Pelvic organ prolapse
Pelvic organ prolapse (POP) is characterized by descent of pelvic organs from their normal positions into the vagina. In women, the condition usually occurs when the pelvic floor collapses after gynecological cancer treatment, childbirth or heavy lifting.[2] Injury incurred to fascia membranes and other connective structures can result in cystocele, rectocele or both. Treatment can involve dietary and lifestyle changes, physical therapy, or surgery.[3]
| Pelvic organ prolapse | |
|---|---|
| Other names | Female genital prolapse |
 | |
| A 40 year old woman with uterine prolapse, which is visible only in standing position, with the cervix protruding through the vulva. | |
| Specialty | Gynecology |
| Frequency | 316 million women (9.3% as of 2010)[1] |
Types

_(14597977337).jpg.webp)
- Anterior vaginal wall prolapse
- Cystocele (bladder into vagina)
- Urethrocele (urethra into vagina)
- Cystourethrocele (both bladder and urethra)
- Posterior vaginal wall prolapse
- Enterocele (small intestine into vagina)
- Rectocele (rectum into vagina)
- Sigmoidocele
- Apical vaginal prolapse
- Uterine prolapse (uterus into vagina)[4]
- Vaginal vault prolapse (descent of the roof of vagina) – after surgical removal of the uterus hysterectomy[5]

Grading
Pelvic organ prolapses are graded either via the Baden–Walker System, Shaw's System, or the Pelvic Organ Prolapse Quantification (POP-Q) System.[6]
Shaw's System
Anterior wall
- Upper 2/3 cystocele
- Lower 1/3 urethrocele
Posterior wall
- Upper 1/3 enterocele
- Middle 1/3 rectocele
- Lower 1/3 deficient perineum
Uterine prolapse
- Grade 0 Normal position
- Grade 1 descent into vagina not reaching introitus
- Grade 2 descent up to the introitus
- Grade 3 descent outside the introitus
- Grade 4 Procidentia
Baden–Walker
| Grade | Posterior urethral descent, lowest part other sites |
|---|---|
| 0 | normal position for each respective site |
| 1 | descent halfway to the hymen |
| 2 | descent to the hymen |
| 3 | descent halfway past the hymen |
| 4 | maximum possible descent for each site |
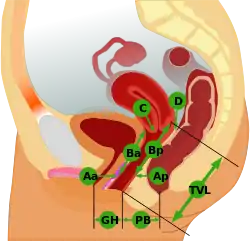
POP-Q
| Stage | Description |
|---|---|
| 0 | No prolapse anterior and posterior points are all −3 cm, and C or D is between −TVL and −(TVL−2) cm. |
| 1 | The criteria for stage 0 are not met, and the most distal prolapse is more than 1 cm above the level of the hymen (less than −1 cm). |
| 2 | The most distal prolapse is between 1 cm above and 1 cm below the hymen (at least one point is −1, 0, or +1). |
| 3 | The most distal prolapse is more than 1 cm below the hymen but no further than 2 cm less than TVL. |
| 4 | Represents complete procidentia or vault eversion; the most distal prolapse protrudes to at least (TVL−2) cm. |
Management
Vaginal prolapses are treated according to the severity of symptoms.
Non-surgical
With conservative measures, such as changes in diet and fitness, Kegel exercises, and pelvic floor physical therapy.[8]
A pessary, a rubber or silicone rubber device fitted to the patient is also a non-surgical option, it is inserted into the vagina and may be retained for up to several months. Vaginal pessaries can immediately relieve prolapse and prolapse-related symptoms.[9] Pessaries are a good choice of treatment for women who wish to maintain fertility, are poor surgical candidates, or who may not be able to attend physical therapy.[10] Pessaries require a provider to fit the device, but most can be removed, cleaned, and replaced by the woman herself. Pessaries should be offered as a non-surgical alternative for women considering surgery.
Surgery
Surgery (for example native tissue repair, biological graft repair, absorbable and non-absorbable mesh repair, colpopexy, or colpocleisis) is used to treat symptoms such as bowel or urinary problems, pain, or a prolapse sensation. When operating a pelvic organ prolapse, introducing a mid-urethral sling during or after surgery seems to reduce stress urinary incontinence.[11] Transvaginal repair seems to be more effective than transanal repair in posterior wall prolapse, but adverse effects cannot be excluded.[12] According to the FDA, serious complications are "not rare."[13]
Evidence does not support the use of transvaginal surgical mesh compared with native tissue repair for anterior compartment prolapse owing to increased morbidity.[14] For posterior vaginal repair, the use of mesh or graft material does not seem to provide any benefits.[12]
Compared to native tissue repair, transvaginal permanent mesh likely reduces both the perception of vaginal prolapse sensation, and the risk of recurrent prolapse and of having repeat surgery for prolapse. However, transvaginal mesh (TVM) has a greater risk of bladder injury and of needing repeat surgery for stress urinary incontinence or mesh exposure.[15] Also, the use of a TVM in treating vaginal prolapses is associated with side effects including pain, infection, and organ perforation.
Safety and efficacy of many newer meshes is unknown.[14] Thousands of class action lawsuits have been filed and settled against several manufacturers of TVM devices.[16]
For surgical treatment of apical vaginal prolapse, going through the abdomen (sacral colpopexy) may have better outcomes than a surgical approach that goes through the vagina.[5]
Epidemiology
Genital prolapse occurs in about 316 million women worldwide as of 2010 (9.3% of all females).[1]
Research
To study POP, various animal models are employed: non-human primates, sheep,[17][18] pigs, rats, and others.[19][20]
See also
References
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. (December 2012). "Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010". Lancet. 380 (9859): 2163–2196. doi:10.1016/S0140-6736(12)61729-2. PMC 6350784. PMID 23245607.
- Ramaseshan AS, Felton J, Roque D, Rao G, Shipper AG, Sanses TV (April 2018). "Pelvic floor disorders in women with gynecologic malignancies: a systematic review". International Urogynecology Journal. 29 (4): 459–476. doi:10.1007/s00192-017-3467-4. PMC 7329191. PMID 28929201.
- "Pelvic organ prolapse". womenshealth.gov. 2017-05-03. Retrieved 2017-12-29.
- Donita D (2015-02-10). Health & physical assessment in nursing. Barbarito, Colleen (3rd ed.). Boston. p. 665. ISBN 978-0-13-387640-6. OCLC 894626609.
{{cite book}}: CS1 maint: location missing publisher (link) - Maher, Christopher; Yeung, Ellen; Haya, Nir; Christmann-Schmid, Corina; Mowat, Alex; Chen, Zhuoran; Baessler, Kaven (2023-07-26). "Surgery for women with apical vaginal prolapse". The Cochrane Database of Systematic Reviews. 2023 (7): CD012376. doi:10.1002/14651858.CD012376.pub2. ISSN 1469-493X. PMC 10370901. PMID 37493538.
- ACOG Committee on Practice Bulletins—Gynecology (September 2007). "ACOG Practice Bulletin No. 85: Pelvic organ prolapse". Obstetrics and Gynecology. 110 (3): 717–729. doi:10.1097/01.AOG.0000263925.97887.72. PMID 17766624.
- Beckley I, Harris N (2013-03-26). "Pelvic organ prolapse: a urology perspective". Journal of Clinical Urology. 6 (2): 68–76. doi:10.1177/2051415812472675. S2CID 75886698.
- "Kegel Exercises | NIDDK". National Institute of Diabetes and Digestive and Kidney Diseases. Retrieved 2017-12-02.
- Boyd, S.S.; Propst, K.; O'Sullivan, D.M.; Tulikangas, P. (March 2019). "25: Pessary use and severity of pelvic organ prolapse over time: a retrospective study". American Journal of Obstetrics and Gynecology. 220 (3): S723. doi:10.1016/j.ajog.2019.01.055. ISSN 0002-9378. S2CID 86740242.
- Tulikangas P, et al. (Committee on Practice Bulletins—Gynecology and the American Urogynecologic Society) (April 2017). "Practice Bulletin No. 176: Pelvic Organ Prolapse". Obstetrics and Gynecology. 129 (4): e56–e72. doi:10.1097/aog.0000000000002016. PMID 28333818. S2CID 46882949.
- Baessler K, Christmann-Schmid C, Maher C, Haya N, Crawford TJ, Brown J (19 August 2018). "Surgery for women with pelvic organ prolapse with or without stress urinary incontinence". Cochrane Database Syst Rev. 2018 (8): CD013108. doi:10.1002/14651858.CD013108. PMC 6513383. PMID 30121956.
- Mowat A, Maher D, Baessler K, Christmann-Schmid C, Haya N, Maher C (5 March 2018). "Surgery for women with posterior compartment prolapse". Cochrane Database Syst Rev. 2018 (3): CD012975. doi:10.1002/14651858.CD012975. PMC 6494287. PMID 29502352.
- "UPDATE on Serious Complications Associated with Transvaginal Placement of Surgical Mesh for Pelvic Organ Prolapse: FDA Safety Communication". U.S. Food and Drug Administration. 13 July 2011. Retrieved 23 June 2015.
- Maher C, Feiner B, Baessler K, Christmann-Schmid C, Haya N, Brown J (November 2016). "Surgery for women with anterior compartment prolapse". The Cochrane Database of Systematic Reviews. 2017 (11): CD004014. doi:10.1002/14651858.CD004014.pub6. PMC 6464975. PMID 27901278.
- Maher, C; Feiner, B; Baessler, K; Christmann-Schmid, C; Haya, N; Marjoribanks, J (9 February 2016). "Transvaginal mesh or grafts compared with native tissue repair for vaginal prolapse". The Cochrane Database of Systematic Reviews. 2 (2): CD012079. doi:10.1002/14651858.CD012079. PMC 6489145. PMID 26858090.
- Michelle Llamas, BCPA (2022-11-11). "Transvaginal Mesh Lawsuits". drugwatch. Retrieved 2023-01-16.
- Patnaik SS, Brazile B, Dandolu V, Damaser M, van der Vaart CH, Liao J. "Sheep as an animal model for pelvic organ prolapse and urogynecological research" (PDF). ASB 2015 Annual Conference 2015. Archived from the original (PDF) on 2019-03-27. Retrieved 2019-03-26.
- Patnaik SS (2015). Investigation of sheep reproductive tract as an animal model for pelvic organ prolapse and urogyencological research. Mississippi State University.
- Couri BM, Lenis AT, Borazjani A, Paraiso MF, Damaser MS (May 2012). "Animal models of female pelvic organ prolapse: lessons learned". Expert Review of Obstetrics & Gynecology. 7 (3): 249–260. doi:10.1586/eog.12.24. PMC 3374602. PMID 22707980.
- Patnaik SS (2016). Chapter Six - Pelvic Floor Biomechanics From Animal Models. Academic Press. pp. 131–148. doi:10.1016/B978-0-12-803228-2.00006-4.