinese medicine to decrease sympathetically mediated symptoms as well.
Block of the stellate ganglion has also been explored in coronary artery bypass surgery,[6] as well as posttraumatic stress disorder.[7]
Left stellectomy is a treatment strategy in prolonged QT syndrome because activity of the stellate ganglia drives prolonged QT. However, this therapy is only offered to patients who are already on a beta blocker and experience frequent shocks from an implantable cardioverter-defibrillator (ICD), because stellectomy causes Horner's syndrome.
Anatomy
The stellate ganglion lies in front of the neck of the first rib, and posterior to the common carotid artery.[8] The vertebral artery lies anterior to the ganglion as it has just originated from the subclavian artery. After passing over the ganglion, the artery enters the vertebral foramen and lies posterior to the anterior tubercle of C6 (Chassaignac's tubercle).[9]
References
- Gofeld, Michael; Shankar, Hariharan (2014-01-01), Benzon, Honorio T.; Rathmell, James P.; Wu, Christopher L.; Turk, Dennis C. (eds.), "56 - Peripheral and Visceral Sympathetic Blocks", Practical Management of Pain (Fifth Edition), Philadelphia: Mosby, pp. 755–767.e2, doi:10.1016/b978-0-323-08340-9.00056-6, ISBN 978-0-323-08340-9, retrieved 2020-11-18
- Petersohn, Jeffrey D. (2011-01-01), Lennard, Ted A.; Walkowski, Stevan; Singla, Aneesh K.; Vivian, David G. (eds.), "42 - Sympathetic Neural Blockade", Pain Procedures in Clinical Practice (Third Edition), Saint Louis: Hanley & Belfus, pp. 507–519, doi:10.1016/b978-1-4160-3779-8.10042-9, ISBN 978-1-4160-3779-8, retrieved 2020-11-18
- Lancet, 2008
- Peterson, Kim (February 2017). "Evidence Brief: Effectiveness of Stellate Ganglion Block for Treatment of Posttraumatic Stress Disorder (PTSD)". VA Evidence Synthesis Program Evidence Briefs [Internet]. VA Evidence Synthesis Program Reports. PMID 28742302.
- Shapira, Ira L. (11 April 2019). "Neuromuscular dentistry and the role of the autonomic nervous system: Sphenopalatine ganglion blocks and neuromodulation. An International College of Cranio Mandibular Orthopedics (ICCMO) position paper". Cranio. 37 (3): 201–206. doi:10.1080/08869634.2019.1592807. PMID 30973097. S2CID 108295446.
- Yildirim V, Akay HT, Bingol H, et al. (2007). "Pre-emptive stellate ganglion block increases the patency of radial artery grafts in coronary artery bypass surgery". Acta Anaesthesiologica Scandinavica. 51 (4): 434–40. doi:10.1111/j.1399-6576.2006.01260.x. PMID 17378781. S2CID 28530232.
- Piraccini, Emanuele; Chang, Ke-Vin (2020). "Stellate Ganglion Blocks". StatPearls. StatPearls Publishing LLC. PMID 29939575. Retrieved 22 June 2019.
- Tubbs, R. Shane; Goodrich, Dylan; Watanabe, Koichi; Loukas, Marios (2015-01-01), Tubbs, R. Shane; Rizk, Elias; Shoja, Mohammadali M.; Loukas, Marios (eds.), "Chapter 43 - Anatomic Landmarks for Selected Nerves of the Head, Neck, and Upper and Lower Limbs", Nerves and Nerve Injuries, San Diego: Academic Press, pp. 575–588, doi:10.1016/b978-0-12-410390-0.00045-7, ISBN 978-0-12-410390-0, retrieved 2020-11-18
- Raj, Practical Management of Pain, 3rd ed, pp656-657
Anatomy of the autonomic nervous system | |||||
|---|---|---|---|---|---|
| Head |
| ||||
| Neck |
| ||||
| Chest |
| ||||
| Abdomen |
| ||||
| Pelvis |
| ||||
| |||||