Anomalous pulmonary venous connection
Anomalous pulmonary venous connection (or anomalous pulmonary venous drainage or anomalous pulmonary venous return[1]) is a congenital defect of the pulmonary veins.
| Anomalous pulmonary venous connection | |
|---|---|
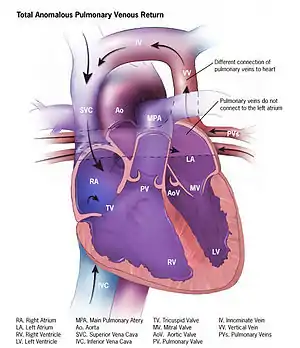 | |
| Illustration of total anomalous pulmonary venous connection | |
| Specialty | Medical genetics |
Total anomalous pulmonary venous connection
Total anomalous pulmonary venous connection, also known as total anomalous pulmonary venous return, is a rare cyanotic congenital heart defect in which all four pulmonary veins are malpositioned and make anomalous connections to the systemic venous circulation. (Normally, pulmonary veins return oxygenated blood from the lungs to the left atrium where it can then be pumped to the rest of the body). A right-to-left shunt such as a patent foramen ovale, patent ductus arteriosus or an atrial septal defect must be present, or else the condition is fatal due to a lack of systemic blood flow.
In some cases, it can be detected prenatally.[2]
There are four variants: Supracardiac (50%): blood drains to one of the innominate veins (brachiocephalic veins) or the superior vena cava; Cardiac (20%), where blood drains into coronary sinus or directly into right atrium; Infradiaphragmatic (20%), where blood drains into portal or hepatic veins; and a mixed (10%) variant.
TAPVC can occur with obstruction, which occurs when the anomalous vein enters a vessel at an acute angle and can cause pulmonary venous hypertension and cyanosis because blood cannot enter the new vein as easily.
Signs and symptoms
- right ventricular heave
- Loud S1
- fixed split S2
- S3 gallop
- systolic ejection murmur at left upper sternal border
- cardiomegaly
- right axis deviation on ECG
- Snowman sign or 'figure of 8 configuration' on chest radiograph
- right ventricular hypertrophy
- cyanosis, tachypnea, dyspnea since the overloaded pulmonary circuit can cause pulmonary edema
- Cottage-loaf sign, that is, chest X-ray appearance similar to a cottage loaf, also known as the 'snow man' sign or 'figure of 8' sign.[3]
Treatment
In TAPVC without obstruction, surgical redirection can be performed within the first month of life. The operation is performed under general anesthesia. The four pulmonary veins are reconnected to the left atrium, and any associated heart defects such as atrial septal defect, ventricular septal defect, patent foramen ovale, and/or patent ductus arteriosus are surgically closed. With obstruction, surgery should be undertaken emergently. PGE1 should be given because a patent ductus arteriosus allows oxygenated blood to go from the circulation of the right heart to the systemic circulation.
Partial anomalous pulmonary venous connection
A Partial anomalous pulmonary venous connection (or Partial anomalous pulmonary venous drainage or Partial anomalous pulmonary venous return) is a congenital defect where the left atrium is the point of return for the blood from some (but not all) of the pulmonary veins.
It is less severe than total anomalous pulmonary venous connection which is a life-threatening anomaly requiring emergent surgical correction, usually diagnosed in the first few days of life. Partial anomalous venous connection may be diagnosed at any time from birth to old age. The severity of symptoms, and thus the likelihood of diagnosis, varies significantly depending on the amount of blood flow through the anomalous connections. In less severe cases, with smaller amounts of blood flow, diagnosis may be delayed until adulthood, when it can be confused with other causes of pulmonary hypertension.[4] There is also evidence that a significant number of mild cases are never diagnosed, or diagnosed incidentally.[5] It is associated with other vascular anomalies, and some genetic syndromes such as Turner syndrome.
Diagnosis
It can be diagnosed with CT scan, angiography, transesophageal echocardiography, or cardiac MRI.[6][7] Unfortunately, less invasive and expensive testing, such as transthoracic echocardiography and CT scanning are generally less sensitive.
References
- "Facts about Total Anomalous Pulmonary Venous Return or TAPVR". Retrieved November 10, 2013.
- Allan LD, Sharland GK (April 2001). "The echocardiographic diagnosis of totally anomalous pulmonary venous connection in the fetus". Heart. 85 (4): 433–7. doi:10.1136/heart.85.4.433. PMC 1729686. PMID 11250972.
- Somerville J, Grech V (2009). "The chest x-ray in congenital heart disease 1. Total anomalous pulmonary venous drainage and coarctation of the aorta". Images Paediatr Cardiol. 11 (1): 7–9. ISSN 1729-441X. PMC 3232600. PMID 22368552.
- Sears EH, Aliotta JM, Klinger JR. Partial anomalous pulmonary venous return presenting with adult-onset pulmonary hypertension. Pulm Circ 2012;2:250-5.
- Ho ML, Bhalla S, Bierhals A, Gutierrez F. MDCT of partial anomalous pulmonary venous return (PAPVR) in adults. J Thorac Imaging 2009;24:89-95.
- Prasad SK, Soukias N, Hornung T, Khan M, Pennell DJ, Gatzoulis MA, et al. (2004). "Role of magnetic resonance angiography in the diagnosis of major aortopulmonary collateral arteries and partial anomalous pulmonary venous drainage". Circulation. 109 (2): 207–14. doi:10.1161/01.cir.0000107842.29467.c5. PMID 14718402.
- Ammash NM, Seward JB, Warnes CA, Connolly HM, O'Leary PW, Danielson GK (May 1997). "Partial anomalous pulmonary venous connection: diagnosis by transesophageal echocardiography". J. Am. Coll. Cardiol. 29 (6): 1351–8. doi:10.1016/S0735-1097(97)82758-1. PMID 9137235.
- ElBardissi AW, Dearani JA, Suri RM, Danielson GK (March 2008). "Left-sided partial anomalous pulmonary venous connections". Ann. Thorac. Surg. 85 (3): 1007–14. doi:10.1016/j.athoracsur.2007.11.038. PMID 18291189.
- Alsoufi B, Cai S, Van Arsdell GS, Williams WG, Caldarone CA, Coles JG (December 2007). "Outcomes after surgical treatment of children with partial anomalous pulmonary venous connection". Ann. Thorac. Surg. 84 (6): 2020–6, discussion 2020–6. doi:10.1016/j.athoracsur.2007.05.046. PMID 18036929.