Telehealth
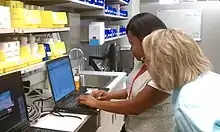
Telehealth is the distribution of health-related services and information via electronic information and telecommunication technologies.[1] It allows long-distance patient and clinician contact, care, advice, reminders, education, intervention, monitoring, and remote admissions.[2][3] Telemedicine is sometimes used as a synonym, or is used in a more limited sense to describe remote clinical services, such as diagnosis and monitoring. When rural settings, lack of transport, a lack of mobility, conditions due to outbreaks, epidemics or pandemics, decreased funding, or a lack of staff restrict access to care, telehealth may bridge the gap[4] as well as provide distance-learning; meetings, supervision, and presentations between practitioners; online information and health data management and healthcare system integration.[5] Telehealth could include two clinicians discussing a case over video conference; a robotic surgery occurring through remote access; physical therapy done via digital monitoring instruments, live feed and application combinations; tests being forwarded between facilities for interpretation by a higher specialist; home monitoring through continuous sending of patient health data; client to practitioner online conference; or even videophone interpretation during a consult.[1][2][5]

Telehealth versus telemedicine
Telehealth is sometimes discussed interchangeably with telemedicine, the latter being more common than the former. The Health Resources and Services Administration distinguishes telehealth from telemedicine in its scope, defining telemedicine only as describing remote clinical services, such as diagnosis and monitoring, while telehealth includes preventative, promotive, and curative care delivery.[1] This includes the above-mentioned non-clinical applications, like administration and provider education.[2][3]
The United States Department of Health and Human Services states that the term telehealth includes "non-clinical services, such as provider training, administrative meetings, and continuing medical education", and that the term telemedicine means "remote clinical services".[6] The World Health Organization uses telemedicine to describe all aspects of health care including preventive care.[7] The American Telemedicine Association uses the terms telemedicine and telehealth interchangeably, although it acknowledges that telehealth is sometimes used more broadly for remote health not involving active clinical treatments.[8]
eHealth is another related term, used particularly in the U.K. and Europe, as an umbrella term that includes telehealth, electronic medical records, and other components of health information technology.
Methods and modalities
Telehealth requires good Internet access by participants, usually in the form of a strong, reliable broadband connection, and broadband mobile communication technology of at least the fourth generation (4G) or long-term evolution (LTE) standard to overcome issues with video stability and bandwidth restrictions.[9][10][11] As broadband infrastructure has improved, telehealth usage has become more widely feasible.[1][2]
Healthcare providers often begin telehealth with a needs assessment which assesses hardships which can be improved by telehealth such as travel time, costs or time off work.[1][2] Collaborators, such as technology companies can ease the transition.[1]
Delivery can come within four distinct domains: live video (synchronous), store-and-forward (asynchronous), remote patient monitoring, and mobile health.[12]
Store and forward
Store-and-forward telemedicine involves acquiring medical data (like medical images, biosignals etc.) and then transmitting this data to a doctor or medical specialist at a convenient time for assessment offline.[8] It does not require the presence of both parties at the same time.[13] Dermatology (cf: teledermatology), radiology, and pathology are common specialties that are conducive to asynchronous telemedicine. A properly structured medical record preferably in electronic form should be a component of this transfer. The 'store-and-forward' process requires the clinician to rely on a history report and audio/video information in lieu of a physical examination.
Remote monitoring

Remote monitoring, also known as self-monitoring or testing, enables medical professionals to monitor a patient remotely using various technological devices. This method is primarily used for managing chronic diseases or specific conditions, such as heart disease, diabetes mellitus, or asthma. These services can provide comparable health outcomes to traditional in-person patient encounters, supply greater satisfaction to patients, and may be cost-effective.[14] Examples include home-based nocturnal dialysis[15] and improved joint management.[16]
Real-time interactive
Electronic consultations are possible through interactive telemedicine services which provide real-time interactions between patient and provider.[13] Videoconferencing has been used in a wide range of clinical disciplines and settings for various purposes including management, diagnosis, counseling and monitoring of patients.[17]
Videotelephony
Videotelephony comprises the technologies for the reception and transmission of audio-video signals by users at different locations, for communication between people in real-time.[18]
At the dawn of the technology, videotelephony also included image phones which would exchange still images between units every few seconds over conventional POTS-type telephone lines, essentially the same as slow scan TV systems.
Currently, videotelephony is particularly useful to the deaf and speech-impaired who can use them with sign language and also with a video relay service, and well as to those with mobility issues or those who are located in distant places and are in need of telemedical or tele-educational services.
Categories
Emergency care
%252C_Michael_Bedwell%252C_trains_Sailors_to_use_Battlefield_Medical_Information_Systems_Telemedicine_(BMIST)_equipped_Personal_Digital.jpg.webp)
Common daily emergency telemedicine is performed by SAMU Regulator Physicians in France, Spain, Chile and Brazil. Aircraft and maritime emergencies are also handled by SAMU centres in Paris, Lisbon and Toulouse.[19]
A recent study identified three major barriers to adoption of telemedicine in emergency and critical care units. They include:
- Regulatory challenges: related to the difficulty and cost of obtaining licensure across multiple states, malpractice protection and privileges at multiple facilities
- Financial barrier: lack of acceptance and reimbursement by government payers and some commercial insurance carriers, which places the investment burden squarely upon the hospital or healthcare system.
- Cultural barriers: occurring from the lack of desire, or unwillingness, of some physicians to adapt clinical paradigms for telemedicine applications.[20]
_01.JPG.webp)
Emergency Telehealth is also gaining acceptance in the United States. There are several modalities currently being practiced that include but are not limited to TeleTriage, TeleMSE and ePPE.
An example of telehealth in the field is when EMS arrives on scene of an incident and is able to take an EKG that is then sent directly to a physician at the hospital to be read. Therefore, allowing instant care and management.[21]
Telenursing
Telenursing refers to the use of telecommunications and information technology in order to provide nursing services in health care whenever a large physical distance exists between patient and nurse, or between any number of nurses. As a field it is part of telehealth, and has many points of contacts with other medical and non-medical applications, such as telediagnosis, teleconsultation, telemonitoring, etc.
Telenursing is achieving significant growth rates in many countries due to several factors: the preoccupation in reducing the costs of health care, an increase in the number of aging and chronically ill population, and the increase in coverage of health care to distant, rural, small or sparsely populated regions. Among its benefits, telenursing may help solve increasing shortages of nurses; to reduce distances and save travel time, and to keep patients out of hospital. A greater degree of job satisfaction has been registered among telenurses.[22]
In Australia, during January 2014, Melbourne tech startup Small World Social collaborated with the Australian Breastfeeding Association to create the first hands-free breastfeeding Google Glass application for new mothers.[23] The application, named Google Glass Breastfeeding app trial, allows mothers to nurse their baby while viewing instructions about common breastfeeding issues (latching on, posture etc.) or call a lactation consultant via a secure Google Hangout,[24] who can view the issue through the mother's Google Glass camera.[25] The trial was successfully concluded in Melbourne in April 2014, and 100% of participants were breastfeeding confidently.[26][27][28][29]
Telepalliative care
Palliative care is an interdisciplinary medical caregiving approach aimed at optimizing quality of life and mitigating suffering among people with serious, complex, and often terminal illnesses. In the past, palliative care was a disease specific approach, but today the World Health Organization (WHO) takes a broader approach suggesting that palliative care should be applied as early as possible to any chronic and fatal illness. As in many aspects of healthcare, telehealth is increasingly being used in palliative care [30] and is often referred to as telepalliative care.[31] The types of technology applied in telepalliative care are typically telecommunication technologies, such as video conferencing or messaging for follow-up, or digital symptom assessments through digital questionnaires generating alerts to health care professionals.[32] Telepalliative care has been shown to be a feasible approach to deliver palliative care among patients, caregivers and health care professionals.[33][32][34] Telepalliative care can provide an added support system that enable patients to remain at home through self-reporting of symptoms and tailoring care to specific patients.[34] Studies have shown that the use of telehealth in palliative care is mostly well received by patients, and that telepalliative care may improve access to health care professionals at home and enhance feelings of security and safety among patients receiving palliative care.[33] Further, telepalliative care may enable more efficient utilization of healthcare resources, promotes collaboration between different levels of healthcare and makes healthcare professionals more responsive to changes in patients' condition.[32]
Challenging aspects of the use of telehealth in palliative care have also been described. Generally, palliative care is a diverse medical specialty, involving interdisciplinary professionals from different professional traditions and cultures, delivering care to a heterogenous cohort of patients with diverse diseases, conditions and symptoms. This makes it a challenge to develop telehealth that is suitable for all patients and in all contexts of palliative care. Some of the barriers to telepalliative care relate to inflexible reporting of complex and fluctuating symptoms and circumstances using electronic questionnaires.[34] Further, palliative care emphasizes a holistic approach that should address existential, spiritual and mental distress related to serious illness.[35] However, few studies have included the self-reporting of existential or spiritual concerns, emotions, and well-being.[34] Healthcare professionals may also be uncomfortable providing emotional or psychological care remotely.[32] Palliative care has been characterized as high-touch rather than high-tech, limiting the interest in applying technological advancements when developing interventions.[36] To optimize the advantages and minimize the challenges with the use of telehealth in home-based palliative care, future research should include users in the design and development process. Understanding the potential of telehealth to support therapeutic relationships between patients and health care professionals and being aware of the possible difficulties and tensions it may create are critical to its successful and acceptable use.[32][34]
Telepharmacy
Telepharmacy is the delivery of pharmaceutical care via telecommunications to patients in locations where they may not have direct contact with a pharmacist. It is an instance of the wider phenomenon of telemedicine, as implemented in the field of pharmacy. Telepharmacy services include drug therapy monitoring, patient counseling, prior authorization and refill authorization for prescription drugs, and monitoring of formulary compliance with the aid of teleconferencing or videoconferencing. Remote dispensing of medications by automated packaging and labeling systems can also be thought of as an instance of telepharmacy. Telepharmacy services can be delivered at retail pharmacy sites or through hospitals, nursing homes, or other medical care facilities. Health outcomes appear similar when pharmacy services are delivered by telepharmacy compared to traditional service delivery.[37]
The term can also refer to the use of videoconferencing in pharmacy for other purposes, such as providing education, training, and management services to pharmacists and pharmacy staff remotely.[38]
Telepsychiatry
.jpg.webp)
Telepsychiatry or telemental health refers to the use of telecommunications technology (mostly videoconferencing and phone calls) to deliver psychiatric care remotely for people with mental health conditions. It is a branch of telemedicine.[39][40]
Telepsychiatry can be effective in treating people with mental health conditions. In the short-term it can be as acceptable and effective as face-to-face care.[41]
It can improve access to mental health services for some but might also represent a barrier for those lacking access to a suitable device, the internet or the necessary digital skills. Factors such as poverty that are associated with lack of internet access are also associated with greater risk of mental health problems, making digital exclusion an important problem of telemental health services.[41]
During the COVID-19 pandemic mental health services were adapted to telemental health in high-income countries. It proved effective and acceptable for use in an emergency situation but there were concerns regarding its long-term implementation.[42]Teledentistry
Teledentistry is the use of information technology and telecommunications for dental care, consultation, education, and public awareness in the same manner as telehealth and telemedicine.
Teleaudiology
Tele-audiology is the utilization of telehealth to provide audiological services and may include the full scope of audiological practice. This term was first used by Dr Gregg Givens in 1999 in reference to a system being developed at East Carolina University in North Carolina, US.
Teleneurology
Teleneurology describes the use of mobile technology to provide neurological care remotely, including care for stroke, movement disorders like Parkinson's disease, seizure disorders (e.g., epilepsy), etc. The use of teleneurology gives us the opportunity to improve health care access for billions around the globe, from those living in urban locations to those in remote, rural locations. Evidence shows that individuals with Parkinson's disease prefer personal connection with a remote specialist to their local clinician. Such home care is convenient but requires access to and familiarity with internet.[43][44] A 2017 randomized controlled trial of "virtual house calls" or video visits with individuals diagnosed with Parkinson disease evidences patient preference for the remote specialist vs their local clinician after one year.[44] Teleneurology for patients with Parkison's disease is found to be cheaper than in person visits by reducing transportation and travel time[45][46] A recent systematic review by Ray Dorsey et al.[43] describes both the limitations and potential benefits of teleneurology to improve care for patients with chronic neurological conditions, especially in low-income countries. White, well educated and technologically savvy people are the biggest consumers of telehealth services for Parkinson's disease.[45][46] as compared to ethnic minorities in the US.[46]
Teleneurosurgery
Telemedicine in neurosurgery was historically primarily used for follow-up visits by patients that had to travel far to undergo surgery.[47] In the last decade, telemedicine was also used for remote ICU rounding as well as prompt evaluation for acute ischemic stroke and administration of IV alteplase in conjunction with Neurology.[48][49] From the onset of the COVID-19 pandemic, there was a rapid surge in the use of telemedicine across all divisions of neurosurgery: vascular, oncology, spine, and functional neurosurgery. Not only for follow-up visits, but it has gained popularity for seeing new patients or following established patients regardless of whether they underwent surgery.[50][51] Telemedicine is not limited to direct patient care only; there are a number of new research groups and companies focused on using telemedicine for clinical trials involving patients with neurosurgical diagnoses.
Teleneuropsychology
Teleneuropsychology is the use of telehealth/videoconference technology for the remote administration of neuropsychological tests. Neuropsychological tests are used to evaluate the cognitive status of individuals with known or suspected brain disorders and provide a profile of cognitive strengths and weaknesses. Through a series of studies, there is growing support in the literature showing that remote videoconference-based administration of many standard neuropsychological tests results in test findings that are similar to traditional in-person evaluations, thereby establishing the basis for the reliability and validity of teleneuropsychological assessment.[52][53][54][55][56][57]
Telenutrition
Telenutrition refers to the use of video conferencing/ telephony to provide online consultation by a nutritionist or dietician. Patient or clients upload their vital statistics, diet logs, food pictures etc. on a telenutrition portal which are then used by nutritionist or dietician to analyze their current health condition. Nutritionist or dietician can then set goals for their respective client/ patients and monitor their progress regularly by follow-up consultations.
Telenutrition portals can help people seek remote consultation for themselves and/or their family. This can be extremely helpful for elderly or bed ridden patients who can consult their dietician from comfort of their homes.
Telenutrition showed to be feasible and the majority of patients trusted the nutritional televisits, in place of the scheduled but not provided follow-up visits during the lockdown of the COVID-19 pandemic.[58]
Telerehabilitation

Telerehabilitation (or e-rehabilitation[59][60]) is the delivery of rehabilitation services over telecommunication networks and the Internet. Most types of services fall into two categories: clinical assessment (the patient's functional abilities in his or her environment), and clinical therapy. Some fields of rehabilitation practice that have explored telerehabilitation are: neuropsychology, speech–language pathology, audiology, occupational therapy, and physical therapy. Telerehabilitation can deliver therapy to people who cannot travel to a clinic because the patient has a disability or because of travel time. Telerehabilitation also allows experts in rehabilitation to engage in a clinical consultation at a distance.
Most telerehabilitation is highly visual. As of 2014, the most commonly used mediums are webcams, videoconferencing, phone lines, videophones and webpages containing rich web applications. The visual nature of telerehabilitation technology limits the types of rehabilitation services that can be provided. It is most widely used for neuropsychological rehabilitation; fitting of rehabilitation equipment such as wheelchairs, braces or artificial limbs; and in speech-language pathology. Rich web applications for neuropsychological rehabilitation (aka cognitive rehabilitation) of cognitive impairment (from many etiologies) were first introduced in 2001. This endeavor has expanded as a teletherapy application for cognitive skills enhancement programs for school children. Tele-audiology (hearing assessments) is a growing application. Currently, telerehabilitation in the practice of occupational therapy and physical therapy is limited, perhaps because these two disciplines are more "hands on".
Two important areas of telerehabilitation research are (1) demonstrating equivalence of assessment and therapy to in-person assessment and therapy, and (2) building new data collection systems to digitize information that a therapist can use in practice. Ground-breaking research in telehaptics (the sense of touch) and virtual reality may broaden the scope of telerehabilitation practice, in the future.
In the United States, the National Institute on Disability and Rehabilitation Research's (NIDRR)[61] supports research and the development of telerehabilitation. NIDRR's grantees include the "Rehabilitation Engineering and Research Center" (RERC) at the University of Pittsburgh, the Rehabilitation Institute of Chicago, the State University of New York at Buffalo, and the National Rehabilitation Hospital in Washington DC. Other federal funders of research are the Veterans Health Administration, the Health Services Research Administration in the US Department of Health and Human Services, and the Department of Defense.[62] Outside the United States, excellent research is conducted in Australia and Europe.
Only a few health insurers in the United States, and about half of Medicaid programs,[63] reimburse for telerehabilitation services. If the research shows that teleassessments and teletherapy are equivalent to clinical encounters, it is more likely that insurers and Medicare will cover telerehabilitation services.
In India, the Indian Association of Chartered Physiotherapists (IACP) provides telerehabilitation facilities. With the support and collaboration of local clinics and private practitioners and the Members IACP, IACP runs the facility, named Telemedicine. IACP has maintained an internet-based list of their members on their website, through which patients can make online appointments.
Teletrauma care
Telemedicine can be utilized to improve the efficiency and effectiveness of the delivery of care in a trauma environment. Examples include:
Telemedicine for trauma triage: using telemedicine, trauma specialists can interact with personnel on the scene of a mass casualty or disaster situation, via the internet using mobile devices, to determine the severity of injuries. They can provide clinical assessments and determine whether those injured must be evacuated for necessary care. Remote trauma specialists can provide the same quality of clinical assessment and plan of care as a trauma specialist located physically with the patient.[64]
Telemedicine for intensive care unit (ICU) rounds: Telemedicine is also being used in some trauma ICUs to reduce the spread of infections. Rounds are usually conducted at hospitals across the country by a team of approximately ten or more people to include attending physicians, fellows, residents and other clinicians. This group usually moves from bed to bed in a unit discussing each patient. This aids in the transition of care for patients from the night shift to the morning shift, but also serves as an educational experience for new residents to the team. A new approach features the team conducting rounds from a conference room using a video-conferencing system. The trauma attending, residents, fellows, nurses, nurse practitioners, and pharmacists are able to watch a live video stream from the patient's bedside. They can see the vital signs on the monitor, view the settings on the respiratory ventilator, and/or view the patient's wounds. Video-conferencing allows the remote viewers two-way communication with clinicians at the bedside.[65]
Telemedicine for trauma education: some trauma centers are delivering trauma education lectures to hospitals and health care providers worldwide using video conferencing technology. Each lecture provides fundamental principles, firsthand knowledge and evidenced-based methods for critical analysis of established clinical practice standards, and comparisons to newer advanced alternatives. The various sites collaborate and share their perspective based on location, available staff, and available resources.[66]
Telemedicine in the trauma operating room: trauma surgeons are able to observe and consult on cases from a remote location using video conferencing. This capability allows the attending to view the residents in real time. The remote surgeon has the capability to control the camera (pan, tilt and zoom) to get the best angle of the procedure while at the same time providing expertise in order to provide the best possible care to the patient.[67]
Telecardiology
ECGs, or electrocardiographs, can be transmitted using telephone and wireless. Willem Einthoven, the inventor of the ECG, actually did tests with transmission of ECG via telephone lines. This was because the hospital did not allow him to move patients outside the hospital to his laboratory for testing of his new device. In 1906 Einthoven came up with a way to transmit the data from the hospital directly to his lab.[68][69]
Transmission of ECGs
One of the oldest known telecardiology systems for teletransmissions of ECGs was established in Gwalior, India in 1975 at GR Medical college by Ajai Shanker, S. Makhija, P.K. Mantri using an indigenous technique for the first time in India.
This system enabled wireless transmission of ECG from the moving ICU van or the patients home to the central station in ICU of the department of Medicine. Transmission using wireless was done using frequency modulation which eliminated noise. Transmission was also done through telephone lines. The ECG output was connected to the telephone input using a modulator which converted ECG into high frequency sound. At the other end a demodulator reconverted the sound into ECG with a good gain accuracy. The ECG was converted to sound waves with a frequency varying from 500 Hz to 2500 Hz with 1500 Hz at baseline.
This system was also used to monitor patients with pacemakers in remote areas. The central control unit at the ICU was able to correctly interpret arrhythmia. This technique helped medical aid reach in remote areas.[70]
In addition, electronic stethoscopes can be used as recording devices, which is helpful for purposes of telecardiology. There are many examples of successful telecardiology services worldwide.
In Pakistan three pilot projects in telemedicine were initiated by the Ministry of IT & Telecom, Government of Pakistan (MoIT) through the Electronic Government Directorate in collaboration with Oratier Technologies (a pioneer company within Pakistan dealing with healthcare and HMIS) and PakDataCom (a bandwidth provider). Three hub stations through were linked via the Pak Sat-I communications satellite, and four districts were linked with another hub. A 312 Kb link was also established with remote sites and 1 Mbit/s bandwidth was provided at each hub. Three hubs were established: the Mayo Hospital (the largest hospital in Asia), JPMC Karachi and Holy Family Rawalpindi. These 12 remote sites were connected and on average of 1,500 patients were treated per month per hub. The project was still running smoothly after two years.[71]
Wireless ambulatory ECG technology, moving beyond previous ambulatory ECG technology such as the Holter monitor, now includes smartphones and Apple Watches which can perform at-home cardiac monitoring and send the data to a physician via the internet.[72]
Teleradiology

Teleradiology is the ability to send radiographic images (x-rays, CT, MR, PET/CT, SPECT/CT, MG, US...) from one location to another.[73] For this process to be implemented, three essential components are required, an image sending station, a transmission network, and a receiving-image review station. The most typical implementation are two computers connected via the Internet. The computer at the receiving end will need to have a high-quality display screen that has been tested and cleared for clinical purposes. Sometimes the receiving computer will have a printer so that images can be printed for convenience.
The teleradiology process begins at the image sending station. The radiographic image and a modem or other connection are required for this first step. The image is scanned and then sent via the network connection to the receiving computer.
Today's high-speed broadband based Internet enables the use of new technologies for teleradiology: the image reviewer can now have access to distant servers in order to view an exam. Therefore, they do not need particular workstations to view the images; a standard personal computer (PC) and digital subscriber line (DSL) connection is enough to reach Keosys' central server. No particular software is necessary on the PC and the images can be reached from anywhere in the world.
Teleradiology is the most popular use for telemedicine and accounts for at least 50% of all telemedicine usage.
Telepathology
Telepathology is the practice of pathology at a distance. It uses telecommunications technology to facilitate the transfer of image-rich pathology data between distant locations for the purposes of diagnosis, education, and research.[74][75] Performance of telepathology requires that a pathologist selects the video images for analysis and the rendering diagnoses. The use of "television microscopy", the forerunner of telepathology, did not require that a pathologist have physical or virtual "hands-on" involvement is the selection of microscopic fields-of-view for analysis and diagnosis.
A pathologist, Ronald S. Weinstein, M.D., coined the term "telepathology" in 1986. In an editorial in a medical journal, Weinstein outlined the actions that would be needed to create remote pathology diagnostic services.[76] He, and his collaborators, published the first scientific paper on robotic telepathology.[77] Weinstein was also granted the first U.S. patents for robotic telepathology systems and telepathology diagnostic networks.[78] Weinstein is known to many as the "father of telepathology".[79] In Norway, Eide and Nordrum implemented the first sustainable clinical telepathology service in 1989.[80] This is still in operation, decades later. A number of clinical telepathology services have benefited many thousands of patients in North America, Europe, and Asia.
Telepathology has been successfully used for many applications including the rendering histopathology tissue diagnoses, at a distance, for education, and for research. Although digital pathology imaging, including virtual microscopy, is the mode of choice for telepathology services in developed countries, analog telepathology imaging is still used for patient services in some developing countries.
Teledermatology
Teledermatology allows dermatology consultations over a distance using audio, visual and data communication, and has been found to improve efficiency, access to specialty care, and patient satisfaction.[81][82] Applications comprise health care management such as diagnoses, consultation and treatment as well as (continuing medical) education.[83][84][85] The dermatologists Perednia and Brown were the first to coin the term teledermatology in 1995, where they described the value of a teledermatologic service in a rural area underserved by dermatologists.[86]
Teleophthalmology
Teleophthalmology is a branch of telemedicine that delivers eye care through digital medical equipment and telecommunications technology. Today, applications of teleophthalmology encompass access to eye specialists for patients in remote areas, ophthalmic disease screening, diagnosis and monitoring; as well as distant learning. Teleophthalmology may help reduce disparities by providing remote, low-cost screening tests such as diabetic retinopathy screening to low-income and uninsured patients.[87][88] In Mizoram, India, a hilly area with poor roads, between 2011 and 2015, teleophthalmology provided care to over 10,000 patients. These patients were examined by ophthalmic assistants locally but surgery was done on appointment after the patient images were viewed online by eye surgeons in the hospital 6–12 hours away. Instead of an average five trips for say, a cataract procedure, only one was required for surgery alone as even post-op care like removal of stitches and appointments for glasses was done locally. There were large cost savings in travel as well.[89]
In the United States, some companies allow patients to complete an online visual exam and within 24 hours receive a prescription from an optometrist valid for eyeglasses, contact lenses, or both. Some US states such as Indiana have attempted to ban these companies from doing business.[90]
Telesurgery
Remote surgery (also known as telesurgery) is the ability for a doctor to perform surgery on a patient even though they are not physically in the same location. It is a form of telepresence. Remote surgery combines elements of robotics, cutting-edge telecommunications such as high-speed data connections, telehaptics and elements of management information systems. While the field of robotic surgery is fairly well established, most of these robots are controlled by surgeons at the location of the surgery.
Remote surgery is remote work for surgeons, where the physical distance between the surgeon and the patient is immaterial. It promises to allow the expertise of specialized surgeons to be available to patients worldwide, without the need for patients to travel beyond their local hospital.[91]
Remote surgery or telesurgery is performance of surgical procedures where the surgeon is not physically in the same location as the patient, using a robotic teleoperator system controlled by the surgeon. The remote operator may give tactile feedback to the user. Remote surgery combines elements of robotics and high-speed data connections. A critical limiting factor is the speed, latency and reliability of the communication system between the surgeon and the patient, though trans-Atlantic surgeries have been demonstrated.
Teleabortion
Telemedicine has been used globally to increase access to abortion care, specifically medical abortion, in environments where few abortion care providers exist or abortion is legally restricted. Clinicians are able to virtually provide counseling, review screening tests, observe the administration of an abortion medication, and directly mail abortion pills to people.[92] In 2004, Women on Web (WoW), Amsterdam, started offering online consultations, mostly to people living in areas where abortion was legally restricted, informing them how to safely use medical abortion drugs to end a pregnancy.[92] People contact the Women on Web service online; physicians review any necessary lab results or ultrasounds, mail mifepristone and misoprostol pills to people, then follow up through online communication.[93] In the United States, medical abortion was introduced as a telehealth service in Iowa by Planned Parenthood of the Heartland in 2008 to allow a patient at one health facility to communicate via secure video with a health provider at another facility.[94] In this model a person seeking abortion care must come to a health facility. An abortion care provider communicates with the person located at another site using clinic-to-clinic videoconferencing to provide medical abortion after screening tests and consultation with clinic staff. In 2018, the website Aid Access was launched by the founder of Women on Web, Dr. Rebecca Gomperts. It offers a similar service as Women on Web in the United States, but the medications are prescribed to an Indian pharmacy, then mailed to the United States.
The TelAbortion study conducted by Gynuity Health Projects, with special approval from the U.S. Food and Drug Administration (FDA), aims to increase access to medical abortion care without requiring an in-person visit to a clinic.[95][96][94] This models was expanded during the COVID-19 pandemic and as of March 2020 exists in 13 U.S. states and has enrolled over 730 people in the study.[97][96] The person receives counseling and instruction from an abortion care provider via videoconference from a location of their choice. The medications necessary for the abortion, mifepristone and misoprostol, are mailed directly to the person and they have a follow-up video consultation in 7–14 days. A systematic review of telemedicine abortion has found the practice to be safe, effective, efficient, and satisfactory.[92]
In the United States, eighteen states require the clinician to be physically present during the administration of medications for abortion which effectively bans telehealth of medication abortion: five states explicitly ban telemedicine for medication abortion, while thirteen states require the prescriber (usually required to be a physician) to be physically present with the patient.[98][99] In the UK, the Royal College of Obstetricians and Gynecologists approved a no-test protocol for medication abortion, with mifepristone available through a minimal-contact pick-up or by mail.[100]
Other specialist care delivery
Telemedicine can facilitate specialty care delivered by primary care physicians according to a controlled study of the treatment of hepatitis C.[101] Various specialties are contributing to telemedicine, in varying degrees.
In light of the COVID-19 pandemic, primary care physicians have relied on telehealth to continue to provide care in outpatient settings.[102] The transition to virtual health has been beneficial in providing patients access to care (especially care that does not require a physical exam e.g. medication changes, minor health updates) and avoid putting patients at risk of COVID-19. This included providing services to pediatric patients during the pandemic, where issues of last minute cancelation and rescheduling were frequently related to a lack of technicality and engagement, two factors often understudied in the literature.[103]
Telemedicine has also been beneficial in facilitating medical education to students while still allowing for adequate social distancing during the COVID-19 pandemic. Many medical schools have shifted to alternate forms of virtual curriculum and are still able to engage in meaningful telehealth encounters with patients.[104][105]
Medication assisted treatment (MAT) is the treatment of opioid use disorder (OUD) with medications, often in combination with behavioral therapy[106] As a response to the COVID-19 pandemic the use of telemedicine has been granted by the Drug Enforcement Administration to start or maintain people OUD on buprenorphine (trade name Suboxone) via telemedicine without the need for an initial in-person examination.[107] On March 31, 2020, QuickMD became the first national TeleMAT service in the United States to provide Medication-assisted Treatment with Suboxone online – without the need of an in-person visit; with others announcing to follow soon.[108]
Major developments
In policy
Telehealth is a modern form of health care delivery. Telehealth breaks away from traditional health care delivery by using modern telecommunication systems including wireless communication methods.[109][110] Traditional health is legislated through policy to ensure the safety of medical practitioners and patients. Consequently, since telehealth is a new form of health care delivery that is now gathering momentum in the health sector, many organizations have started to legislate the use of telehealth into policy.[110] In New Zealand, the Medical Council has a statement about telehealth on their website. This illustrates that the medical council has foreseen the importance that telehealth will have on the health system and have started to introduce telehealth legislation to practitioners along with government.[111]
Transition to mainstream
Traditional use of telehealth services has been for specialist treatment. However, there has been a paradigm shift and telehealth is no longer considered a specialist service.[112] This development has ensured that many access barriers are eliminated, as medical professionals are able to use wireless communication technologies to deliver health care. This is evident in rural communities. For individuals living in rural communities, specialist care can be some distance away, particularly in the next major city. Telehealth eliminates this barrier as health professionals are able to conduct medical consultations through the use of wireless communication technologies. However, this process is dependent on both parties having Internet access.[113][114]
Telehealth allows the patient to be monitored between physician office visits which can improve patient health. Telehealth also allows patients to access expertise which is not available in their local area. This remote patient monitoring ability enables patients to stay at home longer and helps avoid unnecessary hospital time. In the long-term, this could potentially result in less burdening of the healthcare system and consumption of resources.[1][115]
During the COVID-19 pandemic, there were large increases in the use of telemedicine for primary care visits within the United States, increasing from an average of 1.4 million visits in Q2 of 2018 and 2019 to 35 million visits in Q2 2020, according to data from IQVIA.[116] The telehealth market is expected to grow at 40% a year in 2021. Use of telemedicine by General Practitioners in the UK rose from 20 to 30% pre-COVID to almost 80% by the beginning of 2021. More than 70% of practitioners and patients were satisfied with this.[117] Boris Johnson was said to have "piled pressure on GPs to offer more in-person consultations" supporting a campaign largely orchestrated by the Daily Mail. The Royal College of General Practitioners said that a patient "right" to have face-to-face appointments if they wished was "undeliverable".[118]
Technology advancement
The technological advancement of wireless communication devices is a major development in telehealth.[119] This allows patients to self-monitor their health conditions and to not rely as much on health care professionals. Furthermore, patients are more willing to stay on their treatment plans as they are more invested and included in the process as the decision-making is shared.[120][121] Technological advancement also means that health care professionals are able to use better technologies to treat patients for example in maternal care[122] and surgery. A 2023 study published in the Journal of the American College of Surgeons showed telemedicine as making a positive impact, with expectations exceeded for those physicians and patients who had consulted online for surgeries.[123] Technological developments in telehealth are essential to improve health care, especially the delivery of healthcare services, as resources are finite along with an ageing population that is living longer.[119][120][121]
Licensing
U.S. licensing and regulatory issues
Restrictive licensure laws in the United States require a practitioner to obtain a full license to deliver telemedicine care across state lines. Typically, states with restrictive licensure laws also have several exceptions (varying from state to state) that may release an out-of-state practitioner from the additional burden of obtaining such a license. A number of states require practitioners who seek compensation to frequently deliver interstate care to acquire a full license.
If a practitioner serves several states, obtaining this license in each state could be an expensive and time-consuming proposition. Even if the practitioner never practices medicine face-to-face with a patient in another state, he/she still must meet a variety of other individual state requirements, including paying substantial licensure fees, passing additional oral and written examinations, and traveling for interviews.
In 2008, the U.S. passed the Ryan Haight Act which required face-to-face or valid telemedicine consultations prior to receiving a prescription.[124]
State medical licensing boards have sometimes opposed telemedicine; for example, in 2012 electronic consultations were illegal in Idaho, and an Idaho-licensed general practitioner was punished by the board for prescribing an antibiotic, triggering reviews of her licensure and board certifications across the country.[125] Subsequently, in 2015 the state legislature legalized electronic consultations.[125]
In 2015, Teladoc filed suit against the Texas Medical Board over a rule that required in-person consultations initially; the judge refused to dismiss the case, noting that antitrust laws apply to state medical boards.[126]
Major implications and impacts
Telehealth allows multiple, varying disciplines to merge and deliver a potentially more uniform level of care, using technology. As telehealth proliferates mainstream healthcare, it challenges notions of traditional healthcare delivery. Some populations experience better quality, access and more personalized health care.[127][128]
Health promotion

Telehealth can also increase health promotion efforts. These efforts can now be more personalised to the target population and professionals can extend their help into homes or private and safe environments in which patients of individuals can practice, ask and gain health information.[115][121][129] Health promotion using telehealth has become increasingly popular in underdeveloped countries where there are very poor physical resources available. There has been a particular push toward mHealth applications as many areas, even underdeveloped ones have mobile phone and smartphone coverage.[130][131][132]
In a 2015 article reviewing research on the use of a mobile health application in the United Kingdom,[133] authors describe how a home-based application helped patients manage and monitor their health and symptoms independently. The mobile health application allows people to rapidly self-report their symptoms – 95% of patients were able to report their daily symptoms in less than 100 seconds, which is less than the 5 minutes (plus commuting) taken to measure vital signs by nurses in hospitals.[134] Online applications allow patients to remain at home to keep track of the progression of their chronic illnesses. The downside of using mHealth applications is that not everyone, especially in developing countries, has daily access to internet or electronic devices.[135]
In developed countries, health promotion efforts using telehealth have been met with some success. The Australian hands-free breastfeeding Google Glass application reported promising results in 2014. This application made in collaboration with the Australian Breastfeeding Association and a tech startup called Small World Social, helped new mothers learn how to breastfeed.[136][137][138] Breastfeeding is beneficial to infant health and maternal health and is recommended by the World Health Organisation and health organisations all over the world.[139][140] Widespread breastfeeding can prevent 820,000 infant deaths globally but the practice is often stopped prematurely or intents to do are disrupted due to lack of social support, know-how or other factors.[140] This application gave mother's hands-free information on breastfeeding, instructions on how to breastfeed and also had an option to call a lactation consultant over Google Hangout. When the trial ended, all participants were reported to be confident in breastfeeding.[138]
Health care quality and barriers to adoption
A scientific review indicates that, in general, outcomes of telemedicine are or can be as good as in-person care with health care use staying similar.[141]
.webp.png.webp)
Advantages of the nonexclusive adoption of already existing telemedicine technologies such as smartphone videotelephony may include reduced infection risks,[143] increased control of disease during epidemic conditions,[144] improved access to care,[145] reduced stress and exposure to other pathogens[146][147] during illness for better recovery, reduced time[148] and labor costs, efficient more accessible matching of patients with particular symptoms and clinicians who are experts for such, and reduced travel while disadvantages may include privacy breaches (e.g. due to software backdoors and vulnerabilities or sale of data), dependability on Internet access[143] and, depending on various factors, increased health care use.
Theoretically, the whole health system could benefit from telehealth. There are indications telehealth consumes fewer resources and requires fewer people to operate it with shorter training periods to implement initiatives.[12] Commenters suggested that lawmakers may fear that making telehealth widely accessible, without any other measures, would lead to patients using unnecessary health care services.[145] Telemedicine could also be used for connected networks between health care professionals.[149]
Telemedicine also can eliminate the possible transmission of infectious diseases or parasites between patients and medical staff. This is particularly an issue where MRSA is a concern. Additionally, some patients who feel uncomfortable in a doctors office may do better remotely. For example, white coat syndrome may be avoided. Patients who are home-bound and would otherwise require an ambulance to move them to a clinic are also a consideration.
However, whether or not the standard of health care quality is increasing is debatable, with some literature refuting such claims.[128][150][151] Research has reported that clinicians find the process difficult and complex to deal with.[150][152] Furthermore, there are concerns around informed consent, legality issues as well as legislative issues. A recent study also highlighted that the swift and large-scale implementation of telehealth across the United Kingdom NHS Allied Health Professional (AHP) services might increase disparities in health care access for vulnerable populations with limited digital literacy.[153] Although health care may become affordable with the help of technology, whether or not this care will be "good" is the issue.[128] Many patient experience studies indicate high satisfaction with telemedicine.[154]
Major problems with increasing adoption include technically challenged staff, resistance to change or habits[146] and age of patient. Focused policy could eliminate several barriers.[155]
A review lists a number of potentially good practices and pitfalls, recommending the use of "virtual handshakes" for confirming identity, taking consent for conducting remote consultation over a conventional meeting, and professional standardized norms for protecting patient privacy and confidentiality.[156] It also found that the COVID-19 pandemic substantially increased, voluntarily, the adoption of telephone or video consultation and suggests that telemedicine technology "is a key factor in delivery of health care in the future".[156]
Economic evaluations
Due to its digital nature it is often assumed that telehealth saves the health system money. However, the evidence to support this is varied. When conducting economic evaluations of telehealth services, the individuals evaluating them need to be aware of potential outcomes and extraclinical benefits of the telehealth service.[157] Economic viability relies on the funding model within the country being examined (public vs private), the consumers willingness-to-pay, and the expected remuneration by the clinicians or commercial entities providing the services (examples of research on these topics from teledermoscopy in Australia)[158][159][160]
In a UK telehealth trial done in 2011, it was reported that the cost of health could be dramatically reduced with the use of telehealth monitoring. The usual cost of in vitro fertilisation (IVF) per cycle would be around $15,000; with telehealth it was reduced to $800 per patient.[161] In Alaska the Federal Health Care Access Network, which connects 3,000 healthcare providers to communities, engaged in 160,000 telehealth consultations from 2001 and saved the state $8.5 million in travel costs for just Medicaid patients.[162]
Digital interventions for mental health conditions seem to be cost-effective compared to no intervention or non-therapeutic responses such as monitoring. However, when compared to in-person therapy or medication their added value is currently uncertain.[163]
Beneficial enablements
Telemedicine can be beneficial to patients in isolated communities and remote regions, who can receive care from doctors or specialists far away without the patient having to travel to visit them.[164] Recent developments in mobile collaboration technology can allow healthcare professionals in multiple locations to share information and discuss patient issues as if they were in the same place.[165] Remote patient monitoring through mobile technology can reduce the need for outpatient visits and enable remote prescription verification and drug administration oversight, potentially significantly reducing the overall cost of medical care.[166] It may also be preferable for patients with limited mobility, for example, patients with Parkinson's disease.[43] Telemedicine can also facilitate medical education by allowing workers to observe experts in their fields and share best practices more easily.[167]
During war and disasters
Remote surgery and types of videoconferencing for sharing expertise (e.g. ad hoc assistance) have been and could be used to support doctors in Ukraine during the 2022 Russian invasion of Ukraine.[168]
Nonclinical uses
- Distance education including continuing medical education, grand rounds, and patient education[3]
- administrative uses including meetings among telehealth networks, supervision, and presentations
- research on telehealth
- online information and health data management
- healthcare system integration
- asset identification, listing, and patient to asset matching, and movement
- overall healthcare system management
- patient movement and remote admission
- Physical distancing to prevent transmission of communicable diseases[169][170][171]
Limitations and restrictions
While many branches of medicine have wanted to fully embrace telehealth for a long time, there are certain risks and barriers which bar the full amalgamation of telehealth into best practice. For a start, it is dubious as to whether a practitioner can fully leave the "hands-on" experience behind.[128] Although it is predicted that telehealth will replace many consultations and other health interactions, it cannot yet fully replace a physical examination, this is particularly so in diagnostics, rehabilitation or mental health.[128]
The benefits posed by telehealth challenge the normative means of healthcare delivery set in both legislation and practice. Therefore, the growing prominence of telehealth is starting to underscore the need for updated regulations, guidelines and legislation which reflect the current and future trends of healthcare practices.[2][128] Telehealth enables timely and flexible care to patients wherever they may be; although this is a benefit, it also poses threats to privacy, safety , medical licensing and reimbursement. When a clinician and patient are in different locations, it is difficult to determine which laws apply to the context.[172] Once healthcare crosses borders different state bodies are involved in order to regulate and maintain the level of care that is warranted to the patient or telehealth consumer. As it stands, telehealth is complex with many grey areas when put into practice especially as it crosses borders. This effectively limits the potential benefits of telehealth.[2][128]
An example of these limitations include the current American reimbursement infrastructure, where Medicare will reimburse for telehealth services only when a patient is living in an area where specialists are in shortage, or in particular rural counties. The area is defined by whether it is a medical facility as opposed to a patient's' home. The site that the practitioner is in, however, is unrestricted. Medicare will only reimburse live video (synchronous) type services, not store-and-forward, mhealth or remote patient monitoring (if it does not involve live-video). Some insurers currently will reimburse telehealth, but not all yet. So providers and patients must go to the extra effort of finding the correct insurers before continuing. Again in America, states generally tend to require that clinicians are licensed to practice in the surgery' state, therefore they can only provide their service if licensed in an area that they do not live in themselves.[125]
More specific and widely reaching laws, legislations and regulations will have to evolve with the technology. They will have to be fully agreed upon, for example, will all clinicians need full licensing in every community they provide telehealth services too, or could there be a limited use telehealth licence? Would the limited use licence cover all potential telehealth interventions, or only some? Who would be responsible if an emergency was occurring and the practitioner could not provide immediate help – would someone else have to be in the room with the patient at all consult times? Which state, city or country would the law apply in when a breach or malpractice occurred? [128][173]
A major legal action prompt in telehealth thus far has been issues surrounding online prescribing and whether an appropriate clinician-patient relationship can be established online to make prescribing safe, making this an area that requires particular scrutiny.[127] It may be required that the practitioner and patient involved must meet in person at least once before online prescribing can occur, or that at least a live-video conference must occur, not just impersonal questionnaires or surveys to determine need.[174]
Telehealth has some potential for facilitating self-management techniques in health care, but for patients to benefit from it, the appropriate contact with, and relationship, between doctor and patient must be established first.[175] This would start with an online consultation, providing patients with techniques and tools that help them participate in healthy behaviors, and initiating a collaborative partnership between health care professionals and patient.[176] Self-management strategies fall into a broader category called patient activation, which is defined as a "patients' willingness and ability to take independent actions to manage their health."[177] It can be achieved by increasing patients' knowledge and confidence in coping with and managing their own disease through a "regular assessment of progress [...] and problem-solving support."[176] Teaching patients about their conditions and ways to cope with chronic illnesses will allow them to be knowledgeable about their disease and willing to manage it, improving their everyday life. Without a focus on the doctor-patient relationship and on the patient's understanding, telehealth cannot improve the quality of life of patients, despite the benefit of allowing them to do their medical check-ups from the comfort of their home.
The downsides of telemedicine include the cost of telecommunication and data management equipment and of technical training for medical personnel who will employ it. Virtual medical treatment also entails potentially decreased human interaction between medical professionals and patients, an increased risk of error when medical services are delivered in the absence of a registered professional, and an increased risk that protected health information may be compromised through electronic storage and transmission.[178] There is also a concern that telemedicine may actually decrease time efficiency due to the difficulties of assessing and treating patients through virtual interactions; for example, it has been estimated that a teledermatology consultation can take up to thirty minutes, whereas fifteen minutes is typical for a traditional consultation.[179] Additionally, potentially poor quality of transmitted records, such as images or patient progress reports, and decreased access to relevant clinical information are quality assurance risks that can compromise the quality and continuity of patient care for the reporting doctor.[180] Other obstacles to the implementation of telemedicine include unclear legal regulation for some telemedical practices and difficulty claiming reimbursement from insurers or government programs in some fields.[38] Some medical organizations have delivered position statement on the correct use of telemedicine in their field.[181][182][183][184]
Another disadvantage of telemedicine is the inability to start treatment immediately. For example, a patient with a bacterial infection might be given an antibiotic hypodermic injection in the clinic, and observed for any reaction, before that antibiotic is prescribed in pill form.
We must also be wary of equitability. Many families and individuals in the United States, and other countries, do not have internet access in their homes. Not to mention they may lack the necessary equipment to access telehealth services, such as a laptop, tablet, or smart phone.
Ethical issues
Informed consent is another issue – should the patient give informed consent to receive online care before it starts? Or will it be implied if it is care that can only practically be given over distance? When telehealth includes the possibility for technical problems such as transmission errors, security breaches, or storage issues, it can impact the system's ability to communicate. It may be wise to obtain informed consent in person first, as well as having backup options for when technical issues occur. In person, a patient can see who is involved in their care (namely themselves and their clinician in a consult), but online there will be other involved such as the technology providers, therefore consent may need to involve disclosure of anyone involved in the transmission of the information and the security that will keep their information private, and any legal malpractice cases may need to involve all of those involved as opposed to what would usually just be the practitioner.[127][173][174]
The state of the market
The rate of adoption of telehealth services in any jurisdiction is frequently influenced by factors such as the adequacy and cost of existing conventional health services in meeting patient needs; the policies of governments and/or insurers with respect to coverage and payment for telehealth services; and medical licensing requirements that may inhibit or deter the provision of telehealth second opinions or primary consultations by physicians.
Projections for the growth of the telehealth market are optimistic, and much of this optimism is predicated upon the increasing demand for remote medical care. According to a recent survey, nearly three-quarters of U.S. consumers say they would use telehealth.[185] At present, several major companies along with a bevvy of startups are working to develop a leading presence in the field.
In the UK, the Government's Care Services minister, Paul Burstow, has stated that telehealth and telecare would be extended over the next five years (2012–2017) to reach three million people.
United States
In the United States, telemedicine companies are collaborating with health insurers and other telemedicine providers to expand marketshare and patient access to telemedicine consultations.
As of 2019, 95% of employers believe their organizations will continue to provide health care benefits over the next five years.[186]
The COVID-19 pandemic drove increased usage of telehealth services in the U.S. The U.S. Centers for Disease Control and Prevention reported a 154% increase in telehealth visits during the last week of March 2020, compared to the same dates in 2019.[187]
Switzerland
From 1999 to 2018, the University Hospital of Zurich (USZ) offered clinical telemedicine and online medical advice on the Internet. A team of doctors answered around 2500 anonymous inquiries annually, usually within 24 to 48 hours. The team consisted of up to six physicians who are specialists in clinical telemedicine at the USZ and have many years of experience, particularly in internal and general medicine. In the entire period, 59360 inquiries were sent and answered.[188] The majority of the users were female and on average 38 years old. However, in the course of time, considerably more men and older people began to use the service. The diversity of medical queries covered all categories of the International Statistical Classification of Diseases and Related Health Problems (ICD) and correlated with the statistical frequency of diseases in hospitals in Switzerland. Most of the inquiries concerned unclassified symptoms and signs, services related to reproduction, respiratory diseases, skin diseases, health services, diseases of the eye and nervous systems, injuries and disorders of the female genital tract. As with the Swedish online medical advice service,[189] one-sixth of the requests related to often shameful and stigmatised diseases of the genitals, gastrointestinal tract, sexually transmitted diseases, obesity and mental disorders. By providing an anonymous space where users can talk about (shameful) diseases, online telemedical services empower patients and their health literacy is enhanced by providing individualized health information. The Clinical Telemedicine and Online Counselling service of the University Hospital of Zurich is currently being revised and will be offered in a new form in the future.[190]
Developing countries
For developing countries, telemedicine and eHealth can be the only means of healthcare provision in remote areas. For example, the difficult financial situation in many African states and lack of trained health professionals has meant that the majority of the people in sub-Saharan Africa are badly disadvantaged in medical care, and in remote areas with low population density, direct healthcare provision is often very poor[191] However, provision of telemedicine and eHealth from urban centers or from other countries is hampered by the lack of communications infrastructure, with no landline phone or broadband internet connection, little or no mobile connectivity, and often not even a reliable electricity supply.[192]
Telemedicine in India
India has broad rural-urban population and rural India is bereaved from medical facilities, giving telemedicine a space for growth in India. Deprived education and medical professionals in rural areas is the reason behind government's ideology to use technology to bridge this gap. Remote areas not only present a number of challenges for the service providers but also for the families who are accessing these services. Since 2018, telemedicine has expanded in India. It has undertaken a new way for doctor consultations. On 25 March 2020, in the wake of COVID-19 pandemic, the Ministry of Health and Family Welfare issued India's Telemedicine Practice Guidelines.[193] The Board of Governors entasked by the Health Ministry published an amendment to the Indian Medical Council (Professional Conduct, Etiquette and Ethics) Regulations, 2002 that gave much-needed statutory support for the practice of telemedicine in India. This sector is at an ever-growing stage with high scope of development.[194] In April 2020, the union health ministry launched the eSanjeevani telemedicine service that operates at two levels: the doctor-to-doctor telemedicine platform, and the doctor-to-patient platform. This service crossed five million tele-consultations within a year of its launch indicating conducive environment for acceptability and growth of telemedicine in India.[195]
Telemedicine in Sub-Saharan Africa
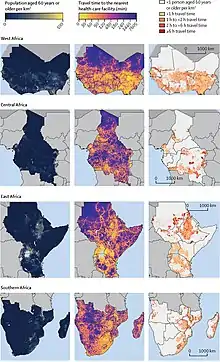
Sub-Saharan Africa is marked by the massive introduction of new technologies and internet access.[196] Urban areas are facing a rapid change and development, and access to internet and health is rapidly improving. Population in remote areas however, still lack access to healthcare and modern technologies. Some people in rural regions must travel more between 2 and 6 hours to reach the closest healthcare facilities of their country.[197] leaving room for telehealth to grow and reach isolated people in the near future.
Internet via satellite in rural areas
The Satellite African eHEalth vaLidation (SAHEL) demonstration project has shown how satellite broadband technology can be used to establish telemedicine in such areas. SAHEL was started in 2010 in Kenya and Senegal, providing self-contained, solar-powered internet terminals to rural villages for use by community nurses for collaboration with distant health centers for training, diagnosis and advice on local health issues.[198] Those methods can have major impact on both health professionals to get and provide training from remote areas, and on the local population who can receive care without traveling long distances. Some non-profits such as the Christian organization Mission Aviation Fellowship (MAF) provide internet to rural places around the world using a mobile VSAT terminal. This VSAT terminal equips remote regions allowing them to alert the world when there is a medical emergency, resulting in a rapid deployment or response from developed countries.[199] Technologies such as the ones used by MAF allows health professionals in remote clinics to have internet access, making consultations much easier, both for patients and doctors.
In 2014, the government of Luxembourg, along with satellite operator, SES and NGOs, Archemed, Fondation Follereau, Friendship Luxembourg, German Doctors and Médecins Sans Frontières, established SATMED, a multilayer eHealth platform to improve public health in remote areas of emerging and developing countries, using the Emergency.lu disaster relief satellite platform and the Astra 2G TV satellite.[200] SATMED was first deployed in response to a report in 2014 by German Doctors of poor communications in Sierra Leone hampering the fight against Ebola, and SATMED equipment arrived in the Serabu clinic in Sierra Leone in December 2014.[201][202] In June 2015 SATMED was deployed at Maternité Hospital in Ahozonnoude, Benin to provide remote consultation and monitoring, and is the only effective communication link between Ahozonnoude, the capital and a third hospital in Allada, since land routes are often inaccessible due to flooding during the rainy season.[203][204]
History
The development and history of telehealth or telemedicine (terms used interchangeably in literature) is deeply rooted in the history and development in not only technology but also society itself. Humans have long sought to relay important messages through torches, optical telegraphy, electroscopes, and wireless transmission. Early forms of telemedicine achieved with telephone and radio have been supplemented with videotelephony, advanced diagnostic methods supported by distributed client/server applications, and additionally with telemedical devices to support in-home care.[13]
In the 21st century, with the advent of the internet, portable devices and other such digital devices are taking a transformative role in healthcare and its delivery.[205]
Earliest instances
Although, traditional medicine relies on in-person care, the need and want for remote care has existed from the Roman and pre-Hippocratic periods in antiquity. The elderly and infirm who could not visit temples for medical care sent representatives to convey information on symptoms and bring home a diagnosis as well as treatment.[205] In Africa, villagers would use smoke signals to warn neighboring villages of disease outbreak.[206] The beginnings of telehealth have existed through primitive forms of communication and technology.[205] The exact date of origin for Telehealth is unknown, but it was known to have been used during the Bubonic Plague. That version of telehealth was far different from how we know it today. During that time, they were communicating by heliograph and bonfire. Those were used to notify other groups of people about famine and war.[207] Those are not using any form of technology yet but are starting to spread the idea of connectivity among groups of people who geographically could not be together.
1800s to early 1900s
As technology developed and wired communication became increasingly commonplace, the ideas surrounding telehealth began emerging. The earliest telehealth encounter can be traced to Alexander Graham Bell in 1876, when he used his early telephone as a means of getting help from his assistant Mr. Watson after he spilt acid on his trousers. Another instance of early telehealth, specifically telemedicine was reported in The Lancet in 1879. An anonymous writer described a case where a doctor successfully diagnosed a child over the telephone in the middle of the night.[205] This Lancet issue, also further discussed the potential of Remote Patient Care in order to avoid unnecessary house visits, which were part of routine health care during the 1800s.[205][208] Other instances of telehealth during this period came from the American Civil War, during which telegraphs were used to deliver mortality lists and medical care to soldiers.[208] As the 1900s started, physicians quickly found a use for the telephone making it a prime communication channel to contact patients and other physicians.[207] Over the next fifty-plus years, the telephone was a staple for medical communication. As the 1930s came around, radio communication played a key role, especially during World War I. It was specifically used to communicate with remote areas such as Alaska and Australia.[207] They used the radio to communicate medical information. During the Vietnam War, radio communication had become more advanced and was now used to send medical teams in helicopters to help. This then brought together the Aerial Medical Service (AMS) who used telegraphs, radios, and planes to help care for people who lived in remote areas.
From the late 1800s to the early 1900s the early foundations of wireless communication were laid down.[205] Radios provided an easier and near instantaneous form of communication. The use of radio to deliver healthcare became accepted for remote areas.[205][115] The Royal Flying Doctor Service of Australia is an example of the early adoption of radios in telehealth.[206]
In 1925 the inventor Hugo Gernsback wrote an article for the magazine Science and Invention which included a prediction of a future where patients could be treated remotely by doctors through a device he called a "teledactyl". His descriptions of the device are similar to what would later become possible with new technology.[209]
Mid-1900s to 1980s
When the American National Aeronautics and Space Administration (NASA) began plans to send astronauts into space, the need for telemedicine became clear. In order to monitor their astronauts in space, telemedicine capabilities were built into the spacecraft as well as the first spacesuits.[205][115] Additionally, during this period, telehealth and telemedicine were promoted in different countries especially the United States and Canada.[205] Carrier Sekani Family Services helped pioneer telehealth in British Columbia and Canada, according to its CEO Warner Adam.[210] After the telegraph and telephone started to successfully help physicians treat patients from remote areas, telehealth became more recognized. Technological advancements occurred when NASA sent men to space. Engineers for NASA created biomedical telemetry and telecommunications systems.[207] NASA technology monitored vitals such as blood pressure, heart rate, respiration rate, and temperature. After the technology was created, it then became the base of telehealth medicine for the public.
Massachusetts General Hospital and Boston's Logan International Airport had a role in the early use of telemedicine, which more or less coincided with NASA's foray into telemedicine through the use of physiologic monitors for astronauts.[211] On October 26, 1960, a plane struck a flock of birds upon takeoff, killing many passengers and leaving a number wounded. Due to the extreme complexity of trying to get all the medical personnel out from the hospital, the practical solution became telehealth.[212] This was expanded upon in 1967, when Kenneth Bird at Massachusetts General founded one of the first telemedicine clinics. The clinic addressed the fundamental problem of delivering occupational and emergency health services to employees and travellers at the airport, located three congested miles from the hospital. Clinicians at the hospital would provide consultation services to patients who were at the airport. Consultations were achieved through microwave audio as well as video links.[205][213] The airport began seeing over a hundred patients a day at its nurse-run clinic that cared for victims of plane crashes and other accidents, taking vital signs, electrocardiograms, and video images that were sent to Massachusetts General.[214] Over 1,000 patients are documented as having received remote treatment from doctors at MGH using the clinic's two-way audiovisual microwave circuit.[215] One notable story featured a woman who got off a flight in Boston and was experiencing chest pain. They performed a workup at the airport, took her to the telehealth suite where Raymond Murphy appeared on the television, and had a conversation with her. While this was happening, another doctor took notes and the nurses took vitals and any test that Murphy ordered.[212] At this point, telehealth was becoming more mainstream and was starting to become more technologically advanced, which created a viable option for patients.
In 1964, the Nebraska Psychiatric Institute began using television links to form two-way communication with the Norfolk State Hospital which was 112 miles away for the education and consultation purposes between clinicians in the two locations.[213]
In 1972 the Department of Health, Education and Welfare in the United States approved funding for seven telemedicine projects across different states. This funding was renewed and two further projects were funded the following year.[205][213]
In March 1972, the San Bernardino County Medical Society officially implemented its Tel-Med program, a system of prerecorded health-related messages, with a log of 50 tapes.[216][217] The nonprofit initiative began in 1971 as a local medical project to ease the doctor shortage in the expanding San Bernardino Valley and improve the public's access to sound medical information.[217][216] It covered subjects ranging from cannabis to vaginitis.[216] In January 1973, in response to the developing "London flu" epidemic hitting California and the country, a tape providing information on the disease was on air within a week after news broke of the flu spreading in the state.[218] That spring, programs were implemented in San Diego and Indianapolis, Indiana, signaling a national acceptance of the concept.[217] By 1979, its system offered messages on over 300 different subjects, 200 of which were available in Spanish as well as English, and serviced over 65 million people in 180 cities around the country.[216]
1980s to 1990s – maturation and renaissance
Telehealth projects underway before and during the 1980s would take off but fail to enter mainstream healthcare.[206][115] As a result, this period of telehealth history is called the "maturation" stage and made way for sustainable growth.[205] Although state funding in North America was beginning to run low, different hospitals began to launch their own telehealth initiatives.[205] NASA provided an ATS-3 satellite to enable medical care communications of American Red Cross and Pan American Health Organization response teams, following the 1985 Mexico City earthquake. The agency then launched its SateLife/HealthNet programme to increase health service connectivity in developing countries. In 1997, NASA sponsored Yale's Medical Informatics and Technology Applications Consortium project.[115][219]
Florida first experimented with "primitive" telehealth in its prisons during the latter 1980s.[220] Working with Doctors Oscar W. Boultinghouse and Michael J. Davis, from the early 1990s to 2007; Glenn G. Hammack led the University of Texas Medical Branch (UTMB) development of a pioneering telehealth program in Texas state prisons. The three UTMB alumni would, in 2007, co-found telehealth provider NuPhysician.[221]
The first interactive telemedicine system, operating over standard telephone lines, designed to remotely diagnose and treat patients requiring cardiac resuscitation (defibrillation) was developed and launched by an American company, MedPhone Corporation, in 1989. A year later under the leadership of its President/CEO S Eric Wachtel, MedPhone introduced a mobile cellular version, the MDPhone. Twelve hospitals in the U.S. served as receiving and treatment centers.[222]
At-home virtual care
As the expansion of telehealth continued in 1990 Maritime Health Services (MHS) was a big part of the initiation for occupational health services. They sent a medical officer aboard the Pacific trawler that allowed for round-the-clock communication with a physician. The system that allows for this is called the Medical Consultation Network (MedNet). MedNet is a video chatting system that has live audio and visual so the physician on the other end of the call can see and hear what is happening. MetNet can be used from anywhere, not just aboard ships.[207] Being able to provide onsite visual information allows remote patients expert emergency help and medical attention that saves money as well as lives. This has created a demand for at-home monitoring. At-home care has also become a large part of telehealth. Doctors or nurses will now give pre-op and post-op phone calls to check-in. There are also companies such as Lifeline, which give the elderly a button to press in case of an emergency. That button will automatically call for emergency help. If someone has surgery and then is sent home, telehealth allows physicians to see how the patient is progressing without them having to stay in the hospital. TeleDiagnostic Systems of San Francisco is a company that has created a device that monitors sleep patterns, so people with sleep disorders do not have to stay the night at the hospital.[207] Another at-home device that was created was the Wanderer, which was attached to Alzheimer's patients or people who had dementia. It was attached to them so when they wandered off it notified the staff to allow them to go after them. All these devices allowed healthcare beyond hospitals to improve, which means that more people are being helped efficiently.
2000s to present
The advent of high-speed Internet, and the increasing adoption of ICT in traditional methods of care, spurred advances in telehealth delivery.[12] Increased access to portable devices, like laptops and mobile phones, made telehealth more plausible; the industry then expanded into health promotion, prevention and education.[1][3][115]
In 2002, Dr. G. Byron Brooks, a former NASA surgeon and engineer who had also helped manage the UTMB Telemedicine program, co-founded Teladoc in Dallas, Texas, which was then launched in 2005 as the first national telehealth provider.[223]
In the 2010s, integration of smart home telehealth technologies, such as health and wellness devices, software, and integrated IoT, has accelerated the industry. Healthcare organizations are increasingly adopting the use of self-tracking and cloud-based technologies, and innovative data analytic approaches to accelerate telehealth delivery.[224]
In 2015, Mercy Health system opened Mercy Virtual, in Chesterfield, Missouri, the world's first medical facility dedicated solely to telemedicine.[225]
COVID-19
Telehealth expanded significantly during the COVID-19 pandemic, becoming a vital means of medical communication. It allows doctors to return to humanizing the patient.[226] It forces them to listen to what people have to say and from there make a diagnosis. Studies have demonstrated high trust in telehealth expressed by patients during the COVID-19 pandemic.[227] Some researchers claim this creates an environment that encourages greater vulnerability among patients in self disclosure in the practice of narrative medicine.[226] Telehealth allows for Zoom calls and video chats from across the world checking in on patients and speaking to physicians. Universities are now ensuring that medical students graduate with proficient telehealth communication skills.[228] Experts suggest that telehealth has become a vital part of medical care; with more virtual options becoming available. The pandemic era also identified the "potential to significantly improve global health equity" through telehealth and other virtual care technologies.[229]
See also
- Artificial intelligence in healthcare
- American Telemedicine Association
- American Well
- Center for Telehealth and E-Health Law
- Connected health
- eHealth
- In absentia health care
- Mercy Virtual
- mHealth
- Myca
- National Rural Health Association
- Data sharing between doctors through mixed reality headsets
- Remote therapy
- Ronald S. Weinstein
- Smart city
- Tele-epidemiology
- Teladoc
- Telecare
- Telemedicine service providers
- Telemental health
- Teleneuropsychology
- Telenursing
- Telepathology
- Telepsychology
- UNESCO Chair in Telemedicine
References
- "TeleHealth". The Health Resources and Services Administration. 2017-04-28.
- Shaw DK (June 2009). "Overview of telehealth and its application to cardiopulmonary physical therapy". Cardiopulmonary Physical Therapy Journal. 20 (2): 13–8. doi:10.1097/01823246-200920020-00003. PMC 2845264. PMID 20467533.
- Masson M (December 2014). "Benefits of TED Talks". Canadian Family Physician. 60 (12): 1080. PMC 4264800. PMID 25500595.
- Mashima PA, Doarn CR (December 2008). "Overview of telehealth activities in speech-language pathology". Telemedicine Journal and e-Health. 14 (10): 1101–17. doi:10.1089/tmj.2008.0080. PMID 19119834.
- Miller EA (July 2007). "Solving the disjuncture between research and practice: telehealth trends in the 21st century". Health Policy. 82 (2): 133–41. doi:10.1016/j.healthpol.2006.09.011. PMID 17046097.
- Mitchell B (2015-07-01). "Teladoc shares surge 50% in healthy IPO debut". USA Today. Retrieved 2015-07-02.
- "2010 Opportunities and developments | Report on the second global survey on eHealth | Global Observatory for eHealth series - Volume 2: TELEMEDICINE" (PDF). 13 January 2011. Retrieved 25 March 2016.
- "What is Telemedicine?". Washington, D.C.: American Telemedicine Association. Archived from the original on 8 May 2013. Retrieved 21 August 2011.
- Alexandrov AW, Alexandrov AV (April 2020). "Innovations in Prehospital Stroke Management Utilizing Mobile Stroke Units". Continuum. Minneapolis, Minn. 26 (2): 506–512. doi:10.1212/CON.0000000000000850. PMID 32224764. S2CID 214732273.
- Itrat A, Taqui A, Cerejo R, Briggs F, Cho SM, Organek N, Reimer AP, Winners S, Rasmussen P, Hussain MS, Uchino K (February 2016). "Telemedicine in Prehospital Stroke Evaluation and Thrombolysis: Taking Stroke Treatment to the Doorstep". JAMA Neurology. 73 (2): 162–8. doi:10.1001/jamaneurol.2015.3849. PMID 26641366.
- Audebert H, Fassbender K, Hussain MS, Ebinger M, Turc G, Uchino K, Davis S, Alexandrov A, Grotta J, et al. (PRESTO Group) (December 2017). "The PRE-hospital Stroke Treatment Organization". International Journal of Stroke. 12 (9): 932–940. doi:10.1177/1747493017729268. PMID 28872449.
- "What is Telehealth?". The Center for Connected Health Policy. Archived from the original on January 15, 2012.
- Sachpazidis I (10 Jul 2008). Image and Medical Data Communication Protocols for Telemedicine and Teleradiology (dissertation) (PDF) (Thesis). Darmstadt, Germany: Department of Computer Science, Technical University of Darmstadt. Retrieved 14 Aug 2018.
- Salehahmadi Z, Hajialiasghari F (January 2013). "Telemedicine in iran: chances and challenges". World Journal of Plastic Surgery. 2 (1): 18–25. PMC 4238336. PMID 25489500.
- Pierratos A (November 1999). "Nocturnal hemodialysis: dialysis for the new millennium". Canadian Medical Association Journal. 161 (9): 1137. PMC 1230743. PMID 10569098.
- Koutras C, Bitsaki M, Koutras G, Nikolaou C, Heep H (17 August 2015). "Socioeconomic impact of e-Health services in major joint replacement: A scoping review". Technology and Health Care. 23 (6): 809–17. doi:10.3233/THC-151036. PMID 26409523.
- Fatehi F, Armfield NR, Dimitrijevic M, Gray LC (October 2014). "Clinical applications of videoconferencing: a scoping review of the literature for the period 2002-2012". Journal of Telemedicine and Telecare. 20 (7): 377–83. doi:10.1177/1357633X14552385. PMID 25399998. S2CID 39080490.
- McGraw-Hill Concise Encyclopedia of Engineering. Videotelephony, McGraw-Hill, 2002. Retrieved from the FreeDictionary.com website, January 9, 2010
- George R. Schwartz, C. Gene Cayten; George R. Schwartz (editor). Principles and Practice of Emergency Medicine, Volume 2, Lea & Febiger, 1992, pg.3202, ISBN 0-8121-1373-X, ISBN 978-0-8121-1373-0.
- Rogove HJ, McArthur D, Demaerschalk BM, Vespa PM (January–February 2012). "Barriers to telemedicine: survey of current users in acute care units". Telemedicine Journal and e-Health. 18 (1): 48–53. doi:10.1089/tmj.2011.0071. PMID 22082107.
- Langabeer JR, Champagne-Langabeer T, Alqusairi D, Kim J, Jackson A, Persse D, Gonzalez M (September 2017). "Cost-benefit analysis of telehealth in pre-hospital care". Journal of Telemedicine and Telecare. 23 (8): 747–751. doi:10.1177/1357633X16680541. PMID 27913657. S2CID 26707384.
- "Nurses Happier Using Telecare, Says International Survey". eHealth Insider. 15 June 2005. Archived from the original on 18 June 2006. Retrieved 4 April 2009.
- "Google Glass connects breastfeeding moms with lactation help". Inquisitr. 24 April 2014. Retrieved 12 June 2014.
- Social, Small World (25 February 2014). "Breastfeeding Walkthrough for Mothers and Counselors" – via Vimeo.
- "Exclusive Clips Google glasses help breastfeeding mums". Jumpin Today Show. Mi9 Pty. Ltd. Retrieved 12 June 2014.
- "Breastfeeding mothers get help from Google Glass and Small World". The Sydney Morning Herald.
- "Turns Out Google Glass Is Good for Breastfeeding". Motherboard Vice Media Inc. 21 April 2014. Retrieved 1 May 2014.
- "SWS Website - We transfer complex and tacit knowledge". SWS Website.
- "Breastfeeding Support Project - Small World Social". 23 April 2014. Archived from the original on 2014-04-23.
- Finucane, Anne M.; O'Donnell, Hannah; Lugton, Jean; Gibson-Watt, Tilly; Swenson, Connie; Pagliari, Claudia (2021-04-06). "Digital health interventions in palliative care: a systematic meta-review". npj Digital Medicine. 4 (1): 64. doi:10.1038/s41746-021-00430-7. ISSN 2398-6352. PMC 8024379. PMID 33824407.
- Chen, Yiping; Qiao, Caihong; Zhang, Xianhui; Li, Wei; Yang, Hui (2022-09-14). "The Effect of Tele-palliative Care on Patient and Caregiver Outcomes: A Systematic Review". American Journal of Hospice and Palliative Medicine. 40 (8): 907–925. doi:10.1177/10499091221123566. ISSN 1049-9091. PMID 36113129. S2CID 252287978.
- Lundereng, Elias David; Nes, Andréa Aparecida Gonçalves; Holmen, Heidi; Winger, Anette; Thygesen, Hilde; Jøranson, Nina; Borge, Christine Råheim; Dajani, Olav; Mariussen, Kari L.; Steindal, Simen A. (2023-03-29). "Health Care Professionals' Experiences and Perspectives on Using Telehealth for Home-based Palliative Care: Scoping Review". Journal of Medical Internet Research. 25 (1): e43429. doi:10.2196/43429. PMC 10131609. PMID 36989024.
- Steindal, Simen A.; Nes, Andréa Aparecida Goncalves; Godskesen, Tove E.; Dihle, Alfhild; Lind, Susanne; Winger, Anette; Klarare, Anna (2020-05-05). "Patients' Experiences of Telehealth in Palliative Home Care: Scoping Review". Journal of Medical Internet Research. 22 (5): e16218. doi:10.2196/16218. PMC 7238080. PMID 32369037.
- Steindal, Simen A.; Nes, Andréa Aparecida Gonçalves; Godskesen, Tove E.; Holmen, Heidi; Winger, Anette; Österlind, Jane; Dihle, Alfhild; Klarare, Anna (2023-03-13). "Advantages and Challenges of Using Telehealth for Home-Based Palliative Care: Systematic Mixed Studies Review". Journal of Medical Internet Research. 25 (1): e43684. doi:10.2196/43684. PMC 10131904. PMID 36912876.
- "What Are Palliative Care and Hospice Care?". National Institute on Aging. Retrieved 2023-04-27.
- Head, Barbara A.; Schapmire, Tara J.; Zheng, Yongqiang (April 2017). "Telehealth in Palliative Care: A Systematic Review of Patient-Reported Outcomes". Journal of Hospice & Palliative Nursing. 19 (2): 130. doi:10.1097/NJH.0000000000000319. ISSN 1522-2179. S2CID 78763088.
- Lowry SJ, Kay CN, Marsom EN, Park JS, Poole S, Page AT (2020). "Optimising health outcomes via pharmacist delivered telehealth medicines management: a systematic review". Journal of Pharmacy Practice and Research. Wiley. 50 (5): 377–390. doi:10.1002/jppr.1695. ISSN 1445-937X. S2CID 225070505.
- Angaran DM (July 1999). "Telemedicine and telepharmacy: current status and future implications". American Journal of Health-System Pharmacy. 56 (14): 1405–26. doi:10.1093/ajhp/56.14.1405. PMID 10428449.
- "What is Telepsychiatry?". American Psychiatric Association. Retrieved 2023-02-20.
- "What is Telemental Health?". National Institute of Mental Health (NIMH). Retrieved 2023-02-20.
- Schlief, Merle; Saunders, Katherine R K; Appleton, Rebecca; Barnett, Phoebe; Vera San Juan, Norha; Foye, Una; Olive, Rachel Rowan; Machin, Karen; Shah, Prisha; Chipp, Beverley; Lyons, Natasha; Tamworth, Camilla; Persaud, Karen; Badhan, Monika; Black, Carrie-Ann (2022-09-29). "Synthesis of the Evidence on What Works for Whom in Telemental Health: Rapid Realist Review". Interactive Journal of Medical Research. 11 (2): e38239. doi:10.2196/38239. ISSN 1929-073X. PMC 9524537. PMID 35767691.
- Appleton, Rebecca; Williams, Julie; Vera San Juan, Norha; Needle, Justin J; Schlief, Merle; Jordan, Harriet; Sheridan Rains, Luke; Goulding, Lucy; Badhan, Monika; Roxburgh, Emily; Barnett, Phoebe; Spyridonidis, Spyros; Tomaskova, Magdalena; Mo, Jiping; Harju-Seppänen, Jasmine (2021-12-09). "Implementation, Adoption, and Perceptions of Telemental Health During the COVID-19 Pandemic: Systematic Review". Journal of Medical Internet Research. 23 (12): e31746. doi:10.2196/31746. ISSN 1438-8871. PMC 8664153. PMID 34709179.
- Dorsey ER, Glidden AM, Holloway MR, Birbeck GL, Schwamm LH (May 2018). "Teleneurology and mobile technologies: the future of neurological care". Nature Reviews. Neurology. 14 (5): 285–297. doi:10.1038/nrneurol.2018.31. PMID 29623949. S2CID 4620042.
- Beck CA, Beran DB, Biglan KM, Boyd CM, Dorsey ER, Schmidt PN, et al. (September 2017). "National randomized controlled trial of virtual house calls for Parkinson disease". Neurology. 89 (11): 1152–1161. doi:10.1212/WNL.0000000000004357. PMC 5595275. PMID 28814455.
- Ben-Pazi H, Browne P, Chan P, Cubo E, Guttman M, Hassan A, et al. (April 2018). "The Promise of Telemedicine for Movement Disorders: an Interdisciplinary Approach". Current Neurology and Neuroscience Reports. 18 (5): 26. doi:10.1007/s11910-018-0834-6. PMID 29654523. S2CID 4850577.
- Beck CA, Beran DB, Biglan KM, Boyd CM, Dorsey ER, Schmidt PN, et al. (September 2017). "National randomized controlled trial of virtual house calls for Parkinson disease". Neurology. 89 (11): 1152–1161. doi:10.1212/WNL.0000000000004357. PMC 5595275. PMID 28814455.
- Appelboom G, Yang AH, Christophe BR, Bruce EM, Slomian J, Bruyère O, et al. (July 2014). "The promise of wearable activity sensors to define patient recovery". Journal of Clinical Neuroscience. 21 (7): 1089–1093. doi:10.1016/j.jocn.2013.12.003. PMID 24534628. S2CID 2543446.
- Lazarus G, Permana AP, Nugroho SW, Audrey J, Wijaya DN, Widyahening IS (October 2020). "Telestroke strategies to enhance acute stroke management in rural settings: A systematic review and meta-analysis". Brain and Behavior. 10 (10): e01787. doi:10.1002/brb3.1787. PMC 7559631. PMID 32812380.
- Chalouhi N, Dressler JA, Kunkel ES, Dalyai R, Jabbour P, Gonzalez LF, et al. (October 2013). "Intravenous tissue plasminogen activator administration in community hospitals facilitated by telestroke service". Neurosurgery. 73 (4): 667–71, discussion 671–2. doi:10.1227/NEU.0000000000000073. PMID 23842556.
- Mouchtouris N, Yu S, Prashant G, Nelson N, Reyes M, Gonzalez G, et al. (July 2022). "Telemedicine in Neurosurgery During the COVID-19 Outbreak: Where We Are 1 Year Later". World Neurosurgery. 163: e83–e88. doi:10.1016/j.wneu.2022.03.037. PMC 8925084. PMID 35306198.
- Mouchtouris N, Lavergne P, Montenegro TS, Gonzalez G, Baldassari M, Sharan A, et al. (August 2020). "Telemedicine in Neurosurgery: Lessons Learned and Transformation of Care During the COVID-19 Pandemic". World Neurosurgery. 140: e387–e394. doi:10.1016/j.wneu.2020.05.251. PMC 7274123. PMID 32512241.
- Wadsworth HE, Dhima K, Womack KB, Hart J, Weiner MF, Hynan LS, Cullum CM (December 2018). "Validity of Teleneuropsychological Assessment in Older Patients with Cognitive Disorders". Archives of Clinical Neuropsychology. 33 (8): 1040–1045. doi:10.1093/arclin/acx140. PMC 6887729. PMID 29329363.
- Wadsworth HE, Galusha-Glasscock JM, Womack KB, Quiceno M, Weiner MF, Hynan LS, et al. (August 2016). "Remote Neuropsychological Assessment in Rural American Indians with and without Cognitive Impairment". Archives of Clinical Neuropsychology. 31 (5): 420–425. doi:10.1093/arclin/acw030. PMC 4954610. PMID 27246957.
- Galusha-Glasscock JM, Horton DK, Weiner MF, Cullum CM (February 2016). "Video Teleconference Administration of the Repeatable Battery for the Assessment of Neuropsychological Status". Archives of Clinical Neuropsychology. 31 (1): 8–11. doi:10.1093/arclin/acv058. PMC 4718188. PMID 26446834.
- Parikh M, Grosch MC, Graham LL, Hynan LS, Weiner M, Shore JH, Cullum CM (2013). "Consumer acceptability of brief videoconference-based neuropsychological assessment in older individuals with and without cognitive impairment". The Clinical Neuropsychologist. 27 (5): 808–817. doi:10.1080/13854046.2013.791723. PMC 3692573. PMID 23607729.
- Grosch MC, Gottlieb MC, Cullum CM (October 2011). "Initial practice recommendations for teleneuropsychology". The Clinical Neuropsychologist. 25 (7): 1119–1133. doi:10.1080/13854046.2011.609840. PMID 21951075. S2CID 29638722.
- Munro Cullum C, Hynan LS, Grosch M, Parikh M, Weiner MF (November 2014). "Teleneuropsychology: evidence for video teleconference-based neuropsychological assessment". Journal of the International Neuropsychological Society. 20 (10): 1028–1033. doi:10.1017/S1355617714000873. PMC 4410096. PMID 25343269.
- Costantino A, Roncoroni L, Noviello D, Nandi N, Lombardo V, Scricciolo A, Scaramella L, Vecchi M, Elli L. Nutritional and Gastroenterological Monitoring of Patients With Celiac Disease During COVID-19 Pandemic: The Emerging Role of Telemedicine and Point-of-Care Gluten Detection Tests. Front Nutr. 2021 Apr 13;8:622514. https://doi.org/10.3389/fnut.2021.622514
- E-health care information systems: an introduction for students and professionals. John Wiley and Sons. 2005. p. 219. ISBN 978-0-7879-6618-8.
- Keaton L, Pierce LL, Steiner V, Lance K (October 2004). "An E-rehabilitation Team Helps Caregivers Deal with Stroke". The Internet Journal of Allied Health Sciences and Practice. Ijahsp.nova.edu. 2 (4). ISSN 1540-580X. Retrieved 26 March 2011.
- "OSERS". www.ed.gov. Archived from the original on 2003-10-11.
- Hiers M. "Everything You Need to Know About Telemedicine". Retrieved 10 July 2014.
- Palsbo SE (July 2004). "Medicaid payment for telerehabilitation". Archives of Physical Medicine and Rehabilitation. 85 (7): 1188–1191. doi:10.1016/j.apmr.2003.09.008. PMID 15241772.
- Collins H (28 August 2008). "Advanced First Responder and Medical Capabilities Could Save Lives". Emergency Management. Archived from the original on 18 August 2016. Retrieved 23 June 2019.
- "Advanced technologies and wireless telecommunications enhance care and medical training at the Ryder Trauma Center in Miami". Virtual Medical Worlds. 4 December 2008. Retrieved 23 July 2013.
- "EMS Trauma Grand Rounds". Utah Telehealth Network. Archived from the original on 16 September 2009. Retrieved 23 July 2013.
- Gonzalez D (10 November 2011). "UM Doctors Use Telemedicine to Continue Care In Iraq". Retrieved 23 July 2013.
- Telecardiology.
- General health care delivery. Remotely treating ventricular fibrillation. Medphone Corporation, 1989
- Shanker A, Makhija S, Mantri PK (1982). "Teletransmission of ECG Waveform: An Ingenious Low Priced Technique". Indian Heart Journal. 34 (6).
- "Electronic Government Directorate | Pakistan telemedicine". Archived from the original on 2011-07-04. Retrieved 25 March 2016.
- Sanders D, Ungar L, Eskander MA, Seto AH (July 2019). "Ambulatory ECG monitoring in the age of smartphones". Cleveland Clinic Journal of Medicine. 86 (7): 483–493. doi:10.3949/ccjm.86a.18123. PMID 31291182. S2CID 195811584.
- Kontaxakis G, Visvikis D, Ohl R, Sachpazidis I, Suarez JP, Selby P, et al. (2006). "Integrated telemedicine applications and services for oncological positron emission tomography". Oncology Reports. 15 (4): 1091–1100. doi:10.3892/or.15.4.1091. PMID 16525707.
- Weinstein RS, Graham AR, Richter LC, Barker GP, Krupinski EA, Lopez AM, et al. (August 2009). "Overview of telepathology, virtual microscopy, and whole slide imaging: prospects for the future". Human Pathology. 40 (8): 1057–1069. doi:10.1016/j.humpath.2009.04.006. PMID 19552937.
- Kumar S (2009). "Telepathology: An Audit". In Kumar S, Dunn BE (eds.). Telepathology. Springer-Verlag Berlin Heidelberg. pp. 225–229. doi:10.1007/978-3-540-85786-0_16. ISBN 978-3-540-85785-3.
- Weinstein RS (May 1986). "Prospects for telepathology". Human Pathology. 17 (5): 433–434. doi:10.1016/s0046-8177(86)80028-4. PMID 3516858.
- Weinstein RS, Bloom KJ, Rozek LS (July 1987). "Telepathology and the networking of pathology diagnostic services". Archives of Pathology & Laboratory Medicine. 111 (7): 646–652. PMID 3606341.
- Kayser K, Szymas J, Weinstein RS (1999). Telepathology: Telecommunications, Electronic Education and Publication in Pathology. Springer, NY. pp. 1–186.
- "ReUnion '10 award winners". Union College. Archived from the original on 5 August 2012. Retrieved 25 July 2013.
- Nordrum I, Engum B, Rinde E, Finseth A, Ericsson H, Kearney M, et al. (June 1991). "Remote frozen section service: a telepathology project in northern Norway". Human Pathology. 22 (6): 514–518. doi:10.1016/0046-8177(91)90226-F. PMID 1864583.
- "Online Visits With Dermatologists Enhance Access to Care for Patients With Minor and Serious Skin Conditions, Boost Physician Productivity". Agency for Healthcare Research and Quality. 2013-11-06. Retrieved 6 November 2013.
- Ford AR, Gibbons CM, Torres J, Kornmehl HA, Singh S, Young PM, et al. (July 2019). "Access to Dermatological Care with an Innovative Online Model for Psoriasis Management: Results from a Randomized Controlled Trial". Telemedicine Journal and e-Health. 25 (7): 619–627. doi:10.1089/tmj.2018.0160. PMC 6417973. PMID 30222518.
- Wootton R, Batch J (2005). Telepediatrics: telemedicine and child health. Royal Society of Medicine. ISBN 978-1-85315-645-8.
- Wurm EM, Hofmann-Wellenhof R, Wurm R, Soyer HP (February 2008). "Telemedicine and teledermatology: Past, present and future". Journal der Deutschen Dermatologischen Gesellschaft. 6 (2): 106–112. doi:10.1111/j.1610-0387.2007.06440.x. PMID 18005076. S2CID 41450493.
- Burg G, Hasse U, Cipolat C, Kropf R, Djamei V, Soyer HP, Chimenti S (2005). "Teledermatology: just cool or a real tool?". Dermatology. 210 (2): 169–173. doi:10.1159/000082573. PMID 15724100. S2CID 36135198.
- Perednia DA, Brown NA (January 1995). "Teledermatology: one application of telemedicine". Bulletin of the Medical Library Association. 83 (1): 42–47. PMC 225996. PMID 7703938.
- "Telemedicine-Based Eye Examinations Enhance Access, Reduce Costs, and Increase Satisfaction for Low-Income and Minority Patients with Diabetes". Agency for Healthcare Research and Quality. 2013-07-17. Retrieved 24 July 2013.
- "Remote Retinal Screening Facilitates Diagnosis and Treatment of Retinopathy for Poor and/or Uninsured Patients With Diabetes in Rural California". Agency for Healthcare Research and Quality. 2012-10-03. Retrieved 24 July 2013.
- Phukan R, Mehta MR, Gogia S (2014-11-02). "Results and Problems in Executing Teleophthalmology". Indian Journal of Medical Informatics. 8 (2): 32–33.
- "Telehealth company sues Indiana for ban on online eye exams". TimesUnion.com. 21 April 2019.
- "IST's Media Collection". Interface Surgical Technologies.
- Endler M, Lavelanet A, Cleeve A, Ganatra B, Gomperts R, Gemzell-Danielsson K (August 2019). "Telemedicine for medical abortion: a systematic review". BJOG. 126 (9): 1094–1102. doi:10.1111/1471-0528.15684. PMC 7496179. PMID 30869829.
- "Study: Taking abortion pill at home as safe as in a clinic". NBC News. 17 May 2017. Retrieved 2020-05-18.
- "Improving Access to Abortion via Telehealth". Guttmacher Institute. 2019-05-07. Retrieved 2020-04-21.
- "Telabortion Project". Retrieved April 26, 2020.
- Belluck P (28 April 2020). "Abortion by Telemedicine: A Growing Option as Access to Clinics Wanes". New York Times. Retrieved May 5, 2020.
- "Home - Telabortion". telabortion.org. Retrieved 2020-05-11.
- Jones RK, Jerman J (March 2017). "Abortion Incidence and Service Availability In the United States, 2014". Perspectives on Sexual and Reproductive Health. 49 (1): 17–27. doi:10.1363/2019.30760. PMC 5487028. PMID 28094905.
- "Medication Abortion and Telemedicine: Innovations and Barriers During the COVID-19 Emergency". KFF. 2020-06-08. Retrieved 2020-08-03.
- "Coronavirus (COVID-19) infection and abortion care". Royal College of Obstetricians & Gynaecologists. Retrieved 2020-08-03.
- Arora S, Thornton K, Murata G, Deming P, Kalishman S, Dion D, et al. (June 2011). "Outcomes of treatment for hepatitis C virus infection by primary care providers". The New England Journal of Medicine. 364 (23): 2199–2207. doi:10.1056/NEJMoa1009370. PMC 3820419. PMID 21631316.
- "Healthcare Workers". 11 February 2020.
- Sezgin, Emre; Huang, Yungui; Lin, Deborah; Ramtekkar, Ujjwal; Pauline, Lindsey; Lin, Simon (2021-10-01). "Documented Reasons of Cancellation and Rescheduling of Telehealth Appointments During the Pandemic". Telemedicine and e-Health. 27 (10): 1143–1150. doi:10.1089/tmj.2020.0454. ISSN 1530-5627. PMID 33373553. S2CID 229721870.
- Louis S, Isaacson JH, Yepes-Rios M, Mehta N (April 2020). "Designing Virtual Medical Student Ambulatory Rotations in Light of the Coronavirus Pandemic: A Pilot Project". EdArXiv. doi:10.35542/osf.io/9urcd. S2CID 243221925.
- Murphy B (17 September 2020). "How Medical Students are Innovating During COVID-19". American Medical Association.
- "Information on Medication-Assisted Treatment (MAT)". SAMHSA. 21 July 2015.
- "Use of Telephone Evaluations to Initiate Buprenorphine Prescribing" (PDF). DEA Information Page.
- Jane (2020-07-21). "I am Addicted to Opioids and in my Desperation I Turned to the Internet — Here is What happened". Medium. Retrieved 2020-07-22.
- Alharthi MS (2012). Telehealth Practice in Eight Countries: New Zealand, Australia, the USA, Canada, UK, Malaysia, China and India (Masters in Information Science thesis). Massey University, Albany Campus, Auckland, New Zealand.
- García-Rojo M (2016). "International Clinical Guidelines for the Adoption of Digital Pathology: A Review of Technical Aspects". Pathobiology. 83 (2–3): 99–109. doi:10.1159/000441192. PMID 27100834.
- "Statement on telehealth" (PDF). Medical Council of New Zealand. 2013.
- Lucas J (2013). Clinicians' perceptions of telemedicine: Opportunities and barriers for emergency medicine • Health Improvement and Innovation Resource Centre (Masters (Nursing) thesis). University of Auckland. Archived from the original on 2018-12-04. Retrieved 2018-12-04.
- Possemato K, Bishop TM, Willis MA, Lantinga LJ (October 2013). "Healthcare utilization and symptom variation among veterans using Behavioral Telehealth Center services". The Journal of Behavioral Health Services & Research. 40 (4): 416–26. doi:10.1007/s11414-013-9338-y. PMID 23616251. S2CID 33937086.
- Darkins A, Foster L, Anderson C, Goldschmidt L, Selvin G (July 2013). "The design, implementation, and operational management of a comprehensive quality management program to support national telehealth networks". Telemedicine Journal and e-Health. 19 (7): 557–64. doi:10.1089/tmj.2012.0263. PMID 23705961.
- Maheu M, Whitten P, Allen A (2002-02-28). E-Health, Telehealth, and Telemedicine: A Guide to Startup and Success. John Wiley & Sons. ISBN 9780787959036.
- Alexander GC, Tajanlangit M, Heyward J, Mansour O, Qato DM, Stafford RS (October 2020). "Use and Content of Primary Care Office-Based vs Telemedicine Care Visits During the COVID-19 Pandemic in the US". JAMA Network Open. 3 (10): e2021476. doi:10.1001/jamanetworkopen.2020.21476. PMC 7532385. PMID 33006622.
- "Telemedicine is here to stay". Building Better Healthcare. 11 August 2021. Retrieved 26 September 2021.
- "Prime Minister says GPs should see patients face to face". Pulse. 21 September 2021. Retrieved 26 September 2021.
- Vockley M (2015-10-01). "The Rise of Telehealth: 'Triple Aim,' Innovative Technology, and Popular Demand Are Spearheading New Models of Health and Wellness Care". Biomedical Instrumentation & Technology. 49 (5): 306–20. doi:10.2345/0899-8205-49.5.306. PMID 26443907.
- Kvedar J, Coye MJ, Everett W (February 2014). "Connected health: a review of technologies and strategies to improve patient care with telemedicine and telehealth". Health Affairs. 33 (2): 194–9. doi:10.1377/hlthaff.2013.0992. PMID 24493760.
- Hirani SP, Rixon L, Beynon M, Cartwright M, Cleanthous S, Selva A, Sanders C, Newman SP (May 2017). "Quantifying beliefs regarding telehealth: Development of the Whole Systems Demonstrator Service User Technology Acceptability Questionnaire" (PDF). Journal of Telemedicine and Telecare. 23 (4): 460–469. doi:10.1177/1357633X16649531. PMID 27224997. S2CID 206705202.
- Cantor AG, Jungbauer RM, Totten AM, Tilden EL, Holmes R, Ahmed A, et al. (September 2022). "Telehealth Strategies for the Delivery of Maternal Health Care : A Rapid Review". Annals of Internal Medicine. 175 (9): 1285–1297. doi:10.7326/M22-0737. PMID 35878405. S2CID 251067668.
- Richard Payerchin (January 20, 2023). "Telemedicine better than expected for consulting on surgeries". Medical Economics.
- "Ryan Haight Act will Require Tighter Restrictions on Internet Pharmacies". www.govtech.com. 27 July 2010. Retrieved 7 March 2016.
- "Telemedicine sanction in Idaho clouds doctor's future". Spokesman.com. Retrieved 7 March 2016.
- "Teladoc case against Texas Medical Board will move forward, judge rules". Modern Healthcare. 14 December 2015. Retrieved 7 March 2016.
- Myers K, Turvey C, eds. (2012-09-20). Telemental Health: Clinical, Technical, and Administrative Foundations for Evidence-Based Practice (1 ed.). Elsevier. ISBN 9780124160484.
- Umefjord G (2006-01-01). Internet consultation in medicine: studies of a text-based Ask the doctor service (Ph.D. thesis). Umeå University).
- Kahn JM (April 2015). "Virtual visits--confronting the challenges of telemedicine". The New England Journal of Medicine. 372 (18): 1684–1685. doi:10.1056/NEJMp1500533. PMID 25923547.
- Goggin G (2006-01-01). Cell Phone Culture: Mobile Technology in Everyday Life. Routledge. ISBN 9780415367431.
- Bloomsbury.com. "mHealth in Practice". Bloomsbury Publishing. Retrieved 2016-06-16.
- Ben-Zeev D, Brian RM, Jonathan G, Razzano L, Pashka N, Carpenter-Song E, et al. (September 2018). "Mobile Health (mHealth) Versus Clinic-Based Group Intervention for People With Serious Mental Illness: A Randomized Controlled Trial". Psychiatric Services. 69 (9): 978–985. doi:10.1176/appi.ps.201800063. PMID 29793397.
- Hardinge M, Rutter H, Velardo C, Shah SA, Williams V, Tarassenko L, Farmer A (June 2015). "Using a mobile health application to support self-management in chronic obstructive pulmonary disease: a six-month cohort study". BMC Medical Informatics and Decision Making. 15 (1): 46. doi:10.1186/s12911-015-0171-5. PMC 4472616. PMID 26084626.
- Dall'Ora C, Griffiths P, Hope J, Briggs J, Jeremy J, Gerry S, Redfern OC (June 2021). "How long do nursing staff take to measure and record patients' vital signs observations in hospital? A time-and-motion study". International Journal of Nursing Studies. 118: 103921. doi:10.1016/j.ijnurstu.2021.103921. PMC 8249906. PMID 33812297.
- "Facts and Figures 2021: 2.9 billion people still offline". ITU Hub. 2021-11-29. Retrieved 2022-05-10.
- "Google Glass can help you breastfeed". HLN Staff. 2014.
- "Breastfeeding and Google Glass application trial". The Australian Breastfeeding Association. 2016. Archived from the original on 2019-04-10. Retrieved 2016-06-16.
- "Breastfeeding Support Program Through Google Glass". Small World. 2015.
- "WHO | Evidence on the long-term effects of breastfeeding". www.who.int. Archived from the original on January 16, 2012. Retrieved 2016-06-16.
- Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J, et al. (January 2016). "Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect". Lancet. 387 (10017): 475–490. doi:10.1016/S0140-6736(15)01024-7. PMID 26869575.
- Albritton J, Ortiz A, Wines R, Booth G, DiBello M, Brown S, et al. (February 2022). "Video Teleconferencing for Disease Prevention, Diagnosis, and Treatment : A Rapid Review". Annals of Internal Medicine. 175 (2): 256–266. doi:10.7326/m21-3511. PMID 34871056. S2CID 244923066.
- Novak M. "Telemedicine Predicted in 1925". Smithsonian Magazine. Retrieved 1 February 2022.
- Gillman-Wells CC, Sankar TK, Vadodaria S (February 2021). "COVID-19 Reducing the Risks: Telemedicine is the New Norm for Surgical Consultations and Communications". Aesthetic Plastic Surgery. 45 (1): 343–348. doi:10.1007/s00266-020-01907-8. PMC 7471549. PMID 32885319.
- Monaghesh E, Hajizadeh A (August 2020). "The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence". BMC Public Health. 20 (1): 1193. doi:10.1186/s12889-020-09301-4. PMC 7395209. PMID 32738884.
- "Telehealth Key to Maintaining Access to Addiction Recovery". www.aafp.org. Retrieved 27 January 2022.
- Portnoy J, Waller M, Elliott T (May 2020). "Telemedicine in the Era of COVID-19". The Journal of Allergy and Clinical Immunology. In Practice. 8 (5): 1489–1491. doi:10.1016/j.jaip.2020.03.008. PMC 7104202. PMID 32220575.
- "Benefits of Telemedicine". www.hopkinsmedicine.org. 18 January 2022. Retrieved 1 February 2022.
- Molfenter T, Boyle M, Holloway D, Zwick J (May 2015). "Trends in telemedicine use in addiction treatment". Addiction Science & Clinical Practice. 10 (1): 14. doi:10.1186/s13722-015-0035-4. PMC 4636787. PMID 26016484.
- Hyder MA, Razzak J (November 2020). "Telemedicine in the United States: An Introduction for Students and Residents". Journal of Medical Internet Research. 22 (11): e20839. doi:10.2196/20839. PMC 7690251. PMID 33215999.
- Bardsley M, Steventon A, Doll H (October 2013). "Impact of telehealth on general practice contacts: findings from the whole systems demonstrator cluster randomised trial". BMC Health Services Research. 13: 395. doi:10.1186/1472-6963-13-395. PMC 3852608. PMID 24099334.
- Cartwright M, Hirani SP, Rixon L, Beynon M, Doll H, Bower P, et al. (February 2013). "Effect of telehealth on quality of life and psychological outcomes over 12 months (Whole Systems Demonstrator telehealth questionnaire study): nested study of patient reported outcomes in a pragmatic, cluster randomised controlled trial". BMJ. 346: f653. doi:10.1136/bmj.f653. PMC 3582704. PMID 23444424.
- Sanders C, Rogers A, Bowen R, Bower P, Hirani S, Cartwright M, et al. (July 2012). "Exploring barriers to participation and adoption of telehealth and telecare within the Whole System Demonstrator trial: a qualitative study". BMC Health Services Research. 12: 220. doi:10.1186/1472-6963-12-220. PMC 3413558. PMID 22834978.
- Eddison N, Leone E, Healy A, Royse C, Chockalingam N (June 2022). "The potential impact of allied health professional telehealth consultations on health inequities and the burden of treatment". International Journal for Equity in Health. 21 (1): 91. doi:10.1186/s12939-022-01689-2. PMC 9245876. PMID 35773695.
- Waller M, Stotler C (August 2018). "Telemedicine: a Primer". Current Allergy and Asthma Reports. 18 (10): 54. doi:10.1007/s11882-018-0808-4. PMID 30145709. S2CID 52089750.
- Scott Kruse C, Karem P, Shifflett K, Vegi L, Ravi K, Brooks M (January 2018). "Evaluating barriers to adopting telemedicine worldwide: A systematic review". Journal of Telemedicine and Telecare. 24 (1): 4–12. doi:10.1177/1357633X16674087. PMC 5768250. PMID 29320966.
- Iyengar K, Jain VK, Vaishya R (1 September 2020). "Pitfalls in telemedicine consultations in the era of COVID 19 and how to avoid them". Diabetes & Metabolic Syndrome. 14 (5): 797–799. doi:10.1016/j.dsx.2020.06.007. PMC 7280804. PMID 32534432.
- Snoswell C, Smith AC, Scuffham PA, Whitty JA (October 2017). "Economic evaluation strategies in telehealth: Obtaining a more holistic valuation of telehealth interventions". Journal of Telemedicine and Telecare. 23 (9): 792–796. doi:10.1177/1357633x16671407. PMID 27789615. S2CID 25527349.
- Snoswell CL, Whitty JA, Caffery LJ, Loescher LJ, Gillespie N, Janda M (December 2018). "Direct-to-consumer mobile teledermoscopy for skin cancer screening: Preliminary results demonstrating willingness-to-pay in Australia". Journal of Telemedicine and Telecare. 24 (10): 683–689. doi:10.1177/1357633x18799582. PMID 30343653.
- Snoswell CL, Caffery LJ, Whitty JA, Soyer HP, Gordon LG (June 2018). "Cost-effectiveness of Skin Cancer Referral and Consultation Using Teledermoscopy in Australia". JAMA Dermatology. 154 (6): 694–700. doi:10.1001/jamadermatol.2018.0855. PMC 6145645. PMID 29801161.
- Snoswell CL, Whitty JA, Caffery LJ, Finnane A, Soyer HP (August 2019). "What do Australian dermatologists expect to be paid for store-and-forward teledermoscopy? A preliminary investigation" (PDF). Journal of Telemedicine and Telecare. 25 (7): 438–444. doi:10.1177/1357633x18776766. PMID 29933722. S2CID 49389361.
- Chausiaux O, Hayes J, Long C, Morris S, Williams G, Husheer S (2011). "Pregnancy Prognosis in Infertile Couples on the DuoFertility Programme Compared with In Vitro Fertilisation/Intracytoplasmic Sperm Injection". European Obstetrics & Gynaecology. 6 (2): 92–94.
- "Telehealth Improves Access and Quality of Care for Alaska Natives". The Innovations Exchange Team. 2013.
- Gega L, Jankovic D, Saramago P, Marshall D, Dawson S, Brabyn S, et al. (January 2022). "Digital interventions in mental health: evidence syntheses and economic modelling". Health Technology Assessment. National Institute for Health and Care Research (NIHR). 26 (1): 1–182. doi:10.3310/RCTI6942. PMC 8958412. PMID 35048909.
- Berman M, Fenaughty A (June 2005). "Technology and managed care: patient benefits of telemedicine in a rural health care network". Health Economics. Wiley. 14 (6): 559–573. doi:10.1002/hec.952. PMID 15497196.
- Van't Haaff C (March–April 2009). "Virtually On-sight" (PDF). Just for Canadian Doctors. p. 22. Archived from the original (PDF) on 2012-03-24.
- Saylor M (2012). The Mobile Wave: How Mobile Intelligence Will Change Everything. Perseus Books/Vanguard Press. p. 153. ISBN 9781593157203.
- Conde JG, De S, Hall RW, Johansen E, Meglan D, Peng GC (January–February 2010). "Telehealth innovations in health education and training". Telemedicine Journal and e-Health. 16 (1): 103–106. doi:10.1089/tmj.2009.0152. PMC 2937346. PMID 20155874.
- Best J (May 2022). "From Ukraine to remote robotics: how videoconferencing and next generation technology are transforming surgery". BMJ. 377: o1078. doi:10.1136/bmj.o1078. PMID 35504650. S2CID 248497139.
- Snoswell CL, Caffery LJ, Haydon HM, Thomas EE, Smith AC (September 2020). "Telehealth uptake in general practice as a result of the coronavirus (COVID-19) pandemic". Australian Health Review. 44 (5): 737–740. doi:10.1071/AH20183. PMID 32853536. S2CID 221357628.
- Smith AC, Thomas E, Snoswell CL, Haydon H, Mehrotra A, Clemensen J, Caffery LJ (June 2020). "Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19)". Journal of Telemedicine and Telecare. 26 (5): 309–313. doi:10.1177/1357633x20916567. PMC 7140977. PMID 32196391.
- Zhou X, Snoswell CL, Harding LE, Bambling M, Edirippulige S, Bai X, Smith AC (April 2020). "The Role of Telehealth in Reducing the Mental Health Burden from COVID-19". Telemedicine Journal and e-Health. 26 (4): 377–379. doi:10.1089/tmj.2020.0068. PMID 32202977.
- Keck CS, Doarn CR (July 2014). "Telehealth technology applications in speech-language pathology". Telemedicine Journal and E-health. 20 (7): 653–9. doi:10.1089/tmj.2013.0295. PMID 24820794.
- Paul DL. Collaborative activities in virtual settings: A knowledge management perspective of telemedicine. J Manage Inf Syst 2006;22(4):143-176.
- Cascella LM (2016). Virtual Risk: An Overview of Telehealth From a Risk Management Perspective.
- Luz PL (August 2019). "Telemedicine and the Doctor/Patient Relationship". Arquivos Brasileiros de Cardiologia. 113 (1): 100–102. doi:10.5935/abc.20190117. PMC 6684176. PMID 31411296.
- Dineen-Griffin S, Garcia-Cardenas V, Williams K, Benrimoj SI (2019-08-01). Leroyer C (ed.). "Helping patients help themselves: A systematic review of self-management support strategies in primary health care practice". PLOS ONE. 14 (8): e0220116. Bibcode:2019PLoSO..1420116D. doi:10.1371/journal.pone.0220116. PMC 6675068. PMID 31369582.
- Hibbard JH, Greene J (February 2013). "What the evidence shows about patient activation: better health outcomes and care experiences; fewer data on costs". Health Affairs. 32 (2): 207–214. doi:10.1377/hlthaff.2012.1061. PMID 23381511. S2CID 11684473.
- Hjelm NM (1 March 2005). "Benefits and drawbacks of telemedicine". Journal of Telemedicine and Telecare. 11 (2): 60–70. doi:10.1258/1357633053499886. PMID 15829049. S2CID 24145715.
- Moffatt JJ (February 2011). "Barriers to the up-take of telemedicine in Australia – a view from providers" (PDF). The University of Queensland, School of Medicine.
- Strehle EM, Shabde N (December 2006). "One hundred years of telemedicine: does this new technology have a place in paediatrics?". Archives of Disease in Childhood. 91 (12): 956–9. doi:10.1136/adc.2006.099622. PMC 2082971. PMID 17119071.
- Omboni, S., McManus, R. J., Bosworth, H. B., Chappell, L. C., Green, B. B., Kario, K., ... & Wakefield, B. J. (2020). Evidence and recommendations on the use of telemedicine for the management of arterial hypertension: an international expert position paper. Hypertension, 76(5), 1368-1383
- Daniel, H., Sulmasy, L. S., & Health and Public Policy Committee of the American College of Physicians*. (2015). Policy recommendations to guide the use of telemedicine in primary care settings: an American College of Physicians position paper. Annals of internal medicine, 163(10), 787-789.
- Dramburg, S., Walter, U., Becker, S., Casper, I., Röseler, S., Schareina, A., ... & Klimek, L. (2021). Telemedicine in allergology: practical aspects: A position paper of the Association of German Allergists (AeDA). Allergo Journal International, 30, 119-129.
- Costantino, A., Bortoluzzi, F., Giuffrè, M., Vassallo, R., Montalbano, L. M., Monica, F., ... & Elli, L. (2021). Correct use of telemedicine in gastroenterology, hepatology, and endoscopy during and after the COVID-19 pandemic: Recommendations from the Italian association of hospital gastroenterologists and endoscopists (AIGO). Digestive and Liver Disease, 53(10), 1221-1227.
- "Survey: Consumers Keen on Telemedicine". Archived from the original on 2010-04-29. Retrieved 2010-04-26.
- 2019 Best Practices in Health Care Employer Survey Highlights, Willis Towers Watson, November 5, 2019
- Trends in the Use of Telehealth During the Emergence of the COVID-19 Pandemic — United States, January–March 2020, Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report (MMWR), October 30, 2020
- Kessler SH, Schmidt-Weitmann S (February 2021). "Diseases and Emotions: An Automated Content Analysis of Health Narratives in Inquiries to an Online Health Consultation Service" (PDF). Health Communication. 36 (2): 226–235. doi:10.1080/10410236.2019.1673950. PMID 36112901. S2CID 210568504.
- Umefjord G, Sandström H, Malker H, Petersson G (February 2008). "Medical text-based consultations on the Internet: a 4-year study". International Journal of Medical Informatics. 77 (2): 114–121. doi:10.1016/j.ijmedinf.2007.01.009. PMID 17317292.
- "Willkommen am UniversitätsSpital Zürich". www.usz.ch (in Swiss High German). Archived from the original on 2020-01-17. Retrieved 2020-01-23.
- Refocusing Europe-Africa Strategy: Strategic Importance of eHealth NEPAD. Accessed 28 January 2016.
- Gerhard Bethscheider Satellite is vital for a unified, global, E-Health system September 2015 World Teleport Association. Accessed 28 January 2016.
- "Telemedicine Practice Guidelines of India".
- "The future of Telemedicine in India". Retrieved 19 May 2020.
- "Govt's telemedicine service crosses 5 million consultations". Hindustan Times. 2021-05-14. Retrieved 2021-10-10.
- Kanjo C, Jere T (May 2015). "On bringing governance into technology: Case of Internet governance and implications for Africa". 2015 IST-Africa Conference. IEEE. pp. 1–12. doi:10.1109/istafrica.2015.7190589. ISBN 978-1-9058-2451-9. S2CID 2013728.
- Geldsetzer P, Reinmuth M, Ouma PO, Lautenbach S, Okiro EA, Bärnighausen T, Zipf A (August 2020). "Mapping physical access to healthcare for older adults in sub-Saharan Africa: A cross-sectional analysis with implications for the COVID-19 response". medRxiv 10.1101/2020.07.17.20152389.
- Helping to build sustainable eHealth services in Africa SES Broadband. Company brochure. Accessed 28 January 2016.
- Wilk-Jakubowski J (2021). "A review on information systems engineering using vsat networks and their development directions". Yugoslav Journal of Operations Research. 31 (3): 409–428. doi:10.2298/yjor200215015w. S2CID 226657332.
- Caleb Henry SES Joins Clinton Global Initiative, Announces SATMED Project September 25, 2014 Satellite Today. Accessed 28 January 2016.
- Satmed Archived 2018-07-20 at the Wayback Machine Luxembourg's Development Cooperation. Accessed February 26, 2016
- E-Inclusion: Satellites Are The Answer Satellite Pro. Issue 59 February 2017. Accessed 27 June 2022
- SES SATMED ehealth platform deployed in hospital in Benin Reuters June 4, 2015. Accessed February 26, 20166
- Executive Spotlight: Gerhard Bethscheider SatMagazine November 2015. Accessed February 26, 20166
- Bashshur R, Shannon GW (2009-01-01). History of Telemedicine: Evolution, Context, and Transformation. Mary Ann Liebert. ISBN 9781934854112.
- Nakajima I, Sastrokusumo U, Mishra SK, Komiya R, Malik AZ, Tanuma T (2006-08-01). "The Asia Pacific telecommunity's telemedicine activities". HEALTHCOM 2006 8th International Conference on e-Health Networking, Applications and Services. pp. 280–282. doi:10.1109/HEALTH.2006.246471. ISBN 978-0-7803-9704-0. S2CID 28788501.
- Cuffia A (2019-01-02). "The Medical Library Association Guide to Developing Consumer Health Collections". Journal of Hospital Librarianship. 19 (1): 84–85. doi:10.1080/15323269.2019.1568127. ISSN 1532-3269. S2CID 86403514.
- Zundel KM (January 1996). "Telemedicine: history, applications, and impact on librarianship". Bulletin of the Medical Library Association. 84 (1): 71–9. PMC 226126. PMID 8938332.
- Novak M (14 March 2012). "Telemedicine Predicted in 1925". The Smithsonian Institution.
- Elizabeth, McSheffrey (2022), 'Better outcomes': B.C. organization gets American award for championing Indigenous children, Canada: Global News, retrieved 2023-08-01
- "A Brief History of Telemedicine" Archived 2007-11-24 at the Wayback Machine, Telemedicine Information Exchange website, (Accessed December 10, 2008)
- Weinstein RS, Holcomb MJ, Krupinski EA, Latifi R (2021). "First Trainees: The Golden Anniversary of the Early History of Telemedicine Education at the Massachusetts General Hospital and Harvard (1968–1970)". Telemedicine, Telehealth and Telepresence. Cham: Springer International Publishing. pp. 3–18. doi:10.1007/978-3-030-56917-4_1. ISBN 978-3-030-56916-7. S2CID 229427661.
- Allan R (28 June 2006). "A Brief History Of Telemedicine". Electronic Design.
- Buhler LH (January 2019). "Recollections of Pioneers in Xenotransplantation Research Edited by David K. C.Cooper, Nova Medicine and Health, Nova Science Publishers, New York, NY, 2018". Xenotransplantation. 26 (1): e12495. doi:10.1111/xen.12495. ISSN 0908-665X. S2CID 91740391.
- "Highlights from the Eighth Annual Meeting of the American Telemedicine Association" (Accessed December 10, 2008), Medscape website
- Harer WB (August 1979). "Tel-Med--a success story". The Western Journal of Medicine. 131 (2): 162–164. PMC 1271730. PMID 516712.
- Rovner S (7 September 1979). "Health Talk: With Tel-Med, Medical Information Is Only a Phone Call Away". The Washington Post. Retrieved 12 May 2022.
- "Tel-Med Proves Its Versatility". The San Bernardino Sun. 10 January 1973. p. 22. Retrieved 12 May 2022.
- Markman J (August 26, 2018). "NASA-Incubated Healthcare Provider Is Out Of This World". Retrieved 2019-10-06.
- Illove M (January 21, 2016). "State Prisons Turn to Telemedicine to Improve Health and Save Money". The PEW Charitable Trusts. Retrieved 2019-10-03.
- Freudenheim M (May 29, 2010). "The Doctor Will See You Now. Please Log On". The New York Times. Retrieved 2019-10-03.
- Blyth WJ (1990). Telecommunications, Concepts, Development, and Management (Second ed.). Glencoe/McCgraw-Hill. pp. 280–282. ISBN 978-0026808415.
- Goodman M (November 2016). "How the North Texas Telemedicine Revolution Began". D Magazine. Retrieved 2019-10-03.
- Dinesen B, Nonnecke B, Lindeman D, Toft E, Kidholm K, Jethwani K, et al. (March 2016). "Personalized Telehealth in the Future: A Global Research Agenda". Journal of Medical Internet Research. 18 (3): e53. doi:10.2196/jmir.5257. PMC 4795318. PMID 26932229.
- Allen A (November 8, 2017). "A hospital without patients". Politico. Retrieved 2019-10-06.
- Schiffman R (2021-02-25). "Learning to Listen to Patients' Stories". The New York Times. ISSN 0362-4331. Retrieved 2021-11-18.
- Costantino A, Noviello D, Mazza S, Berté R, Caprioli F, Vecchi M. Trust in telemedicine from IBD outpatients during the COVID-19 pandemic. Dig Liver Dis. 2021 Mar;53(3):291-294. doi: 10.1016/j.dld.2020.10.035. Epub 2020 Nov 5. PMID 33187917; PMCID: PMC7644233.
- Thomas EE, Haydon HM, Mehrotra A, Caffery LJ, Snoswell CL, Banbury A, Smith AC (May 2022). "Building on the momentum: Sustaining telehealth beyond COVID-19". Journal of Telemedicine and Telecare. 28 (4): 301–308. doi:10.1177/1357633X20960638. PMID 32985380. S2CID 222154106.
- "Telemedicine could help the world achieve health equity by bringing care to the home - here's how". World Economic Forum. 12 January 2023. Retrieved 2023-01-12.
Further reading
- "Headline Findings" (PDF). UK Department of Health Whole System Demonstrator Programme. December 2011. Results from clinical trial carried out by the UK Government's Department of Health
- "Telemedicine, Telehealth, and the Consumer". Telemedicine Information Exchange. Online introduction and primer to telehealth and telemedicine
- Norris AC (2002). Essentials of Telemedicine and Telecare. West Sussex, England; New York: John Wiley & Sons, Ltd. ISBN 0-471-53151-0.
- Maheu MM, Whitten P, Allen A (2001). E-Health, Telehealth, and Telemedicine: A Guide to Start-up and Success. San Francisco: Jossey Bass. ISBN 0-7879-4420-3.
- Olmeda CJ (2000). Information Technology in Systems of Care. Delfin Press. ISBN 978-0-9821442-0-6.
- Burgess SG. "Telehealth Technical Assistance Manual" (PDF). - A document to assist in the planning of telehealth and telemedicine projects for rural community and migrant health centers and other health care organizations.
- Gärtner A. "Teleneurology and requirements of the European Medical Devices Directive (MDD)". Telemedical Systems and regulatory affairs for Europe. Archived from the original on 2012-02-16. Retrieved 2009-04-02.
- Gilman M, Stensland J (2013). "Telehealth and Medicare: payment policy, current use, and prospects for growth". Medicare & Medicaid Research Review. 3 (4): E1–E17. doi:10.5600/mmrr.003.04.a04. PMC 4011650. PMID 24834368.
External links
![]() Media related to Telemedicine at Wikimedia Commons
Media related to Telemedicine at Wikimedia Commons
| History |
| |
|---|---|---|
| Pioneers |
| |
| Transmission media | ||
| Network topology and switching | ||
| Multiplexing | ||
| Concepts | ||
| Types of network | ||
| Notable networks | ||
| Locations |
| |
| ||